

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Sung Hoon Moon, M.D., Chul Gie Hong, M.D., Woon Sang Lee, M.D., Jin Woo Park, M.D.
Abstract
This case report describes the unusual occurrence of a flexor digitorum profundus avulsion secondary to an enchondroma of the distal phalanx of the middle finger. The enchondroma was treated by simple curettage with an autogenous bone graft harvested from the olecranon. The avulsed bone fragment was reattached to the distal phalanx using the pull-out suture technique. Bony union and full function of the digit were achieved.
Figures and Tables
Figure 1
Standard X-rays showing a bony fragment avulsed from an enchondroma at the base of the distal phalanx of the left middle finger. (A) Posteroanterior view. (B) Lateral view.
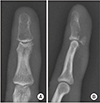
Figure 2
Post-contrast fat-suppressed T1-weighted magnetic resonance imagings show an expansile intramedullary lesion in the entire bone marrow of the distal phalanx with small dot-like enhancing foci. (A) Coronal view. (B) Sagittal view.

Figure 3
(A) Flexor digitorum profundus (FDP) tendon had been avulsed at its insertion. (B) After curettage and bone graft insertion, the FDP was reinserted on the grafted bone using the pull-out suture technique. (C) Immediate postoperative lateral X-ray shows the pull-out button on top of the nail plate.



References
1. Leddy JP, Packer JW. Avulsion of the profundus tendon insertion in athletes. J Hand Surg Am. 1977; 2:66–69.

2. Gaulke R. The distribution of solitary enchondromata at the hand. J Hand Surg Br. 2002; 27:444–445.
3. Lu H, Chen Q, Yang H, Shen H. Enchondroma in the distal phalanx of the finger: an observational study of 34 cases in a single institution. Medicine (Baltimore). 2016; 95:e4966.
4. Ogunro O. Avulsion of flexor profundus, secondary to enchondroma of the distal phalanx. J Hand Surg Am. 1983; 8:315–316.
5. Arthozoul M, Brun C, Laffosse JM, Martinel V, Grolleau JL, André A. Avulsion of flexor digitorum profundus secondary to enchondroma of the distal phalanx. Case report and literature review. Chir Main. 2015; 34:210–214.
6. Merchant J, Powell-Smith E. Enchondroma of the distal phalanx causing rupture of flexor digitorum profundus: successful fixation avoiding a pull-out suture. J Hand Surg Eur Vol. 2014; 39:1012–1013.
7. Hasselgren G, Forssblad P, Törnvall A. Bone grafting unnecessary in the treatment of enchondromas in the hand. J Hand Surg Am. 1991; 16:139–142.
8. Yamauchi T, Yoshii T, Sempuku T. Flexor digitorum profundus avulsion of the left little finger through enchondroma of the distal phalanx: pull-out wire technique treatment without bone graft. Hand Surg. 2008; 13:17–20.
9. Wong W, Cross K, Mahoney J. Avulsion of the flexor digitorum tendon secondary to enchondroma of the distal phalanx. Can J Plast Surg. 2004; 12:67–68.
10. Bruno RJ, Cohen MS, Berzins A, Sumner DR. Bone graft harvesting from the distal radius, olecranon, and iliac crest: a quantitative analysis. J Hand Surg Am. 2001; 26:135–141.
 XML Download
XML Download