

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Advances in neonatal and pediatric intensive care have reduced child mortality. Especially in children with chronic respiratory failure, the use of mechanically-assisted ventilators reduced mortality and prolonged life span.1 However, children who would have passed away with poor treatment in the past or those who survive with substantial disabilities have formed a unique group of technology-dependent children. Due to the increase in the cost of medical care and the risk of hospital acquired infection, caregivers have shown interest in family-centered benefits of home care, and this has encouraged early discharges from long-term hospitalization. All this with improving rehabilitation technology has made home mechanical ventilation (HMV) a safe option for children and an expected service nowadays.23
Since its invention in 1977, there have been a number of regional and national surveys reporting on the status and trend of pediatric HMV from many centers around the world, including centers in USA and Europe.4567891011 The HMV population has not only grown worldwide but also has included various diagnosis and complex medical conditions. In addition, growth in this population showed different characteristics across countries and ventilator subgroups. Eurovent surveys,2 a wide cross sectional survey including both adults and children, report how important information collection is for national planning of HMV use. However, there are limited studies on pediatric HMV and only one recent nationwide report in Korea.121314
Since the Korean national health insurance started to cover HMV in 2016, the cost of HMV has reduced and population based nationwide data has been available, which might have resulted in an upsurge of HMV use. It is crucial to understand this population through analyzing the present situation. To that end, we have done descriptive analyses on children using HMV from the National Health Insurance Service (NHIS) database for a nationwide scale study, and from a tertiary children's hospital for more detail to show the present situation of Korea. We also investigated unmet needs and compared it to the evolution of home care programs and the use of resources in other countries.
METHODS
Study population
This study utilized data from NHIS, which provides mandatory health insurance in Korea. The percentage of the population affiliated is 99.01% which covers all forms of medical service, including medical visits, admissions, ICU care, emergency care, and pharmaceutical services. Medical institutions submit health care utilization information in electronic form for reimbursement purposes, and this information is integrated to the NHIS database. From this, HMV prescriptions for children under the age of 19 were retrieved using payment code 3150 for prescriptions in 2016. Patients who have returned their prescribed HMV within 3 months have been excluded from analysis.
In a single tertiary center, retrospective chart review was conducted on children under the age of 18, who received prescriptions for HMV for at least 3 months in Severance Children's Hospital between January 1, 2016 and December 31, 2018.
Characteristics of children using HMV
From the NHIS database, basic demographic data, cases of tracheostomy, adjunctive therapies (oxygen, gastrostomy), and home nursing care were collected. Cases of tracheostomy were retrieved using medical charge codes O1300 (invasive tracheostomy), O1301 (percutaneous dilatational tracheostomy), O1305 (mediastinal tracheostomy). Patients who had a tracheostomy record at least once between 2002 and the prescription of HMV in 2016 were considered as having tracheostomy. Gastrostomy cases were collected using codes Q2614 (permanent invasive gastrostomy), Q2613 (transient invasive gastrostomy), Q2612 and M6730 (percutaneous gastrostomy). Instances of oxygen therapy was gathered based on prescription code M0040 (oxygen inhalation per day). Home nursing care was under the codes AN200, AN300, AN400, or AN500, depending on the type of hospital the prescription was made from. This study was conducted assuming that all patients with HMV prescriptions use HMV as prescribed. Patients with a tracheostomy or gastrostomy prescription code were considered performed. From all children with prescribed HMV in 2016, cause of death was analyzed for all deceased cases in 2016 using the Statistics Korea database. This database is based on death certificate forms filled out at death by physicians, which specifies the primary cause of death using International Classification of Disease 10th revision (ICD-10) codes. We have classified cause of death into 5 categories; underlying disease, respiratory failure, infection, cardiac, and unclassified. Causes of respiratory failure were estimated using the principal diagnosis in insurance claim records up to 2 years before the prescription of HMV. Due to the nature of the data, only year-end age was available for analysis, and this was used to compute median age and quartile ranges.
