

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Anterior uveitis (AU) is the most common extra-articular manifestation of ankylosing spondylitis (AS), with a pooled prevalence of 25.8%, according to a recent meta-analysis.1 It is one of the major causes of poor quality of life in patients with AS because of its relapsing disease course, frightening symptoms, and potential for vision impairment and ocular complications.2
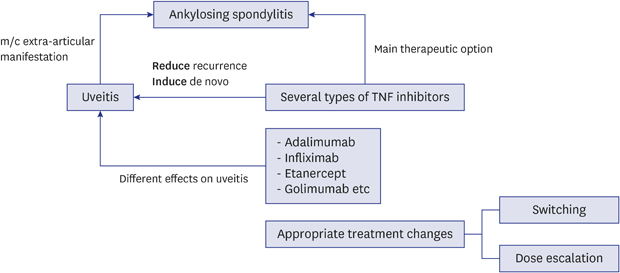
Currently, tumor necrosis factor-alpha (TNF-α) inhibitors (TNFis) are widely used to treat rheumatic diseases, including AS, and several studies have reported the efficacy of TNFis in reducing the incidence of AU in patients with AS.3456 However, some studies have suggested that TNFis may actually induce new-onset AU.789 Taken together these previous reports, TNFis may have a conflicting effect on the occurrence of uveitis.
Several types of TNFis are currently used for AS patients, including anti-TNF-α antibodies [adalimumab (ADA), infliximab (IFX), and golimumab (GOL)] and the soluble TNF receptor molecule (etanercept [ETN]).3 Although some previous studies have shown that anti-TNF-α antibodies and ETN similarly prevent AU,46 other studies have reported that TNF- α antibodies are better at preventing AU than ETN.10111213 Furthermore, the possibility of new-onset uveitis following TNFi therapy has been described mainly in patients treated with ETN.81415
Because AU is commonly caused by AS, TNFis are the main therapeutic agents for AS, and TNFis themselves may cause or exacerbate AU, the relationship between TNFis and AU in AS patients requires clarification. There are also several types of TNFis in use that may have different effects on AU, further complicating the relationship between TNF inhibition and AU development.
Accordingly, the aim of present study was to investigate the effect of TNFis on AU by analyzing the long-term clinical course of AU in AS patients treated with TNFi therapy at a single tertiary referral hospital in which there is strong collaboration between the departments of rheumatology and ophthalmology.
METHODS
The medical records of patients who were diagnosed with AS and treated with TNFis (ADA, IFX, ETN, or GOL) between January 2007 and July 2017 at the Department of Rheumatology of Asan Medical Center were retrospectively reviewed. Inclusion criteria were as follows 1) diagnosed with AS by rheumatologists; 2) treated with TNFis for more than 1 year; and 3) experienced at least one episode of AU during their disease course. The occurrence of AU was assessed on the basis of medical records. Only cases confirmed by an ophthalmologist were included. Patient with suspected infectious causes or prominent posterior involvement were excluded. Patients were also excluded from the study if the clinical features of uveitis in their medical records were incomplete.
The effect of TNFis on AU was investigated with respect to the following: the prevention of AU occurrence, the likelihood of new-onset AU after beginning TNFi therapy, the effects of drug switching, and the effects of dose escalation. To investigate the effect of each TNFi on the prevention of AU, the rates of uveitis flares before and after taking the drug in patients who developed AU before TNFi treatment initiation were calculated. The rate of uveitis flares before TNFi treatment was calculated as the number of AU attacks before TNFi treatment initiation divided by disease duration before TNFi treatment (rate/100 patient-years). The rate of uveitis flares during TNFi treatment was calculated as the number of AU attacks that occurred during TNFi treatment divided by the duration of TNFi treatment (rate/100 patient-years). Only cases where TNFi treatment was used first during the disease course were analysed. Cases in which TNFi was used as a second or third drug were excluded. The relapse-free survival rates among TNFi-treated patients were also measured to evaluate the effect of TNFi on the prevention of AU using Kaplan-Meier survival analysis. In cases of new-onset AU after TNFi therapy, the interval between TNFi treatment initiation and the onset of AU and underlying AS disease activity including the level of acute phase reactants and arthritic symptoms at the time of AU, were recorded to investigate the connection between TNFi therapy and AU development. The remission rate after a change in treatment (drug switching or dose escalation) in patients with prior uveitis flares during TNFi treatment was also evaluated. Remission was defined as the absence of AU recurrence for more than 1 year after the change in treatment.
