

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Ependymoma is rare central nervous system tumor arising from ependymal cells lining the central canal of the spinal cord and ventricle of brain. They may occur supratentorial and posterior fossa, and spinal canal. As intracranial ependymoma is mainly a tumor of children, it makes up a 2% of adult intracranial tumors and 10% of the child ones [1]. Preferentially ependymoma of children is located at posterior fossa, whereas in adult, the tendency was less intensive and ependymoma is found often at supratentorial location [2]. Thus, posterior fossa ependymoma is extremely rare intracranial tumor in adults, especially in the elderly, and even up to one-third of pathologic diagnosis was mistaken to other tumors [1]. Histological grade and the extent of surgical resection were known to be significant for patients' prognosis [134]. High-grade ependymoma prevailed among pediatric patients, and supratentorial location. Although infratentorial ependymoma in adults was known to be preferentially low grade (83% of WHO grade II), there is no consensus of treatment especially those found incidentally, especially in elderly patient.
Go to : 
CASE REPORT
A 68-year-old woman diagnosed with ovarian cancer referred to neurosurgical department from gynecologic department for abnormal finding of brain MRI, which was performed as a check-up before radical surgery of ovarian cancer in 2012. She had a past medical history of surgical clipping of ruptured anterior communicating artery aneurysm with subarachnoid hemorrhage, and subsequent ventriculo-peritoneal shunt due to post hemorrhagic hydrocephalus in 2005.
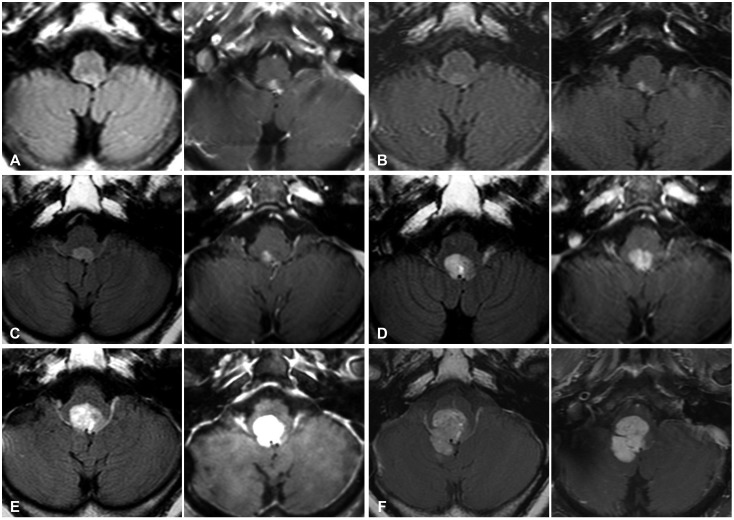
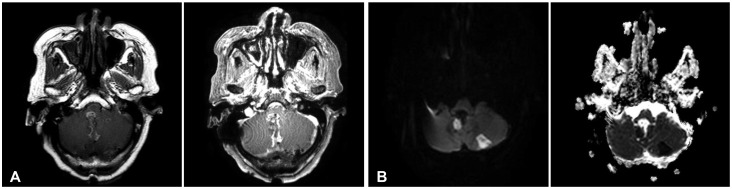
The preoperative T2-weighted MRI showed a 9×5 mm sized, well delineated extra-axial ventricle mass on the 4th ventricle floor, which was found retrospectively on the outside MRI in 2006 as 4 mm sized, 4th ventricle mass (Fig. 1A, B). It appeared isointense on T1-weighted imaging showed fuzzy enhancement after gadolinium enhancement (Fig. 1C, D). As the mass was asymptomatic, the patient refused to receive exploratory operation and have taken regular follow-up MRI and clinical check-up once a year, instead. The size of the tumor had increased each follow-up, but she had remained asymptomatic up to 6th year (Fig. 2). In 6th year follow-up, we recommended surgical excisional biopsy in 2017 for the possibility of malignant brain tumor, as the maximum diameter of the tumor increasing from 9 mm to 30 mm relatively rapidly, and MR spectroscopy with perfusion image showed relatively elevated choline peak to N-acetylaspartate (NAA) peak, which was compatible with low to intermediate degree of malignancy. But her and her family refused to receive surgery.
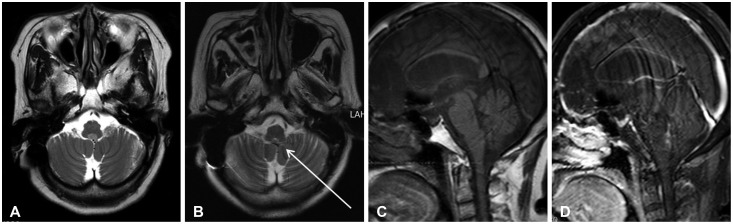 | Fig. 1Initial MRI at the time of diagnosis and retrospectively traced mass at 6 years ago MRI. A: Brain MRI revealed slightly high signal on T2-axial well-delinated ovoid mass in the 4th ventricle floor. B: The mass (arrow) was retrospectively found on MRI taken after aneurysmal clipping and ventriculo-peritoneal shunt 6 years ago. C: T1-sagittal MRI revealed, iso-signal intensity, and D: fuzzy enhancing mass after gadolinium enhancement.
