

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Orofacial trauma that causes injury to the alveolar ridge is extremely rare, prior to the eruption of primary anterior teeth. Orofacial trauma occurs as infants begin to crawl, its incidence rises as infants begin to walk, and peaks at 2–3 years of age when children become increasingly active [123]. For these reasons, trauma that occurs prior to the eruption of the primary anterior teeth may definitely have an impact, although it is often neglected as an etiology of the abnormalities of the deciduous dentition [4]. Orotracheal intubation can be one of the most common causes of injury prior to primary tooth eruption.
Several low-weight premature infants require surgery or incubator care, owing to multiple medical problems. They are unprepared for extra-uterine life and have immaturely developed brain, lungs, and eyes [56]. Several premature infants need intubation due to incomplete lung development [7], and 1 of 500 newborn babies may need intubation at birth [8].
Endotracheal intubation is a rapid, safe, simple, and non-surgical technique, which is the gold-standard for airway management, since its advantages include promoting airway patency and preventing pulmonary aspiration [9].
However, pharyngeal, esophageal, and tracheal trauma or perforation; intubation of the mainstem bronchus; subglottic stenosis; accidental extubation; post-extubation atelectasis; respiratory infection; erosion of the nares or septum; and injury to the maxillary anterior alveolar ridge and developing tooth germs may occur during the intubation process [10]. Orotracheal tubes used to prevent septal and respiratory impairment caused by a nasotracheal tube, may have an impact on oral tissue development [1112].
Various complications of orotracheal intubation in infants have been documented in the literature (Tables 1 and 2), including acute [13141516] and chronic trauma [17] to the hypopharyngeal structures, systemic [181920], and local [21] side effects, and deleterious effects on oral development [22232425]. Delayed eruption, ectopic impaction, and tooth malformation following orotracheal intubation are reportedly caused by displacement and localized trauma to the tooth germ [42627]. Moreover, acquired cleft palate, alveolar grooving, palatal grooving, palataldepth and width asymmetry, crossbite, and dental defects may occur as a result of orotracheal intubation [28].
Deformation or enamel defect is a classical dental abnormality of the primary teeth. The mineralization of primary incisors commences at 4 months after birth, and crown mineralization is completed at 6 months. On the other hand, mineralization of primary molars commences at the end of 5 months and is completed about 1 year after delivery. Trauma to the region of the developing tooth germ during this period may result in dental anomalies [29]. Enamel hypoplasia is reportedly observed in about 18–80% of preterm or other medically compromised premature infants, who underwent neonatal intubation [3031].
Despite medical and dental research on the relationship between orotracheal intubation and developmental changes, it is still difficult to clearly determine whether the impact on orofacial tissues is related to preterm birth or extrinsic factors such as orotracheal intubation [32].
ALVEOLAR AND PALATAL GROOVES
Among the preterm infants, who underwent orotracheal intubation, 23.1% showed changes in the alveolar contour [32]. Erenberg and Nowak [24] reported the association between a higher incidence of palatal grooving and neonatal intubation. According to Boice et al. [38], a prominent concavity was observed on the left maxillary alveolar ridge in non-surviving low birth-weight infants, who underwent orotracheal intubation. Moreover, severe developmental defects of the enamel organ were observed in this area.
In another study, indentation of the anterior ridge was observed in infants who were mechanically ventilated following intubation, due to continuous force exerted by the tube [3339].
Intraoral protective devices have been used with orotracheal intubation tubes, to prevent alveolar or palatal deformation caused by intubation. [4041] These appliances were designed to protect the oral tissue from pressure exerted by the tube [4243]. Fadavi et al. [44] performed a randomized prospective study with 26 infants who had undergone orotracheal intubation from day 7 to 109 of birth, with birth weights of 540–1,470 g. While the control group showed 2–5-mm palatal grooves, preterm infants in whom a protective device was used did not exhibit palatal grooves.
DEFECTIVE DEVELOPMENT OF ENAMEL
Defective development of enamel (DDE) may manifest as a defective area on the enamel surface or an incompletely formed crown (Fig. 1).
Compared to premature infants who had not undergone intubation, DDE was 6 times more prevalent among premature infants who underwent orotracheal intubation. Of 157 premature infants, 77 infants underwent intubation and 80 did not. Fifty-one infants exhibited DDE, 44 of whom were intubated. while 7 had not undergone intubation. Of the 77 intubated infants, 44 (57%) showed DDE, and 7 (9%) of 80 non-intubated infants exhibited DDE. Furthermore, a total of 177 teeth with DDE were observed in 51 infants, which was markedly more common in the maxilla (80.2%) than in the mandible (19.8%) [34].