Statistical analysis
Fisher's exact test was used to compare categorical variables, and Wilcoxon signed-rank test, Kruskal-Wallis test, or Mann-Whitney U test was used to compare continuous variables. Kaplan-Meier survival analysis was conducted to evaluate relapse rates after each TNFi treatment. The log-rank test was used to compare AU relapse free survival rates of patients treated with each TNFi. All statistical analyses were performed using SPSS 22.0 for Windows (SPSS, Inc., Chicago, IL, USA), and a P value of ≤ 0.05 was considered statistically significant.
RESULTS
In total, 619 consecutive patients with AS treated with at least one TNFi between January 2007 and July 2017 were screened. From these, 54 patients (42 men, 12 women) with at least one episode of uveitis flare were included in this study. The type and dose of TNFi each patient received was determined by a rheumatologist according to the patient’s clinical status. Generally, Adalimumab (40 mg) was administered subcutaneously every 2–6 weeks. Infliximab (3–5 mg/kg body weight) was administered intravenously during weeks 0, 2, 6, and 14 and at 6 to 12 week intervals thereafter. Etanercept was administered subcutaneously at 25 mg weekly, or from 50 mg once per week to 50 mg twice per weekly. All patients received topical steroid eye drops during the acute phase of uveitis flares; short-term, high-dose systemic steroids or periocular steroid injection was also used at the ophthalmologist's discretion in severe cases. The clinical characteristics of the patients are summarized in Table 1. The first uveitis flare was observed before TNFi treatment in 39 patients (72.2%) and during TNFi treatment in 15 patients (27.8%). During the disease course, 38 patients (70.3%) were treated with one type of TNFi, and 16 patients (29.6%) were treated with more than two types. Among patients treated with one TNFi, the majority received ADA.
Table 1
Demographic and clinical characteristics of patients
Data are presented as mean ± standard deviation (range or interval) or number (%).
TNFi = tumor necrosis factor alpha inhibitor, AU = anterior uveitis, ADA = adalimumab, IFX = infliximab, ETN = etanercept, GOL = golimumab.
![]()
The effect of TNFis on AU prevention
Among the 39 patients who experienced a uveitis flare before TNFi treatment, the type of TNFi first used was ADA in 25 patients, IFX in 7 patients, ETN in 6 patients, and GOL in 1 patient. Patients who received TNFis for less than 1 year (five patients on ADA, one patient on IFX, and two patients on ETN) were excluded from this analysis. In this group, the rates of uveitis flares (number of uveitis flares per 100 patient-years) before and after TNFi treatment were, respectively: for ADA, 59.78 ± 61.11 vs. 7.53 ± 14.63 (P = 0.001); for IFX, 39.78 ± 33.29 vs. 8.93 ± 14.44 (P = 0.046); and for ETN, 102.25 ± 92.21 vs. 71.95 ± 23.83 (P = 0.465) (Table 2). The rate of uveitis flares before treatment with TNFi did not differ among the three groups (P = 0.537), but the rate after treatment was significantly different (P = 0.001). Also, treatment with anti-TNF-α antibodies resulted in a significantly higher relapse-free survival rate than treatment with ETN (ADA vs. ETN, P < 0.001; IFX vs. ETN, P = 0.048) (Fig. 1). No difference was observed between ADA and IFX treatments (P = 0.506).
Table 2
The rates of uveitis flares before and after treatment with each type of TNFi

Data are presented as mean ± standard deviation.
TNFi = tumor necrosis factor alpha inhibitor, ADA = adalimumab, IFX = infliximab, ETN = etanercept, AU = anterior uveitis.
aKruskal-Wallis test; bWilcoxon signed-rank.
![]()
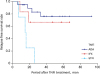 | Fig. 1Kaplan-Meier curve of time to AU relapse after TNFi treatment. There was significant difference in relapse free survival rate between anti-TNF-α antibodies and ETN but no difference between anti-TNF-α antibodies (ADA vs. ETN, P < 0.001; IFX vs. ETN, P = 0.048; ADA vs. IFX, P = 0.506).TNFi = tumor necrosis factor alpha inhibitor, ADA = adalimumab, IFX = infliximab, ETN = etanercept, AU = anterior uveitis.
|
The effect of TNFis on AU induction
Among the 15 patients who first developed AU after TNFi use, 5 were under treatment with soluble TNF receptor and 10 were under treatment with anti-TNF-α antibodies (ADA, 3 patients; INF, 6 patients; GOL, 1 patient) (Table 3). The onset of AU occurred within 1 year after the initiation of TNFi treatment in 4 of 5 patients (80%) treated with soluble TNF receptor and 2 of 10 patients (20%) treated with anti-TNF-α antibodies (P = 0.089). Patients treated with soluble TNF receptor tended to have lower AS disease activity (lower erythrocyte sedimentation rate [ESR]) and more controlled arthritic symptoms) at the time of uveitis flares than patients treated with anti-TNF-α antibodies, although this difference was not statistically significant (P = 0.358, P = 0.152).
