

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer is major cause of cancer death. Non-small cell lung cancer (NSCLC) accounts for about 80% of all lung cancers [1]. Traditionally, surgical resection with or without adjuvant chemotherapy is major treatment choice for lung cancer. However, due to poor therapeutic response and high mortality rate, research has focused on understanding molecular mechanism of cancer [1]. Due to development of molecular biology, molecular targeted agent such as epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKI) is used significantly in the treatment of NSCLC. Some patients have shown dramatic response to TKI [23]. Patients with EGFR mutation have longer median progression free survival than those with wild-type EGFR disease (15.2 months versus 4.4 months, p<0.05) [4].
For patients with brain metastasis (BM), prognosis remains poor, with a median survival time of 4.5–6.0 months despite standard treatment of whole-brain radiation therapy (WBRT) [56789]. About 50% patients of NSCLC have BM. However, characteristics of BM are not well established yet [9].
In Korea society, EGFR mutation rate in NSCLC has been reported to be about 48.6% to 60% in BM [2]. Patients who receive an EGFR TKI therapy after diagnosis of BM are known to survive longer than those who do not [9], suggesting that TKI therapy might be also effective in metastatic brain lesion. However, TKI therapy in BM did not always reveal good treatment results. This might be due to different EGFR mutational status between BM and primary NSCLC. Thus, the objective of this study was to determine EGFR mutational status in BM and primary NSCLC and compare the discordance rate of paired EGFR mutation status. This is the first report to analyze the discordance rate between metastatic brain tumors and NSCLC in Korea society.
Go to : 
MATERIALS AND METHODS
Records of patients who underwent craniotomy for metastatic brain tumors arising from NSCLC at the Neuro-Oncology Clinic of the National Cancer Center of Korea between 2011 and 2016 were retrospectively reviewed. A total of 74 patients underwent surgical resection of a metastatic brain tumor from NSCLC. Among them, retrospective clinical review was performed for 46 patients who underwent EGFR sequencing analysis for primary NSCLC tissues or metastatic brain tissue. Status of EGFR mutations was determined by using peptide nucleic acid mediated real-time PCR clamping method. Pathologic data were collected from electronic medical records, including patient demographics, histological type, grade, tumor stage, and biomarker status.
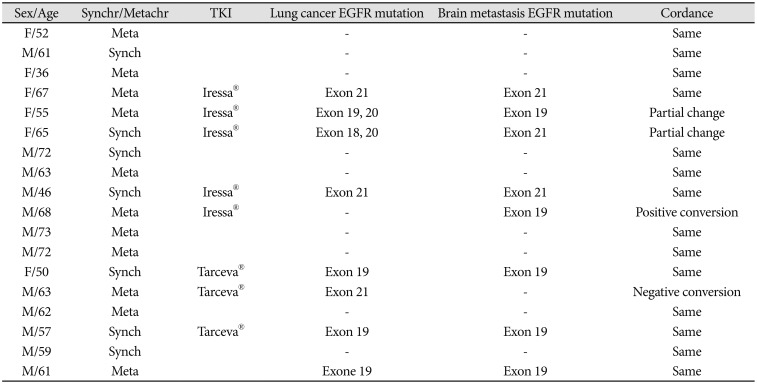
We compared the EGFR mutation frequencies in both primary lung cancer and metastatic brain lesion and analyzed the mutational change of metastatic brain tumor. Based on the mutational change, we classified change in preexisting mutation as partial change, newly developed mutation as positive conversion, absence of mutation as negative conversion, respectively.
Go to :
RESULTS
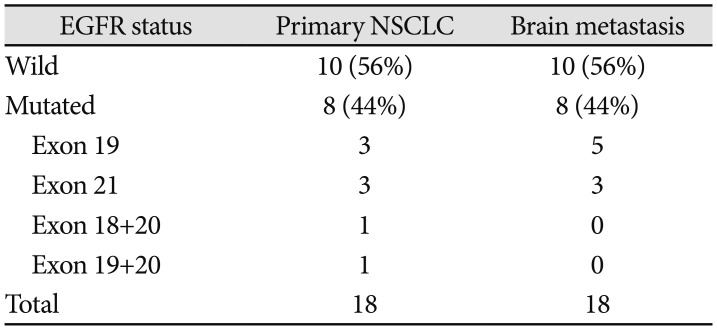
A total of 46 patients (28 males and 18 females) were included in this study. Their mean age was 62.2 (range, 36–83) years. Among these 46 cases, 18 (39.1%) cases showed EGFR mutation in primary lung cancer. Detected mutation sites were exon 19 (8 cases), exon 21 (6 cases), exon 18 (1 cases), and multiple mutations (3 cases) (Table 1). About 61.1% (11/18) of female patients and 25% (7/28) of male patients showed EGFR mutation. All female patients were never smokers. About 66.7% of male non-smokers showed EGFR mutation. In 18 cases of BM, EGFR mutation studies were done. Among them, 8 (25.6%) cases showed mutation on exon 19 (5 cases) or exon 21 (3 cases). To compare EGFR mutation status between primary lung cancer and BM, 18 paired tissues from both NSCLC and matched BM were collected (Table 2). Four (22.5%) patients were discordant for the status of EGFR between primary and metastatic sites. There were two partial changes, positive conversion and negative conversion were one case each (Table 3).
