

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spinal epidural hematoma (EDH) is a rare entity, but occurs more commonly in association with injuries that mainly accompany ankylosing spondylitis, coagulopathies, post-operative bleeding, or Paget's disease.51012) Upon review of the literature, only a few publications regarding traumatic spinal EDH have been reported compared to spontaneous EDH. Also, this type of traumatic extradural hematoma is typically associated with osseous fracture or the presence of hematological abnormalities. Here, we report a case of traumatic cervical EDH in the absence of osseous fracture and with normal hemostatic parameters. Magnetic resonance images (MRIs) were diagnostic and the patient was successfully treated by emergent hematoma removal. We report a rare case of traumatic cervical EDH, present a review of relevant literature, and discuss the etiology, pathogenesis, and prognosis of this case.
Go to : 
CASE REPORT
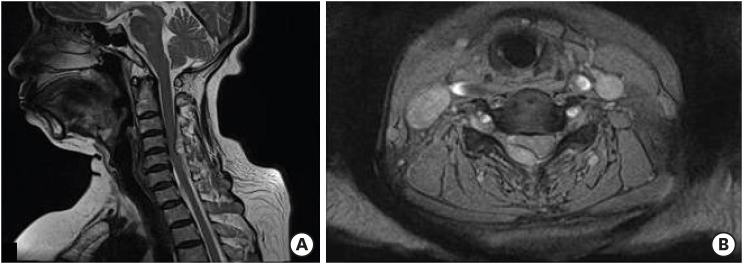
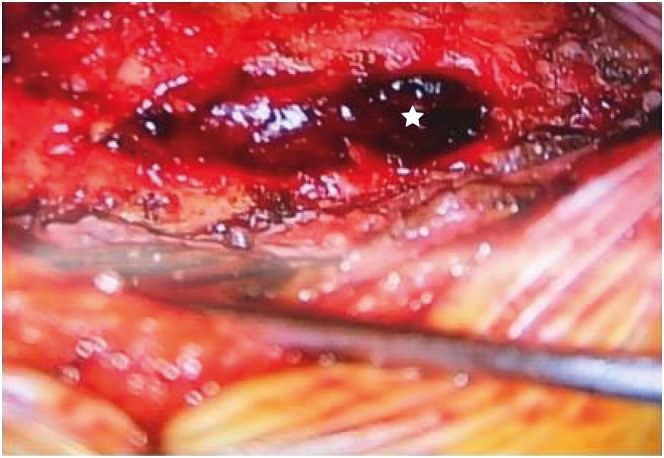
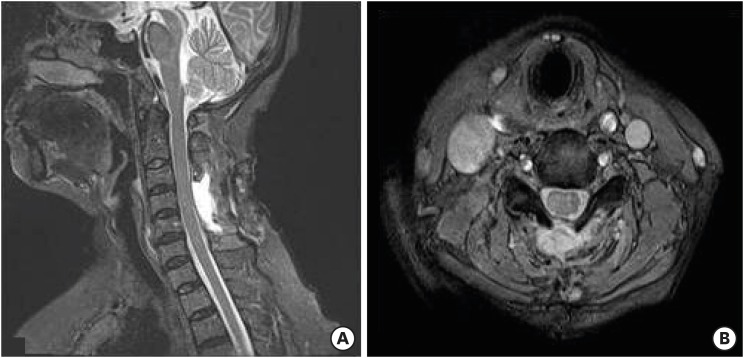
A 47-year-old woman with severe neck pain radiating to the scapula and motor weakness was referred to our emergency room after a car accident. Her symptoms developed immediately after the neck injury and at once she experienced acute dorsal pain. She had no previous history of anticoagulant therapy or hematological coagulopathy, and was in good health before this episode. On neurological examination, she was alert and fully oriented. No neurologic abnormalities were found in cranial nerves or the cerebellar system. However, right side hemiparesis was present with a muscle power of upper limb Grade III and lower limb Grade IV+. Tendon reflexes were absent in right limbs and were slightly hyperactive in the left side. There was no bruise or petechia, and bladder and bowel functions were intact. Paresthesia and slightly reduced sensation to pinprick, light touch, and vibration sensations were noted below the level of the C5 dermatome on the right side. The hematological parameters including platelet count and function of the coagulation cascade were all within normal ranges. Under diagnosis of a cervical lesion, such as, acute disc herniation, emergent radiological studies, including an MRI scan of the cervical spine were performed. Simple radiographs and a computed tomography scan were normal. However, cervical spine MRI revealed a right posteriolateral EDH, from C3 to C5, severely compressing the spinal cord and showing edematous changes (FIGURE 1). Urgent laminectomy and hematoma removal was performed 5 hours after symptom onset. Beneath the ligamentum flavum, liquid dark blood with solid clots was detected and evacuated (FIGURE 2), but no active, discrete bleeding point was identified. Hemostasis was achieved without difficulty. No tumor or vascular abnormality was found in the epidural space. Histopathological examination of the blood clots revealed fibrin deposition but no evidence of malignancy. The right side hemiparesis improved markedly after surgery. The day after surgery, muscle power on the right side had fully recovered and she was able to walk without assistance. MRIs taken 10 days after surgery revealed that the cervical EDH had completely resolved (FIGURE 3). The patient was in good health and free of any neurological deficits at her 6-month follow-up.
