

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Traumatic brain injury (TBI) has been the subject of many studies while a variety of attempts have been conducted. Many guidelines and clinical studies have reported the incidence. The pathogenesis and outcome of these injuries differ from study to study, but all could conclude to the importance of management and categorization. However, neither of them reports the fact that reevaluation of the health care system and tight gun control is extremely necessary.
One of the various kinds of TBI is the injury from a gunshot. The first appearance of the gun took place around 1000 AD in China, but its further evolution is multidimensional and eventful.4) Since then, the incidence of gun brain trauma has been increasing, reaching nowadays the level of mortality12)
In this study, the authors present an effort to categorize the traumatic brain injuries due to gunshot in cadavers, comparing the data from Greece and Bulgaria. The main purpose of the study is to observe and thereafter to evaluate important clinical and autopsy findings of subjects suffering from the same pathology- penetrating brain injury, for which there are no similar reports.
Go to : 
MATERIALS AND METHODS
The records are collected from 2 laboratories of forensic science and toxicology. The first is located in hospital “Stamen Iliev,” in Montana, Bulgaria, while the second in the university hospital of Alexandroupolis, Greece.
The laboratory of forensic science in Bulgaria examines patients and cadavers from the western half of North-West Bulgaria, including 2 regions—Montana and Vidin with a few municipalities (Vidin, Lom and Montana). The university hospital, on the other hand, examines patients and cadavers from the region of East Macedonia and Thrace that include 5 regions—Evros, Rhodope, Xanthi, Kavala, and Drama.
The law in both countries stipulates that an individual might own a weapon, based on solid grounds (reasoning), after proper psychiatric evaluation has been conducted and a license from the police has been issued. Many of the subjects had licenses for weapon ownership, while few of them had an access to such. The fact that all of them were victims of suicide and all of them had an access to gunshot weapon, despite their psychological condition, suggest that better weapon control or healthcare is highly required.
The study is based on the retrospective analysis of the archived protocols from 1 January 2007 to 31 December 2016 from both centers, therefore an informed consent was not needed. The total number of fatal TBI collected from the laboratories of forensic science and toxicology for this period is 233 in Montana/Vidin and 228 in North Greece. The basic concept of the study is the analysis and comparison between both countries on the subject of gunshot brain injury in cadavers. Due to that we excluded every other cause of TBI, as well as cases of living patients. Subsequently, the authors compared three basic categories—demographic, anatomical localization and cadaveric findings.
Under the term “demographic” we included data based on the age, sex, location of the incident and toxicological result.
Under the term “anatomical localization” we concluded anatomical landmarks of the skull, number of skull injuries, open or closed trauma and morphology of the head trauma. Finally, under the term “cadaveric findings” we concluded autopsy findings, such as brain edema, atherosclerosis of the vessels, old scar tissue etc.
Afterwards, the data is analyzed on Jeffreys's Amazing Statistics Program (JASP) statistical program, including Correlation analysis and t-paired tests.
Go to :
RESULTS
Demographic
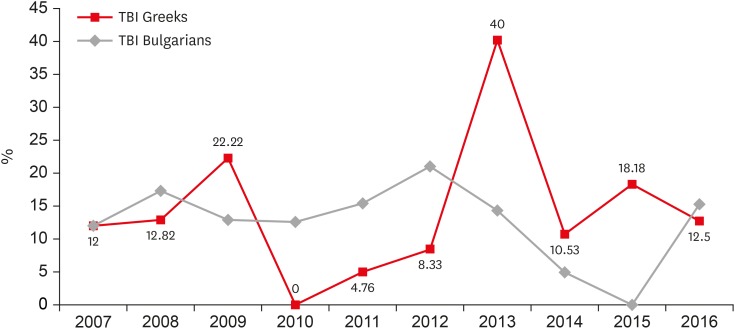
After evaluating the collected data, the authors analyzed 30 cadavers (12.88%) from the both regions in Bulgaria and 31 (13.60%) from Greece, with death caused by a suicide attempt, and no one due to a criminal act. All of them, however, represent the fatality of the penetrating brain trauma for a 10-year period of time in the specific regions. The allocation and percentage of the gunshot TBI per year differ between the 2 countries and it is presented in FIGURE 1. The average number of fatal accidents for the 10-year period is 12.58% in Bulgaria and 15.04% in Greece.