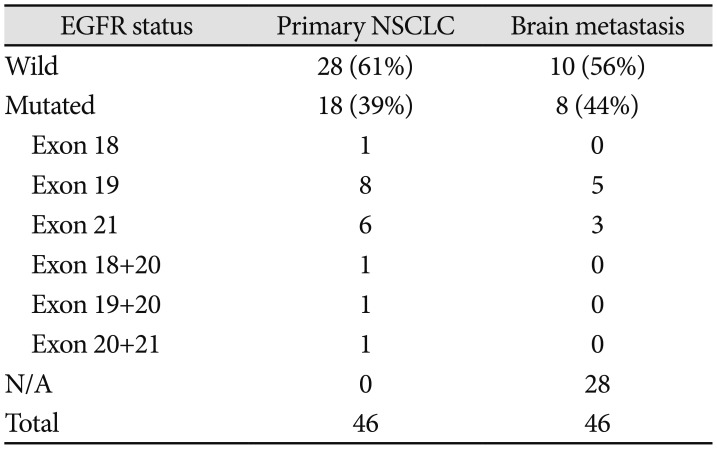
Table 1
Result of EGFR mutation analysis: comparison between 46 patients who underwent EGFR sequencing
![]()
Go to :
DISCUSSION
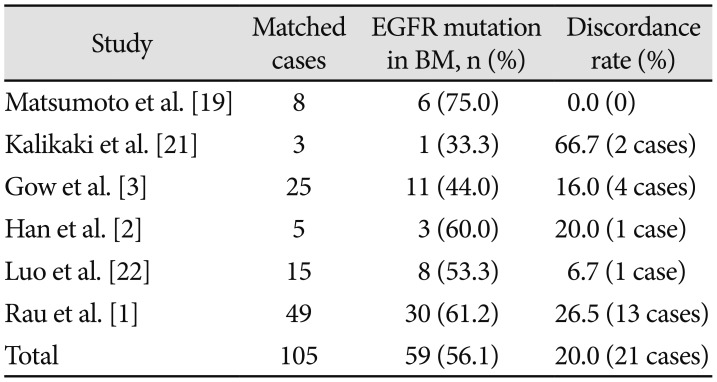
Molecular targeted agents are becoming important treatment choice for cancer because they can lead to good prognosis. Several studies have shown that patients with EGFR mutations have better response to EGFR TKI therapy than those without such mutations [1011]. In a prior study, Gow et al. [12] have retrospectively analyzed 63 NSCLC patients with BM who are treated with WBRT and found that 46 patients who have EGFR mutation have a median survival of 17.3 months while wild-type patients only have a median survival of 6.6 months [12]. A recent study has revealed that patients with EGFR-mutant metastatic lung adenocarcinoma have longer overall survival than wild type patients (30.9 months versus 12.1 months, p<0.05) [13]. Therefore, it is important to identify EGFR mutation status of metastatic lesion for anticipating prognosis. However, previous studies have shown that mutational status of metastatic lesion does not always coincide with primary site. Through the literature review, discordance rate between primary tumor and corresponding metastasis is about 16.2% or 30% by immunohistochemistry analysis [914]. Many studies have revealed heterogeneity of cancer cells and different metastasis site [15161718]. In many studies conducted in other countries, mean discordance rate of EGFR mutation status between primary NSCLC and BM is 20% (Table 4). Masumoto et al. [19] have analyzed 21 metastatic brain tumor tissues from 19 patients treated for lung cancers from 1986 to 2001. They found that all 6 cases with EGFR mutations in their metastatic brain tissues had the same mutational status in the corresponding primary lung cancers. In another study, Rau et al. [1] have analyzed 49 paired tissues with both primary adenocarcinoma of lung and metastatic brain lesion. Their results revealed a discordance rate of 26.5% between primary lung cancer and BM. In our case, in Korea, the discordant rate between primary NSCLC and metastatic brain lesion was 22.5%, similar to that in the previous study [1]. It is known that EGFR mutations in lung cancer occur more frequently in East Asian patients than in Caucasian patients [19]. Therefore, we anticipated that the discordance rate of EGFR mutations would be higher in Asian patients. However, our study revealed that the discordance rate was not higher in Asian patients.
In univariate analysis, EGFR mutation has been found more frequently in female and never smokers [20]. In our study, female accounted for 61.1%. All female patients were never smokers.
This study has some limitations. First, we used retrospective methods that might have selection bias. Biopsy and molecular analysis of primary site and metastatic lesion were not performed at the same time. Moreover, subjects of this study were patients who underwent craniotomy. Surgeons usually recommend this surgery only for patients with favorable prognostic factors. Second, the total number of patients was small. Although treatment choice for BM was WBRT, many lung cancer patients were unsuitable for surgery. Thus, interpretation of our results should be done with these considerations.
For effective systemic therapy, molecular diagnosis of metastatic lesion is recommended. However, biopsy of brain metastatic lesion is not always performed due to limited access to metastatic lesion. Our results suggest that discordant rate between primary NSCLC and metastatic brain lesion is significant. Therefore, if EGFR-mutant NSCLC patients show no response to optimal treatment, we strongly recommend biopsy of metastatic brain lesion.
To the best of our knowledge, this is the first report to analyze a considerable number of metastatic brain tumors of lung adenocarcinoma for EGFR mutations and compare the discordance rate in South Korea.
Go to :
 XML Download
XML Download