

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Hyun-Seok Chae , Bo-Seul Jeon, Jung-Jin Lee, Seung-Geun Ahn, Jae-Min Seo
, Bo-Seul Jeon, Jung-Jin Lee, Seung-Geun Ahn, Jae-Min Seo
, Bo-Seul Jeon, Jung-Jin Lee, Seung-Geun Ahn, Jae-Min Seo
Abstract
Excessive tooth wear can cause irreversible damage to the occlusal surface and can alter the anterior occlusal relationship by destroying the structure of the anterior teeth needed for esthetics and proper anterior guidance. The anterior deep bite is not a morbid occlusion by itself, but it may cause problems such as soft tissue trauma, opposing tooth eruption, tooth wear, and occlusal trauma if there are no stable occlusal contacts between the lower incisal edge against its upper lingual surface. The most important goal of treatment is to form stable occlusal contact in centric relation. In this case report, patients with decrease in vertical dimension and anterior deep bite due to maxillary posterior tooth loss and excessive tooth wear were treated full mouth rehabilitation with increased vertical dimension to regain the space for restoration and improve anterior occlusal relationship and esthetics. The functional and aesthetic problems of the patient could be solved by the equal intensity contact of all the teeth in centic relation (CR), anterior guidance in harmony with the functional movement, and restoration of the wear surface beyond the enamel range.
Figures and Tables
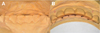
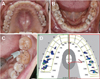
 | Fig. 1Pre-treatment state. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
|

 | Fig. 3Diagnostic cast. (A) Ligual view of mounted diagnostic cast, (B) There are no stable holding contacts on anterior teeth of the mounted diagnostic cast.
|

 | Fig. 5Recontouring of the anterior teeth. (A) Ligual view of diagnostic wax-up cast model, (B) On the diagnostic wax up, a definite holding stops can be provided for each lower incisal edge against its upper lingual surface.
|
 | Fig. 6Diagnostic wax-up model. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Lateral movement-right side, (F) Mandibular occlusal view, (G) Lateral movement-left side.
|
 | Fig. 7Provisional restorations. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Mandibular occlusal view.
|


 | Fig. 10Implant surgery on maxillary edentulous area. (A, B, C) #25, 26 implantation and guided bone regeneration, (D, E, F) #16, 17 implantation.
|
 | Fig. 11The equal intensity contacts of all the teeth in centric occlusion of provisional restoration. And incisal and canine guidance were achieved during each protrusive and lateral movement of mandible.
|
 | Fig. 12Master cast fabrication. (A) Tooth final preparation, (B) Final impression taking, (C) Working model for fixed prosthesis.
|
 | Fig. 13The shape of anterior teeth and the occlusal relationship of provisional restorations are reflected in the final restoration. (A) Customized anterior guide table, (B) Maxillary and mandibular models of provisional restoration mounted on articulator.
|
 | Fig. 14Aesthetic improvement according to occlusal vertical dimension elevation. (A) Facial photo before treatment, (B) Facial photo after provisional restoration.
|
 | Fig. 15Definitive prosthesis. (A) Maxillary occlusal view, (B) Right lateral view, (C) Frontal view, (D) Left lateral view, (E) Lateral movement-right side, (F) Mandibular occlusal view, (G) Lateral movement-left side.
|

References
1. Dawson PE. Functional Occlusion: from TMJ to smile design. St. Louis: Mosby Elsevier;2007. p. 430–466.
2. Akerly WB. Prosthodontic treatment of traumatic overlap of the anterior teeth. J Prosthet Dent. 1977; 38:26–34.

3. The council of professors of dental universities. Textbook of orthodontics. 3rd ed. Seoul: DaehanNarae Publishing;2006. p. 109p. 177–183.
4. The glossary of prosthodontic terms: Ninth edition. J Prosthet Dent. 2017; 117:e1–e105.
5. Okeson JP. Management of temporomandibular disorders and occlusion. 7th ed. St. Louis: Mosby Elsevier;2008. p. 56–61.
6. Beddis HP, Durey K, Alhilou A, Chan MF. The restorative management of the deep overbite. Br Dent J. 2014; 217:509–515.
7. Ramfjord SP, Ash MM Jr. Significance of occlusion in the etiology and treatment of early, moderate, and advanced periodontitis. J Periodontol. 1981; 52:511–517.
8. Gwon GR. The prosthetic approach for collapsed vertical dimension of occlusion. J Korea Acad Stomatognathic. 2004; 20:170–181.
9. Park JH, Jeong CM, Jeon YC, Lim JS. A study on the occlusal plane and the vertical dimension in Korean adults with natural dentition. J Korean Acad Prosthodont. 2005; 43:41–51.
10. Willis FM. Features of the face involved in full denture prosthesis. Dent Cosmos. 1935; 77:851–854.
11. Pleasure MA. Correct vertical dimension and freeway space. J Am Dent Assoc. 1951; 43:160–163.
12. Yang WS, Kim TW, Baek SH. Current orthodontic diagnosis. Seoul: DaehanNarae Publishing;2007. p. 447.
13. Rodriguez-Cardenas YA, Arriola-Guillen LE, Flores-Mir C. Björk-Jarabak cephalometric analysis on CBCT synthesized cephalograms with different dentofacial sagittal skeletal patterns. Dental Press J Orthod. 2014; 19:46–53.
14. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984; 52:467–474.
15. Orthlieb JD, Laurent M, Laplanche O. Cephalometric estimation of vertical dimension of occlusion. J Oral Rehabil. 2000; 27:802–807.
16. Abduo J, Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012; 57:2–10.
 XML Download
XML Download