The average age of the Bulgarians is 45.62 years with age ranging between 15 to 75 years. From the 30 cadavers that were examined, 29 (96.67%) are males and only one is female (3.33%). Twenty-seven (90%) are located in Montana (25 males and 1 female), 2 in Lom (6.67%) and 1 in Vidin (3.33%). Furthermore, 3 died (10%) in the hospital and 27 at the local point of the incident (90%).
On the other hand, the average age of the Greeks is 50.54 years with age varying between 19 and 87. From the aforementioned 31 dead bodies, 30 are males (96.77%) and one is female (3.23%). Twenty-four were found in Evros (77.42%), 5 in Rhodope (16.13%), 1 in Kavala (3.23%) and 1 in Xanthi (3.23%). Additionally, 5 died in the hospital (16.13%) and 26 died at the local point of the incident (83.87%).
At this point, it should be mentioned that under the term “hospital” the authors do not mean only a specific department but everyone from the emergency room to the laboratory of forensic science and toxicology.
Finally, 15 (51,72%) from the Bulgarian males and 12 (40%) from the Greek males had consumed alcohol while 6/12 (50%) had used other substances such as benzodiazepines or opiates combined with alcohol. The 2 females, 14 Bulgarian and 18 Greek males did not consume any toxic substances before the accident (TABLE 1).

Anatomical
Further categorization of the TBI is open/close trauma, number of injuries (1, 2, or multiple), size and morphology and anatomical localization on the skull. From the gunshot forensic science investigation, all of the individuals had an open TBI (100%). 2 subjects among the Bulgarians and 8 among the Greeks did not have an exit wound.
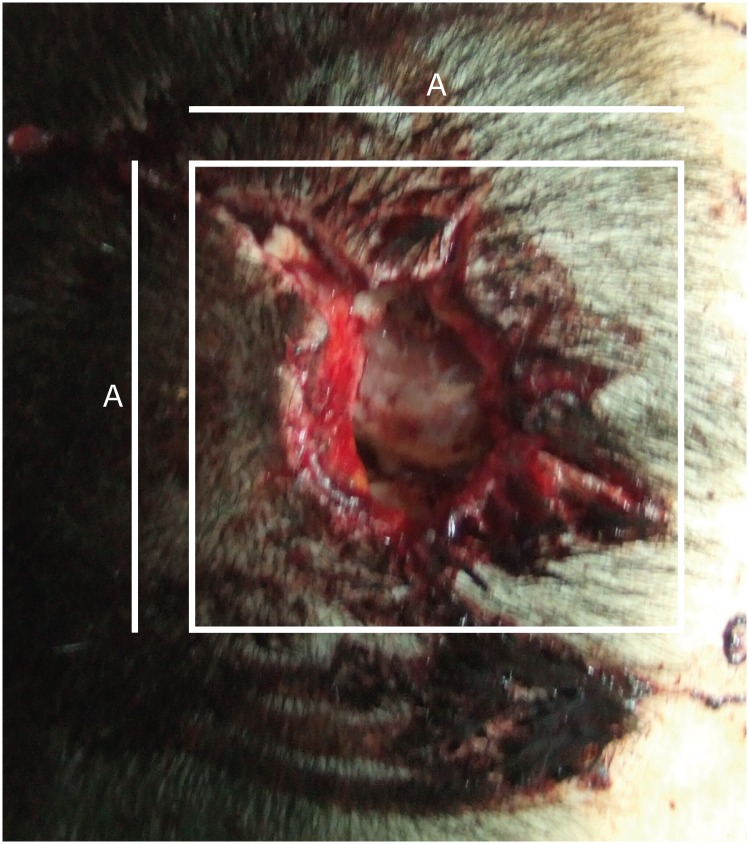
As far as the Greeks are concerned, the size of the PBIs ranged between 0.5 and 10 cm. Assessing these measurements, it could be concluded that the trauma on the skull after gunshot had mainly a square morphology, helping us to understand the trajectory of the gunshot (S= a×a) (FIGURE 2).