Another study reported that defects in maxillary incisors were observed in 85% of intubated infants. The mean birth weight of 63 low-weight infants was 1154 g, with a range from 605 g–1500 g. Of these, 40 infants underwent endotracheal intubation, and 34 (85%) had enamel defects in the maxillary anterior teeth. Of the 23 non-intubated infants, only 5 (21.7%) showed DDE in the maxillary anterior teeth [35].
TOOTH MALFORMATION
A patient underwent multiple orotracheal intubations for six rounds of surgery, starting from 9 days to 4 years of age, due to a complex cardiac abnormality. The patient's primary maxillary right central incisor had not erupted till 3 years of age, and the contralateral primary incisor did not erupt till 6 years and 10 months of age. In addition to delayed eruption, the maxillary deciduous incisor exhibited abnormal morphology, enamel hypoplasia, and abnormal dentine formation [27].
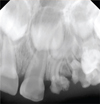
A 2-year-old girl visited the clinic with a chief complaint of an unerupted primary maxillary left incisor. The patient born prematurely at a gestational age of 25 weeks and 6 days, with a birth weight of 830 g. She had undergone orotracheal intubation and was placed in an incubator for about 5 months, due to neonatal respiratory distress syndrome. Clinical examination revealed that the primary maxillary left lateral incisor and canine had not erupted, and radiography revealed malformation, delayed eruption, and dilacerations of the roots of the corresponding teeth (Fig. 2, 3). During a periodic follow-up, no spontaneous pain and clinical abnormalities were observed in the malformed teeth. No abnormal findings were observed in the developing permanent teeth [45].
A 16-month-old boy visited the clinic with a chief complaint of an erupted maxillary primary incisor with an abnormal morphology. The patient was born prematurely, at a gestational age of 25 weeks and 4 days, with a birth weight of 880 g. Orotracheal intubation was maintained for about 2 months, with 3 months of incubator care, due to bronchopulmonary dysplasia and neonatal respiratory distress syndrome. Clinical examination revealed delayed eruption of the primary maxillary left lateral incisor and canine, and radiography revealed malformation of the same teeth (Fig. 2, 3) [45].
DISPLACEMENT OF THE TOOTH GERM
A 16-month-old girl visited the clinic with a chief complaint of delayed eruption of a deciduous incisor. The patient was born prematurely, at a gestational age of 24 weeks, with a birth weight of 480 g. She had undergone patent ductus arteriosus surgery at 1 month of age, and surgery under general anesthesia at 4 months of age, for hernia and retinal detachment and at 8 months for another retinal detachment. Oral examination revealed that the maxillary right primary incisor and mandibular incisor were erupted, but the maxillary left primary incisor was unerupted. No abnormal findings were observed with the erupted primary tooth, and radiography revealed suspected maxillary primary left central incisor malformation and primary central and lateral incisor displacement. Computed tomography (CT) was performed under sedation during the periodic follow-up two months later, with the caregiver's consent. CT revealed displacement of the maxillary left primary central, lateral incisor, and canine tooth germs, with malformation of the primary left incisor. The patient had no systemic disease associated with delayed eruption, and only had a history of multiple orotracheal intubations prior to the eruption of the primary anterior teeth, due to various medical issues related to premature birth. Furthermore, considering that the delayed eruption, malformation, and displacement of tooth germs were localized to the left maxilla, these findings can probably be attributed to a local factor. [46]
Although the displacement of a dental follicle cannot be detected during clinical examination, it is often accompanied ectopic or delayed eruption.
PALATAL SHAPE
Deformation may be caused by the application of unbalanced and continuous mechanical forces to malleable tissues [36]. During the early stage of development of the oral cavity, the palatal bone is malleable and is easily influenced by extrinsic force [47]. Deformation of the median palatine suture may occur due to prolonged orotracheal intubation, since the endotracheal tube exerts continuous pressure on the palate [36374849].
Neonatal intubation lasting for more than 10 days has been reported to induce palatal deformation in infants. This is thought to be a result of direct pressure caused to the median palatine suture by the orotracheal tube [36]; 12% of preterm infants who underwent neonatal intubation exhibited palatal deformation [32].