From a tertiary center, Severance Children's Hospital data, basic demographic data (sex, age, age at initiation), type of HMV (non-invasive ventilation or invasive ventilation via tracheostomy), causes of respiratory failure, adjunctive therapies (oxygen, gastrostomy), patient outcome from current medical status (current followed, improved, lost to follow-up, transferred to local center, mortality), and home nursing care were reviewed.
Statistical analysis
All data acquired from NHIS was analyzed using R version 3.4.4 (R Foundation, Vienna, Austria), and tertiary center data was evaluated using SPSS 23.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the entire study population. Results are presented as frequencies, or median and interquartile, as appropriate.
Ethic statement
The present study protocol was reviewed and approved by the Institutional Review Board of Yonsei University College of Medicine (approval No. 4-2018-0333). Because this was an observational study without intervention and without the presentation of any identifying data, the committee ruled that informed consent was unnecessary.
RESULTS
National prevalence of children using home mechanical ventilation
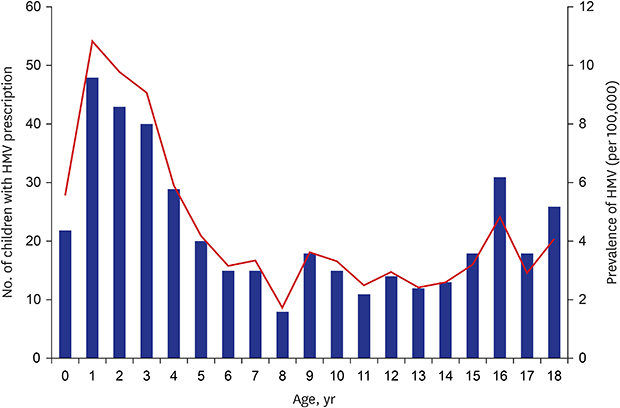
From the NHIS dataset, a total of 416 patients were prescribed with HMV in 2016, with an estimated prevalence of 4.4 per 100,000 in children younger than 19. The number of patients using HMV was the highest at age 1 with 48 cases, followed by an overall decrease, and showed a second peak at age 16. The estimated prevalence also peaked at 10.9 per 100,000 in 1-year-old patients and bottomed out at 1.7 in 8-year-old patients (Fig. 1).
 | Fig. 1The number of children by age at prescription of HMV, retrieved from National Health Insurance Service data. The number of patients using HMV at 1-year-old was the highest, followed by an overall decrease, and showed a second peak at 16-year-old. The black bars indicate the number of children who were prescribed with HMV at each age. The red line shows the prevalence of each age group.HMV = home mechanical ventilation.
|
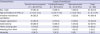
Of the patients, 267 (64%) were male, and median age at HMV prescription was 6-year-old. 202 (49%) had tracheostomy, suggesting that almost half of the patients used invasive mechanical ventilation. 60% of the patients were prescribed with oxygen. A quarter of the patients had gastronomy, and less than a quarter of the patients received home nursing care (Table 1).
Table 1
Characteristics of children using HMV, according to the estimated etiology for the need of ventilator support, retrieved from National Health Insurance Service data
![]()
The estimated causes of HMV use and patient characteristics are shown in Table 1. The most frequent cause was neuromuscular diseases (52%), followed by central nervous system (CNS) diseases (34%), and cardiopulmonary diseases (14%). The median age at which HMV was prescribed was the highest in neuromuscular diseases (10-year-old) compared to other causes. Patients with tracheostomy accounted for more than half in patients with CNS diseases and with cardiopulmonary diseases. Age at receiving tracheostomy was youngest (1-year-old) in patients with cardiopulmonary diseases. The majority of patients with CNS diseases and cardiopulmonary diseases received oxygen prescription. One third of the patients with CNS diseases had gastrostomy, which was most common compared to other causes. According to data from the National Statistical Office, of the patients prescribed with HMV, 51 patients died in 2016 and had a mortality rate of 12.3%. Patients with CNS diseases died the most, followed by neuromuscular diseases and cardiopulmonary diseases. The most common estimated cause of death was the aggravation of underlying diseases. Unclassified causes consisted of one hepatic failure and one burn in patients with CNS diseases and all others were unknown (Table 2).