On the other hand, in Bulgaria were found mainly rectangular—shaped injuries on the skull. The size ranged from 0.5 to 17 cm. (S=a×b)
It should be mentioned that by the given circumstances (suicide attempt), when the bullet entered the skull, it produced a bigger exit wound than the entry one, because of the close range of the shot, mainly in those who had 2 injuries.
Among the Bulgarians, the skull base constituted the most common region of injury while in the Greeks the latter was represented by the facial bones (TABLE 2). Second most common localization was the temporal bone in Bulgarians and the splachnic skull in the Greeks. The anatomical localization could determine easily the trajectory of the shot. Most of the individuals with skull base trauma had also a facial and occipital one, and consequently we can conclude that the gunshot was fired from the anterior—inferior to the posterior –superior part of the head, traumatizing the relevant bones and anatomical structures.
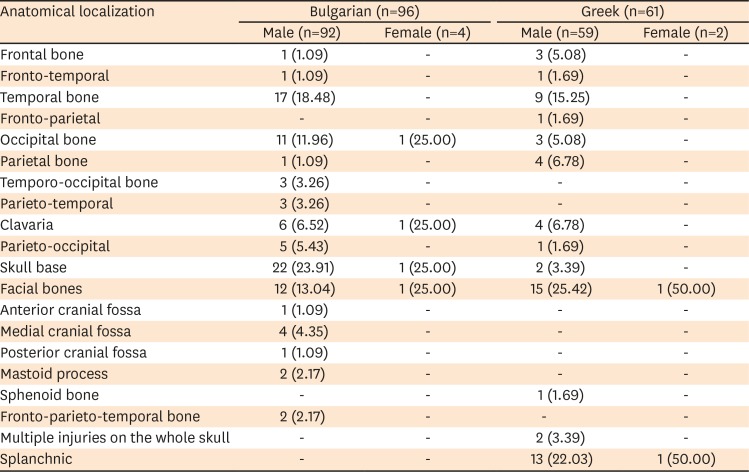
TABLE 2
Anatomical localization on the skull
![]()
Other observed trajectories are between both temporal bones either from left to right or reversely, penetrating anatomical structures of both hemispheres; from the frontal bone through the clavaria, traumatizing the cortex; and injuring through the parietal bone without exit wound or injuring the structures in vertical way.
The morphology of the skull trauma, as well as its localization (temporal, frontal, etc) have impact on the extent of the craniotomy. The bigger the craniotomy, the higher the rates of morbidity and complications. The patients with exit wound increase enormously the aforementioned rates, because of the need of extensive craniotomy and the fact that the trajectory of the shot has damaged a great part of the brain tissue, causing in most cases permanent damage to the brain structures.
Cadaveric
As far as the cadaveric or additional findings are concerned, the authors included all the findings that were made during the autopsy. The latter are classified in 2 different categories. The first is based on the results which are derived from the central nervous system (CNS) and the second from every other organ (TABLE 3 & 4).