|
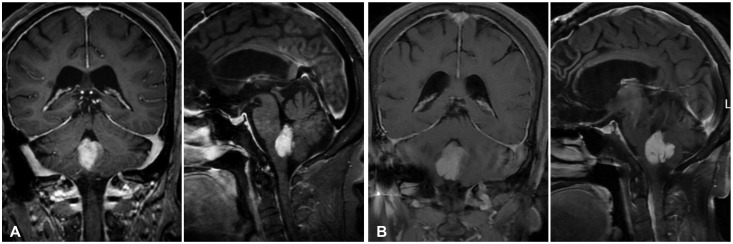
One year later, she vomited every day after meal and lost 5% of her weight. MRI follow-up showed the mass was extending through Foramen Magendie and compressing adjacent medulla and cerebellum (Fig. 3). The mass was enhanced with gadolinium and reached approximately 2.3×2.5×2.8 cm in diameter. The patient decided to receive operation to relief symptoms at 7th year follow-up of 74 years-old.
We performed surgery via midline suboccipital craniotomy with electromyogram-sensing endotracheal tube for monitoring of lower cranial nerve. The tumor was exposed between cerebellar tonsils. It was fragile and colored grey to purple. The tumor was easily dissected from the cerebellum and the roof of 4th ventricle but, sit was tightly attached to the lower lip of 4th ventricle floor. Thus, we leaved small seam of tumor adhered to dorsal lip of 4th ventricle, and near total resection of the tumor was achieved (Fig. 4).
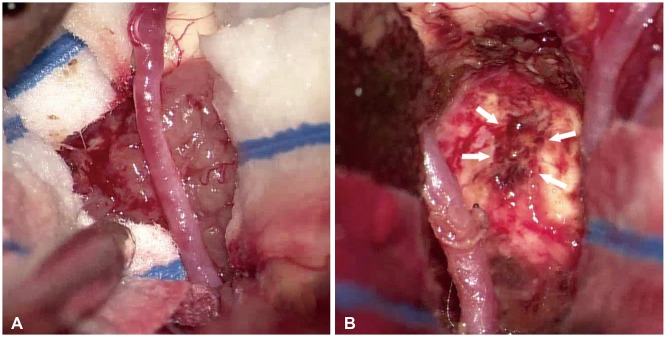 | Fig. 4Midline suboccipital craniotomy were used for resection of 4th ventricle tumor (A). The tumor was exposed between cerebellar tonsils. It was fragile and colored grey to purple (B). Using telovelar approach, we could easily dissect tumor from the cerebellum and the roof of 4th ventricle. We leaved small seam of tumor (arrows) adhered to dorsal lip of 4th ventricle, and near total resection of the tumor was achieved.
|
Histological examination showed relatively cellular tumor composed of small round cells arranged around blood vessels with intervening anucleate zones, forming perivascular pseudorosettes (Fig. 5A). In close up view, tumor cell processes converge on the blood vessels creating fibrillar zone of pseudo-rosettes (Fig. 5B). True ependymal rosettes having luminal spaces are also noted (Fig. 5C). On immunohistochemistry, dot-like perinuclear immunopositivity on epithelial membrane antigen stain was characteristic of ependymal cells (Fig. 5D). Ki-67 was positive for 3% of nuclei. The diagnosis was ependymoma (WHO grade II).
 | Fig. 5Pathologic feature of ependymoma. A: This celluilar tumor is composed of small round cells. The tumor cells are arranged around blood vessels with intervening anucleate zones, forming perivascular pseudorosettes.(H-E, ×100). B: In close up view, tumor cell processes converge on the blood vessels creating fibrillar zone of pseudorosettes (H-E, ×200). C: True ependymal rosettes having luminal spaces are also noted (H-E, ×100). D: Dot-like perinuclear immunopositivity on EMA stain is characteristic. It indicates intracellular lumen of ependymal tumor cells (EMA, ×100). H-E, hematoxylin and eosin; EMA, epithelial membrane antigen.
|
Postoperatively, she had hoarseness due to right vocal cord palsy, dysarthria, dysphagia, left side dysmetria, and aspiration tendency. So, she had to lean on Levin tube feeding, but rapidly recovered in 2 weeks and oral intake became possible with thickener. Postoperative MRI revealed total excision of enhancing mass with linear enhancement of surgical tract (Fig. 6). We examined spine MRI for the possibility of drop metastasis of spine, but spinal cord surface and leptomeninges were clear of tumor cells. The intra-operative CSF cytology also showed no involvement of tumor. She received intensive rehabilitation for ataxia and postural instability, and laryngoplasty for hoarseness. She was transferred to rehabilitation facility at postoperative 3 weeks. At 3 months follow-up, she walked independently and ate normal diet.