Table 2
Cause of the death of patients prescribed with home mechanical ventilation, retrieved by the National Statistical Office
![]()
Clinical characteristics of children using home mechanical ventilation
Fig. 2 shows the increasing number of patients using HMV in Severance Children's Hospital from 2016 to 2018, including both invasive and non-invasive mechanical ventilation. A total of 62 patients received HMV between January 2016 and December 2018. 64.5% were male, and the majority of patients (70%) received invasive mechanical ventilation via tracheostomy. The number of patients using HMV showed an increase over the years, especially in non-invasive mechanical ventilation (Fig. 2A). The median age at start of HMV was 3.1-year-old. Patients under 1 year of age accounted for 40%, and the number of patients prescribed with HMV gradually decreased with age. The majority of patients used supplemental oxygen (84%) and had gastrostomy (68%). Less than 20% of patients received home nursing care. While five patients weaned off HMV, five patients passed away within the study period (Table 3). Three patients died of pneumonia, one died of hypoxia due to tracheostomy tube removal and one died of unclassified respiratory failure.
 | Fig. 2The number of children using HMV per year in a tertiary center. (A) The number of patients using HMV doubled from 12 in 2016 to 29 in 2018. Similar trends are shown in both invasive and non-invasive mechanical ventilation. (B) The number of the children using HMV was the highest at age 0 and generally decreased with age.IMV = invasive mechanical ventilation, NIV = non-invasive mechanical ventilation, HMV = home mechanical ventilation.
|
Table 3
Characteristics of children using HMV according to the etiology for the need of ventilator support, retrieved from a tertiary center
![]()
Cause of HMV use and patients' clinical characteristics are shown in Table 3. CNS diseases were the most frequent cause (68%), followed by cardiopulmonary diseases and neuromuscular diseases, which differed from the etiology retrieved from NHIS. The most represented CNS diseases were hypoxic ischemic encephalopathy (14 cases), epilepsy (11 cases), and encephalitis (7 cases). Non-invasive mechanical ventilation accounted for the largest fraction in neuromuscular diseases (75%), while invasive mechanical ventilation was the largest in CNS diseases (86%).
DISCUSSION
In 2016, a total of 416 patients were prescribed with HMV in Korea, with an estimated prevalence of 4.4 per 100,000 for children under 19, which is comparable to other countries.51516 Median age was 6 and the most frequent cause of HMV use was neuromuscular diseases. The type of ventilation in about half of the patients were estimated as invasive mechanical ventilation. Data from Severance Children's Hospital has suggested that the number of patients using HMV, especially non-invasive mechanical ventilation, has increased by about three-fold from 2016 to 2018. The increasing trend coincides with the worldwide trend of home-ventilator use for children, which has been on the rise for as much as 3–4 folds over the last decade.1718 The median age at start of HMV was 3.1 and the main cause was CNS diseases, which was notably different from the NHIS data.
Although the NHIS data showed the estimated prevalence of HMV use in Korean children, it lacked the exact duration of HMV use including the age at start, the type of HMV (invasive or non-invasive), and the duration of use per day (all day long, intermittently, as needed base or no use). Hence, the prescription of HMV, oxygen use, tracheostomy, and gastrostomy only gives collateral information, suggesting that it cannot represent the exact situation. Nonetheless, our data could reflect the current situation of HMV, because HMV is used for chronically ill patients, not acutely ill patients. To complement these limitations, we have also shown data from a tertiary center to bridge the gaps.
The estimated number of patients using invasive ventilation via tracheostomy from NHIS was 202 cases (49%), while the ratio in the hospital was 69%, which is higher than the use in other countries (from 23% to 49%).410 These differences likely reflect differing years of study and study designs, as well as discrepancies in clinical management and cultural differences.4101617192021 Of note, hospital data showed an increase in use of non-invasive mechanical ventilation at the starting year of insurance coverage, suggesting that physicians might have perceived it as more affordable for patients. According to the estimated causes of HMV from NHIS, the number of patients with neuromuscular diseases who underwent tracheostomy was only 34%. This is consistent with other studies,41022 reporting a significant increase in NIV for neuromuscular diseases in the past 20 years.18 In contrary, another study on neuromuscular disease patients using HMV in Korea showed that most patients (84%) used invasive ventilation via tracheostomy.13 Because this research was done in a single hospital, the nature of the disease group, especially SMA type 1, might have created a bias in the result. Invasive ventilation via tracheostomy were most frequent with 67% in CNS diseases within the study. Many children with CNS involvement have problems with cooperation, clearing airway and swallowing as well as a decrease in respiratory drive, which is known as a contraindication to NIV.323 Similar results were obtained in the hospital data, consistent with the Eurovent survey.2 These results show that HMV type may differ depending on the disease group.