Table 3
Comparison of clinical parameters for assessment of the relationship between TNFi use and AU occurrence
TNFi = tumor necrosis factor alpha inhibitor, ESR = erythrocyte sedimentation rate, AU = anterior uveitis, IQR = interquartile range.
aFisher's exact test; bMann-Whitney U test.
![]()
The effect of drug switching on AU occurrence
There were 22 episodes of drug switching during the study period; 16 patients were switched to a second TNFi, 5 patients were switched to a third drug, and 1 patient was switched to a fourth drug (Table 4). Switching was due to inadequate efficacy in 16 episodes and adverse effects in 6 episodes. With regard to the 16 episodes of inadequate efficacy, persistent AU relapse occurred in 6 cases and uncontrolled arthritic symptoms occurred in 10 cases. Seven of the nine patients (77.8%) who had a uveitis flare before switching showed no recurrence of AU after switching, and two patients with persistent recurrence even after the first switch showed no recurrence of AU after the second switch. Notably, no recurrence was observed in five of six patients (83.3%) for whom the drug was switched because of frequent AU relapse.
Table 4
Clinical characteristics of patients who were treated by switching to ≥ 2 TNFis
TNFi = tumor necrosis factor alpha inhibitor, M = men, ADA = adalimumab, IFX = infliximab, IE-R = inadequate efficacy related to arthritic symptoms, GOL = golimumab, IE-U = inadequate efficacy related to uveitis relapse, W = women, AE = adverse effects, ETN = etanercept.
![]()
The effect of dose escalation on AU occurrence
Dose escalation was required for eight patients who experienced uveitis flares during TNFi treatment (Fig. 2). The treatment interval was shortened in four of these eight patients (three on ADA and one on IFX), and the dose at each administration was increased in the remaining four (one on IFX and three on ETN). A total of five patients (62.5%) showed no relapse after dose escalation, which was achieved by shortening the interval between doses in three patients (two on ADA and one on IFX) and increasing the dose in two patients (one on IFX and one on ETN).

DISCUSSION
This retrospective study was intended to show the relationship between TNFi treatment and AU in patients with AS. First, with respect to the prevention of AU recurrence, the results of this study are consistent with previous studies reporting that the rate of uveitis flares in patients with AS was significantly decreased by treatment with anti-TNF-α antibodies, but not ETN.10111213 Although this study could not evaluate the effects of GOL specifically because of the small number of patients who received the drug, a recent multicenter prospective study reported that GOL also considerably reduced the risk of AU.16 Anti-TNF-α antibodies and soluble TNF receptor treatments also showed differences in efficacy when used to treat inflammatory bowel disease, another extra-articular manifestation of AS. The ability of IFX to induce more apoptosis of activated T cells than ETN is suggested to be one of the reasons for the differences in the efficacies of these agents for the treatment of Crohn's disease.17 This explanation might also explain the difference in efficacy between these two drugs for the prevention of AU, although the exact mechanism remains unknown.
In addition to the lower prevention of AU by ETN than by anti-TNF-α antibodies, several studies have reported that ETN may actually cause new onset AU.81415 In the present study, several patients experienced the first uveitis flare during TNFi treatment. Adverse drug reaction probability scales such as the Naranjo scale, which are used to assess the causality of adverse drug reactions, take into consideration the temporal relationship, the response to dechallenge or stopping, the response to rechallenge or re-exposure, and alternative explanations for the adverse event.18 In our study, AU first developed at less than 1 year after the initiation of TNFi therapy in 4 of 5 patients (80%) receiving ETN and 2 of 10 (20%) patients receiving anti-TNF-α antibodies. Although these results are not statistically significant due to the small number of cases, it appears that the number of patients in which AU occurred soon after the initiation of TNFi therapy was higher in patients receiving ETN than in those receiving anti-TNF-α antibodies. In addition, patients treated with soluble TNF receptor tended to have a lower ESR and more controlled arthritic symptoms at the time of uveitis flares, suggesting that AU in these patients could not be explained by exacerbation of the underlying rheumatologic disease. These findings suggest that drug-induced AU may not be associated with exacerbation of systemic inflammation. If so, the extent of systemic inflammation could be used to differentiate between AU caused by a lack of response to TNFi treatment and AU caused by TNFi treatment. Therefore, for patients with AS who experience AU attacks during TNFi treatment, clinicians should discern whether AU occurred because of uncontrolled systemic inflammation (i.e., inadequate efficacy of TNFi therapy) or the TNFi itself. In such cases, the type of TNFi used; the history of AU before TNFi therapy; systemic disease activity, including the serum levels of acute phase reactants; and the temporal relationship between the initiation of TNFi therapy and the onset of AU may be important factors for clinical decision-making.