Go to :
DISCUSSION
Ependymal tumors are varied by histopathological grade, location, and genomics. The anatomical location is divided in the three part of the CNS system: spine, posterior fossa, and supratentorial and there is a tendency of different location depending on age. In children, two-thirds of ependymoma occurs in posterior fossa. On the contrary, it usually occurs on supratentorium in adults [1]. WHO grades tends to have different ratio depending of the location. In infratentorial ependymomas, WHO grade II account for 83% of patients and especially 89.2% in patients older than 55 years [3]. But patients with age over 55 just account for 34.9% of infratentorial ependymoma. In this patient, the tumor occurred at infratentorium and WHO grade II despite being age of 68 years. Among infratentorial ependymal tumor found at 55 years-old or more, about 28% of cases were WHO grade II. From the literature, Hayashi et al. [5] found 9 cases of ependymoma diagnosed older than 60 years including 4 cases of 4th ventricle ependymoma (Table 1) [5]. Present case is the 5th case of 4th ventricle ependymoma diagnosed at age of 60 years and older, and only case that was found asymptomatic at first presentation. Among those 5 cases, 4 cases were revealed to be WHO grade II.
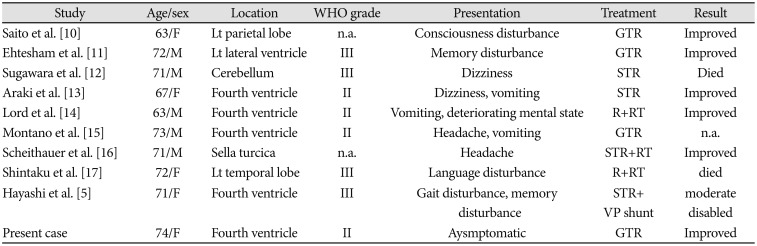
Table 1
Cases of ependymoma in the elderly patients (≥60 years old) from the literature
Adapted from Hayashi et al. Neurol Med Chir (Tokyo) 2012;52:611–6 [5]. GTR, gross total resection; Lt, left; n.a., not available; R, resection (detail was not described); RT, radiotherapy; STR, subtotal resection; WHO, World Health Organization; VP, ventriculo-peritoneal
![]()
Due to adjacent critical structures, posterior fossa, especially fourth ventricle, ependymoma is closely associated with neurological sequelae: gait and motor deficits, speech/swallowing deficits, and cranial nerve deficit. The present case was suffered from vocal cord palsy, dysphagia, aspiration tendency, tongue deviation, and truncal ataxia. Ferguson et al. [6] reported that gait and motor deficit was the most common postoperative complication of fourth ventricle tumor. It affected 56% of patient and lateral extension of tumor is associated with increased incidence of postoperative gait disturbance. In their series, 38% of patients had postoperative speech/swallowing deficits. Anterior extension of tumor significantly associated with this deficit, abutting or invading the brainstem In this context, we suggest that the sooner patients get surgical management before tumor extension, the better with least postoperative complication.
Considering prognostic factor of disease is most important things to know. Age, sex, preoperative Karnofsky Performance Scale (KPS) score, tumor location, extent of surgery, WHO grade, Ki-67 index, adjuvant rt had great impact on the prognosis of infratentorial ependymoma. In this case, female, KPS=80, WHO grade II, Ki-67 index <10% (3%), GTR are good prognostic factor. But 68 year old, lateral and floor extension, no adjuvant RT has bad effect on the prognosis [3].
Also, it is important to consider genetic and molecular alteration like RELA, YAP-1, CIMP. But insurance is not covered these examination in Kore, thus we do not check molecular and genetic alteration. We did not consider adjuvant therapy like radiotherapy, because tumor was gross totally resected on postoperative MRI.
When we reviewed the benign brain tumors in the elderly, most of their treatment plans were wait-and-see. Because, patients diagnosed brain tumor at least 60 years of age presented four times the mortality risk of being between the ages of 18 and 59 [7] and generally elderly benign tumor grow slowly. Although WHO grade is different, meningioma and vestibular schwannoma had revealed the tumor growth rate on wait-and-see follow up period. The mean growth speed of meningioma was 4.94 cm3/year in volume and 0.37 cm/year in diameter. Doubling time of it was 8 years [8]. Similarly, vestibular schwannomas also grow slowly. Initial growth rate in extrameatal vestibular schwannomas was 4.90 mm/year at first year following mean annual growth rate 2.79, 1.15, and 0.75 mm/year [9]. But these studies did not specific the growth rate in elderly patients. Our case was found in old age (68 year-old) without any symptoms and we observed the growth of the tumor by annual MRI follow-up. The largest tumor diameter increased from 9 mm to 30 mm during six years and the apparent annual mean growth rate of diameter was 3.0 mm/year. Our case is a rare case of continuously growing 4th ventricle ependymoma in elderly. Considering this case, we suggest that the elderly who diagnosed with ‘supposed-to-be-benign’ brain tumor need close follow-up to determine the future surgical intervention and to minimize the postoperative complication.
Go to :
 XML Download
XML Download