Another study on the effects of orotracheal intubation on the palatal architecture in preterm infants classified the palatal shape of neonates into square, narrow, and ovoid. A narrow palate (67.6%) was more frequently observed than the square (14.7%) or ovoid (17.7%) morphology in neonates who had undergone intubation for 7 days or longer [37]. The narrow palatal morphology is maintained even after the patient has fully grown (Fig. 4).
Ash et al. [40] assessed the effect of using protective palate plates in preterm infants. They investigated 15 non-intubated infants (control group) and 30 intubated infants born before 32 weeks of gestation, in whom intubation was maintained for at least 10 days and the use of palate plate was randomly controlled. Compared to the non-intubated infants, infants in whom the palatal plate was not used, had a smaller, deeper, and narrower palate. When the plate was used, a reduction of the narrowing and depth of palate was observed in the intubated infants. Palatal plates did not interfere with the lateral growth of the infant's palate or harm other oral tissues.
ACQUIRED ORAL COMMISSURE DEFECT
An oral commissure defect caused by prolonged endotracheal intubation is rarely reported. Infants born at 23 weeks of gestation underwent neonatal intubation after birth for mechanical ventilation and had histories of respiratory distress syndrome, sepsis, pneumonia, patent ductus arteriosus, tracheitis, anemia, thrombocytopenia, inguinal hernia, and chronic pneumatocele. On day 72 after a 3.5-mm endotracheal tube (ETT) intubation, a circular lesion was discovered on the left side of the mouth while replacing the ETT holder. The lesion, which occurred in the oral commissure area, was clean and smooth, without active bleeding, with minimal reactive inflammation [22].
TEMPOROMANDIBULAR JOINT INJURY
Temporomandibular joint (TMJ) injury is very rare but severe. Increased force may cause a rupture of the lateral ligament, while locating the glottis during laryngoscopy. This can reportedly lead to limited mouth opening, joint pain, lateral deviation of the mandible, and protrusion of the mandible [9].
TONGUE INJURY
Compression due to prolonged endotracheal intubation may induce ischemia or venous congestion and ultimately cause macroglossia. Obstruction of the submandibular duct by the ETT may lead to massive tongue swelling. Furthermore, compression injury inflicted during the intubation process has been reported to cause lingual nerve injury [927]. Transient tongue weakness, numbness, or paralysis following laryngoscopy may cause compression of the hypoglossal nerves [50]. In addition to transient tongue damage, cases of uvula injury, sore throat, odynophagia, coughing, and serious life-threatening airway obstruction have also been reported [51].
SIMULTANEOUS OCCURRENCES
As described in this paper, orotracheal intubation in preterm infants can have complex effects as opposed to a single effect on oral tissue development. According to the study by Alves et al. [32], alveolar contour was strongly associated with crossbite and eruption sequence, while palatal form and crown color showed a statistically significant correlation. Kopra and Davis reported that intubated children frequently exhibited a high palatal vault, palatal grooves, and posterior crossbite compared to the non-intubated control group, and such complex oral abnormalities may induce speech impairments [28].
REASONS FOR LEFT MAXILLARY PREDILECTION
The reason for the localization of injuries to the developing left maxillary primary anterior teeth may be explained by the endotracheal intubation and laryngoscope process. In an ideal examination process, no abnormal force should be applied during intubation and laryngoscopy, which may affect the anterior alveolar bone. However, inadvertent force may be applied to the left maxillary alveolar bone, while manipulating the device in low-birth weight infants. Moreover, the developing tooth germ may be more sensitive to external stimulation in very low-birth weight infants, because the cortical bone is thinner due to osteopenia [35]. According to a previous report, 86 out of 142 maxillary primary teeth with DDE were primary left incisors (61%), which implies that DDE has a predilection for the left side [34]. Another study also reported 44 maxillary anterior teeth with defects in 40 intubated children, of which 13 teeth (30%) were primary right incisors, while 31 (70%) were primary left incisors [35].
CONCLUSION
Although this study discussed the adverse effects of endotracheal intubation on oral development, intubation is essential for the survival of preterm infants. Protective devices have been developed to decrease the side-effects of intubation. However, impression making prior to orotracheal intubation may be difficult and the use of protective appliances may be restricted depending on the medical situation.
Orotracheal intubation tubes may cause dental malformation, enamel defects, displacement of the tooth germ, delayed eruption, and oral tissue development, and it may affect the permanent and primary dentitions. Therefore, periodic follow-ups are essential for reevaluation and comprehensive treatment planning, and dentists are responsible for actively intervening in this process and guiding guardians about the child's oral health care needs.





 XML Download
XML Download