This article is about an individual case without the approval of an ethical research. We obtained informed consent from the patient.
Go to :
DISCUSSION
Cervical EDH is a rare pathological entity, which is usually detected by MRI after a cervical fracture and dislocation or in patients with ankylosing spondylitis or a coagulation abnormality.2) Post-traumatic EDH is considered more uncommon compared to spontaneous EDH. The initial clinical manifestations of spinal EDH are back and neck pain, and eventually, compressive myelopathy symptoms. The exact cause of spinal EDH is unknown, but it has been associated with hypertension, anticoagulation, elevated venous pressure, pregnancy, trauma, and vascular malformation.913) In our case, there were no osseous lesions or associated disc bulge, as well as no factors favouring bleeding such as hypertension, arteriovenous malformations, anticoagulant treatment or coagulopathy. No interspinous ligament or spinal muscle rupture was noted preoperatively and intraoperatively. In most cases, the hematoma is located on the dorsal aspect of the spinal cord, which has led to the belief that the posterior epidural venous plexus is the main source of spinal EDH.11) Rupture in the venous plexus during the hyperflexion and hyperextension injury is believed to be caused by reversal of venous flow when intrathoracic or intra-abdominal pressure increases due to excessive strain. The veins in this plexus do not have valves and are vulnerable to rupture by abrupt changes in venous pressure. Also, the rapidity of development of a cervical EDH points toward its arterial origin due to free anastomotic arteries running in the epidural space that also connect with radicular arteries.4) Although degrees of symptoms vary from mild motor or sensory deficit to serious sphincter deficits, spinal EDH can rapidly compromise the spinal cord and result in paralysis or acute deterioration with severe neurologic deficits. Therefore, prompt diagnosis and the determination of hematoma extent are essential.8) Early diagnosis requires clinical suspicion and immediate imaging, and MRI is considered the diagnostic technique of choice. T1-weighted images are most useful due to the signal shift from isointensity with respect to the cord during the early period to hyperintensity in the subacute stage. T2-weighted images are useful for differential diagnosis during the early stage because they can show characteristic focal signal intensity caused by deoxyhemoglobin. The initial clinical features of cervical EDH are neck pain, chest pain, hemiparesis, and sciatic pain with or without subsequent myelopathy. It can resemble those of an acutely ruptured cervical disc, epidural neoplasia, transverse myelitis, acute ischemic stroke, cardiac ischemia, or epidural abscess.7) Spontaneous resolution of spinal EDH without surgery has been reported when neurological deficits are not severe and in cases of rapid clinical improvement.16) However, the treatment of choice for symptomatic cervical EDH is prompt surgical evacuation of the hematoma following laminectomy, and usually achieves favorable results. In general, the earlier the operation, the better the neurological outcome achieved.3)
Go to :
 XML Download
XML Download