

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Schwannomas are the most common primary intraspinal tumor, accounting for 30% of primary spinal neoplasm [1]. They are commonly intradural extramedullary in location. These tumors may be incidentally diagnosed on imaging, and delayed diagnosis is common because of slow growth [2]. Symptoms are related to the radicular and/or spinal cord levels affected by the tumor [3]. The acute hemorrhagic onset of a spinal schwannoma is a rare occurrence and intratumoral hemorrhage may result in rapid neurological deterioration. An MRI scan is useful for detecting hemorrhagic changes associated with intraspinal tumors. Total surgical resection is the goal of treatment to relieve symptoms and prevent recurrence.
We report a case of cervical schwannoma with acute intratumoral hemorrhage, presenting with an acute onset of quadriparesis.
CASE REPORT
A 37-year-old male patient presented with complaint of neck pain and acute onset of quadripresis after physical therapy. On admission, the motor examination revealed grade 0/5 and 4/5 powers in the right and left side limbs, respectively; sensory examination showed decreased pain sensation in the left side limbs and decreased touch sensation in the right side limbs. There was no history of trauma, but cervical myelopathy was suspected. The MRI of the cervical spine revealed a hemorrhagic intradural extramedullary lesion extending to the right side of the spinal cord at C2 to C3 vertebral levels (Fig. 1).
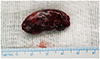
The patient underwent an emergency operation, where right hemilaminectomy from C2 to C3 was done. After opening the dura, an ovoid dark-reddish hemorrhagic extramedullary mass was seen. The spinal cord was compressed and displaced toward the left side. The mass was well-defined and attached to the right C2 nerve root. Dissection was easily achieved, and en-bloc removal of the lesion was done (Fig. 2). The hematoxylin and eosin (H&E) sections of the lesion revealed a moderately cellular neoplastic lesion composed of spindle shaped cells in fascicles with nuclear palisading resembling a Verocay body. Overall histopathological features were suggestive of an ancient schwannoma with intratumoral hemorrhage (Fig. 3). Postoperative spine MRI T2-weighted imaging (WI) showed complete excision of the tumor (Fig. 4). The postoperative period was uneventful. The motor and sensory functions of the patient had gradually improved. At postoperative 3 weeks, there were grade 4/5 and 5/5 powers in right and left side limbs, respectively, and patient was ambulant without support.
This presenting case report was conducted according to guidelines of the Declaration of Helsinki for biomedical research. Informed consent was waived due to its retrospective nature.
DISCUSSION
Schwannomas account for around one-third of all primary spinal tumors, occurring equally in both sexes [456]. Their common locations include intradural extramedullary sites (58%), followed by extradural (27%), dumbbell shaped tumors with both an extradural and an intradural component (15%), and rarely intramedullary (less than 1%) [7]. Delayed diagnosis is common because spinal schwannoma usually has a low growth rate. The symptoms depend on the size and location of the tumor and are related to a slowly enlarging mass with pressure effects or sensory changes in the distributing area of the affected nerve [8].
The most frequent symptom related to intradural schwannoma is pain [9]. The intradural schwannoma with acute intratumoral hemorrhage is a very rare occurrence and presents early due to the rapid onset of neurological deficit [10]. The exact mechanism of acute intratumoral hemorrhage in schwannomas is not known. There are 2 possible underlying conditions that can be considered: the first theory suggests that hyalinized ectatic vessels inside the schwannoma undergo spontaneous thrombosis resulting in distal necrosis and hemorrhage; and the second theory supports the traction of tumor vasculature during movement [11]. A history of anticoagulant/antiplatelet therapy or trauma may cause acute intratumoral hemorrhage.
An MRI scan is the preferred imaging modality for detecting hemorrhages associated with spinal tumors. The signal intensities of hemorrhagic spinal tumor can be influenced by the stages of hemorrhage. Schwannomas usually present with an intense, homogenous enhancement with gadolinium contrast. However, those with tumoral hemorrhage usually show irregular enhancement due to concomitant presence of blood products [12].
The definite diagnosis of spinal schwannoma depends on the histopathological examination. The histological stains show a mixture of 2 growth patterns such as the Antoni A and Antoni B. In the Antoni A pattern, nuclear palisading and associated Verocay bodies with a prominent extracellular matrix and secretion of laminin are the dominant characteristics; whereas, a loose organization with myxomatous and cystic changes are the main features of Antoni B [13]. The major histopathological characteristics of the ancient schwannoma, a rare sub-type of schwannomas, are degenerative changes such as cyst formation, calcification with occasional sites of hemorrhage, and sparse mitotic hyperchromatic nuclei [14].
The complete excision of the tumor, along with its capsule, is the gold standard in the treatment of cervical schwannomas. Early diagnosis and emergency operation are factors responsible for successful outcome in the case of hemorrhagic schwannoma [15]. The prognosis is good, and tumors do not typically recur [8].
In conclusion, spinal schwannomas presenting with intratumoral hemorrhage is a rare event. Early diagnosis and emergency management should be considered in cervical pathologies with rapid progression of neurological symptoms. A contrast enhanced MRI is the gold standard diagnostic modality for intraspinal tumors. The complete excision of hemorrhagic tumor is the goal of treatment to prevent recurrence.



 XML Download
XML Download