Each TNFi differs in its mechanism of action and microstructure, which results in different responses and adverse effects in clinical practice.3 Therefore, unsuccessful treatment with one TNFi because of inadequate efficacy or adverse effects should not preclude the use of another, which may result in a response. The efficacy of switching among TNFis in various autoimmune diseases, including AS and refractory AU, has been reported in previous studies.192021 As shown in the present study, switching TNFis minimized the occurrence of AU in a substantial proportion of patients and was beneficial in patients who failed to respond to even second-line TNFi therapy. Various patterns of drug switching were effective at preventing AU flares, including switching from ETN to a monoclonal TNF-α antibody and switching between monoclonal TNF-α antibodies. The mechanisms involved in secondary failure to ADA or ETN in inflammatory arthropathies are different; failure to ETN is thought to be due to a primary mechanism and failure to ADA is thought to be due to a secondary mechanism associated with immunogenicity.22 Switching from ETN to monoclonal TNF-α antibody treatment is reasonable because these two drugs have different mechanisms of action and because ETN has a lower effects than monoclonal TNF-α antibody when used to prevent AU. Switching between monoclonal TNF-α antibodies might also be beneficial because the microstructures of monoclonal TNF-α antibody preparations are different. Primary and secondary failure of ADA has reported to result from the formation of antibodies against ADA in patients with various immune-mediated diseases.2324 In addition, Cordero-Coma et al.25 reported that the development of permanent antibodies against ADA was associated with undetectable trough ADA levels and worse AU outcomes. In these cases where weakly effective TNFi therapy was attributed to anti-drug antibody formation, administration of another drug with a different microstructure might be effective.
TNFis are administered by subcutaneous or intravenous injection at a certain interval; the dose can be controlled by adjusting the frequency of administration or the dose per injection. Dose escalation was reported to be an effective strategy to optimize efficacy and achieve clinical responses in patients with other immune-mediated diseases who showed secondary loss of response to TNFis.2627 In the present study, 62.5% of patients with uveitis flares during TNFi treatment did not recur after dose escalation. Furthermore, shortening of the interval of ADA administration from 3 to 2 weeks prevented AU recurrence, suggesting that there may be a certain threshold dose according to individual disease activity. However, in cases where drug augmentation is being considered, the possibility that AU was induced by the TNFi should be excluded.
This study has some limitations. The retrospective design and the small number of cases limited the statistical strength of the analysis. Also, because only cases of AU confirmed by an ophthalmologist were included in the study, this study may underestimate the number of AU cases in AS patients receiving TNFis. Because of the episodic nature of AU, the efficacy of TNFi for the prevention of AU can only be assessed through long-term observation. Thus, in this study, we only included cases in which the drug had been used for at least 1 year. However, even a period of 1 year might be insufficient. Patient heterogeneity and differences in treatment methods at the time of treatment changes should be analysed individually and compared with those at the time of no treatment changes. In this study, because of the small number of cases, all the cases were grouped together as if the agents and patients were similar. Thus, the failure to take into consideration patient heterogeneity and differences in treatment methods is a limitation of this study. Future studies with larger numbers of cases will be required to measure the effects of clinical parameters at the time of treatment changes. Also, to observe differences in the induction of de novo AU by TNFis, it will be important to compare the exact incidence rate of new onset AU among all patients prescribed each drug. However, this study could not analyse the incidence rate of de novo AU because it included only patients who experienced AU. Nevertheless, our findings provide meaningful information on the effects of TNFis in actual clinical practice, where dose escalation and drug switching among TNFis are frequently implemented.
In summary, our results suggest that the potential of TNFi treatment to prevent or exacerbate AU in patients with AS should be considered. First, the use of TNFis should be considered in patients with AS and frequent AU relapse, because it can significantly reduce the occurrence of uveitis flares. Second, for patients who experience new-onset uveitis flares or AU exacerbation after TNFi use, clinicians should consider whether the AU indicates a lack of response to the TNFi or was caused by the TNFi itself. In the case of the former, switching to another TNFi could be an effective therapeutic option. If switching to another TNFi is difficult because of the potential adverse effects or previous treatment failure of another TNFi, dose escalation could be considered carefully. On the other hand, if the cause of AU is suspected to be the TNFi, switching to another TNFi, particularly anti-TNF-α antibody, is recommended. Clinicians should consider these various aspects of the relationship between TNFis and the disease course of AU in patients with AS.
 XML Download
XML Download