According to the estimated causes of HMV from NHIS data, neuromuscular diseases occupied the largest proportion (52%), followed by CNS (34%) and cardiopulmonary diseases (14%), which was similar to the results in studies from other countries. Age of patients with neuromuscular disease was the oldest (10-year-old) and cardiopulmonary disease (2-year-old) was the youngest, probably due to the general characteristics of each disease group. Also, the CNS disease group had the most adjunctive therapies, such as gastrostomy (35%). This might be due to overall dysfunction from central originated problems. On the other hand, the most common cause of HMV use in the tertiary center was CNS involvement (68%), followed by cardiopulmonary (19%) and neuromuscular diseases (13%). Despite the difference in order, each group showed similar characteristics with the NHIS data. As a result, this shows that there may be differences in disease groups at each center, and the characteristics of patients may differ depending on the disease group.
Previous studies on HMV use by children are summarized in Table 4.45671012151617182021222425 Physicians in North America, Europe, and Japan have begun to recognize the importance of HMVs and analyzed their status starting from the 1990s. In the 2000s, relatively small-scale analysis of the status of home ventilation usage (n = 30–200) from single centers of hospitals or distinct regions of a country have been reported, emphasizing the need for a national wide HMV program. In the 2010s, large-scale analysis, either multicentered or nationwide (n = 300–900) was done to improve care for home ventilated children. On the other hand, there have been no systematic HMV study in Korea after one in 2005 consisting of 21 children in a tertiary hospital.13
Table 4
Previous studies on home mechanical ventilation for children

| Years | Author (Ref) | Country | Resources | Study period, yr | Sample size, No. | Method | Patient |
|---|---|---|---|---|---|---|---|
| 1995 | Fauroux et al.6 | France | ANTADIR networka | 1992–1993 | 287 | National wide | 158 cases of MV |
| Prospective | IMV 10% | ||||||
| NIV 90% | |||||||
| 1996 | Sakakihara et al.15 | Japan | Not mentioned | 1993 | 434 | National wide | Long term ventilated children |
| Cross-sectional | |||||||
| 2001 | Kamma et al.16 | Switzerland | Not mentioned | 2000 | 32 | National wide | Long term ventilated children |
| Cross-sectional | |||||||
| 2003 | Fauroux et al.7 | France | Not mentioned | 2000 | 102 | National wide | NIV |
| Cross-sectional | |||||||
| 2005 | Edwards et al.20 | New Zealand (Auckland) | Not mentioned | 1991–2004 | 160 | Regional | IMV 3% |
| Single center | NIV 68% | ||||||
| Retrospective | CPAP 29% | ||||||
| 2005 | Ahn et al.12 | Korea | Not mentioned | 1997–2003 | 21 | Regional | IMV 100% |
| Single center | NIV 0% | ||||||
| Retrospective | |||||||
| 2006 | Bertrand et al.24 | Chile | Home ventilatory assistance programb | 1993–2004 | 35 | Regional | IMV 23% |
| Single center | NIV 23% | ||||||
| Retrospective | CPAP 49% | ||||||
| 2007 | Gowans et al.5 | US (Utha) | Home respiratory services | 1994–2004 | 77 | Regional | IMV |
| Multi center | |||||||
| Retrospective | |||||||
| 2007 | Graham et al.4 | US (Massachusetts) | Pediatric home ventilator clinics | 2005 | 195 | Regional | IMV 49% |
| Pediatric pulmonary services | Multi center | NIV 49% | |||||
| Cross-sectional | |||||||
| 2008 | Oktem et al.21 | Turkey | Not mentioned | 2001–2006 | 34 | Regional | IMV 32% |
| Single center | NIV 68% | ||||||
| Retrospective | |||||||
| 2010 | Tibballs et al.25 | Australia | Pediatric home ventilator programc | 1979–2008 | 168 | Regional | IMV 28% |
| Single center | NIV 30% | ||||||
| Retrospective | CPAP 37% | ||||||
| 2011 | Wallis et al.10 | UK | Local community respiratory services | 2008 | 933 | National wide | NIV 22% |
| Cross-sectional | IMV 43% | ||||||
| 2011 | Racca et al.22 | Italy | Not mentioned | 2007 | 362 | National wide | IMV 41% |
| Cross sectional | NIV 59% | ||||||
| 2012 | Paulides et al.17 | Netherland | Home mechanical ventilation centerd | 1979–2009 | 197 | Regional | IMV 51% |
| Single center | NIV 49% | ||||||
| Retrospective | |||||||
| Observational | |||||||
| 2014 | Amin et al.18 | Canada | Pediatric home ventilation programe | 1991–2011 | 379 | Regional | IMV 17% |
| Multicenter | NIV 83% | ||||||
| Retrospective |
References are sorted by published year.
MV = mechanical ventilation, IMV = invasive mechanical ventilation, NIV = non-invasive ventilation, CPAP = continuous positive airway pressure.
aAssociation National Pour le Traitment a Domicile de l'Insuffisance Respiratoire chronique, national organization for home treatment of chronic respiratory failure which fedrate 33 regional associations distributed al over France; bProgram from the Pediatric Service of the Hospital Clinico de la Pontificia Universidad Catolica de Chile; cAd hoc program at the Royal Children's Hospital, Melbourne; dCenter for Home mechanical ventilation, Utrecht; eHome ventilation program at The Hospital for Sick Children, Toronto (Sick Kid).
![]()
A recent paper14 has reported on the prevalence and characteristics of HMV use in the whole population of Korea using data from NHIS, showing the current situation of HMV in Korea after insurance coverage started in 2016. They showed neuromuscular diseases as the most common primary diagnosis and less use of NIV in children younger than 18, which is consistent with our study. Our study focused on children using HMV because there are only a few nursing hospitals for children in Korea compared to adult nursing hospitals. Here, we showed characteristics by age including subdivision and distribution in children using HMV, specific clinical characteristics by disease groups, which might provide insights on family workload. There is a significant lack of resources including home nursing care compared to other countries, even though half of the patients need adjunctive therapies.
Heavy workload, loss of personal time, financial, and emotional resources are the main burden of care related to home ventilation. Moreover, more than half of the children with HMV also have tracheostomy or gastrostomy and need supplementary oxygen, which are additional overloads to caregivers. Most adult patients using HMV are treated in a nursing hospital, but almost all pediatric patient are taken care of at home. Therefore, children with chronic ventilation done at home need a coordinated multi-disciplinary approach based on interactions between different teams from the hospital, community, family, and caregivers.822 According to this study, only 23% of children with HMV have received home nursing care in Korea. This nursing care is not specific to the ventilator, but is merely care for general management. Therefore, even with lacking personal resources, it is necessary to implement HMV centers in each hospital and provide a national wide program for children with HMV to improve care. Further research should be done to better understand the needs of patients and their families.
This study has several limitations. We initially aimed to investigate the present situation of children using HMV in Korea, but NHIS data included only a year of prescription data, which limits our perspective on detailed clinical characteristics. To overcome this limitation, we attempted to complement the lack of detail using 3-year tertiary center's data. However, it is difficult to conclude that the detail characteristics of children using HMV from the tertiary center are identical across the nation, because the data from the single tertiary center cannot be replaced with the NHIS data. The main cause of death inferred based on death certificate data from the National Statistical Office was shown different from the hospital data. The most common cause of death from death certificate data was due to underlying diseases, but it is unclear whether this is the direct cause. Therefore, careful investigation is needed when interpreting the data.
In conclusion, this study provides insights on the present situation of HMV utilization in Korean children. Resources for children with HMV is necessary to better understand and provide better care for patients and their families.
 XML Download
XML Download