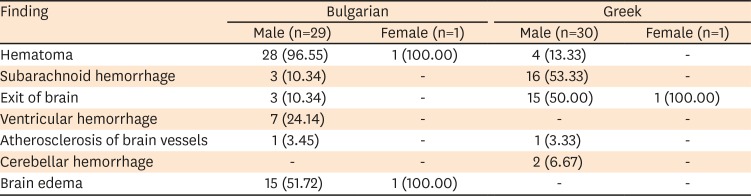
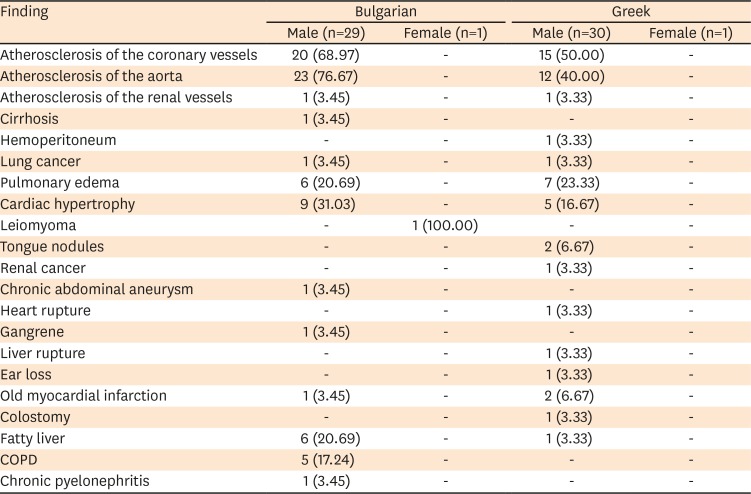
TABLE 3
Comparative autopsy findings of the central nervous system
![]()
TABLE 4
Autopsy findings and comparison between the sites
![]()
Regarding the CNS results, a cross-match between subarachnoid hemorrhage and brain hematoma between both groups, which could not be processed as a difference because of its origin is observed. The only difference is the time interval which has mediated (TABLE 3).
After processing the data on other than CNS organs, it is derived that there is a sufficient difference between the individuals. As it can easily be observed in TABLE 4, atherosclerosis of the coronary arteries and the aorta is more common among Bulgarians and presents the most distinguished difference. A quite interesting point is that Bulgarians suffer more frequently from atherosclerosis of the aorta (79.31%) than the coronary (68.97%), in contrast to the Greeks, who present more frequently atherosclerosis of the coronary, compared to that of the aorta. Another important difference regarding the circulatory system is the cardiac hypertrophy observed mainly among Bulgarians (31.03%), compared to the percentage among the Greek population (16.67%).
Go to :
DISCUSSION
To summarize, our study shows that despite the fact that PBI has the same cause—gunshot, while the guidelines suggest similar therapeutical approaches, the difference between the subjects should be taken under consideration for further investigation and prevention.
Alcohol consumption, age, extended injury of the skull and brain tissue and high rate of co-morbidities are all factors increasing the mortality rate. All of the subjects of the current study had more than one of those factors contributing to the fatal result of the PBIs. More important, due to the cause of the PBIs in the current study, it could be suggested that better healthcare is highly required to prevent and cure this type of brain trauma, including better psychiatric evaluation and post-traumatic management.
The study reports very important facts, but has the limitation that it is conducted for only a small region from each country and more detailed national investigations are highly required. Despite that fact, it observes an important issue regarding gun control, health care system, the current criminal code and most significant—the importance of personalized therapeutical approaches, including also preventative measures.
Penetrating brain trauma is a serious issue not only because of its origin but also due to its high mortality rate and post-traumatic complications. The basic factor behind this, is the trajectory of the gunshot through the skull.2,11) The more domains being injured, the worse the outcome becomes. Hence, the bihemispheric and transventricular trajectory seem to be linked to poorer results.2,11) Other factors for the outcome and the mortality are the existing or post-traumatic co-morbidities2) and the cause of the wound (suicide attempts are linked to higher mortality).6) Our study shows primarily results for poorer outcome—mainly suicide attempts with bihemisphreric brain trauma—covering more than one anatomical structure and bone and plenty of co-morbidities.
As far the demographics are concerned, according to a study made by Izci et al.,5) who examined only male patients, the average age of the participants in the study is 22. Another study, conducted by Liebenberg et al.7) with 125 participating patients, shows male predominance with an average age of 24.9. Solmaz et al.,9) investigating 442 patients, concludes male prevalence in gunshot TBI with an average age of the patients being 23.2 years. On the contrary, the authors of this study observed higher numbers of the average age (45.62 and 50.54) in both nationality groups, but also a definite male dominance (96.72%). According to Esposito and Walker,3) higher numbers of age are linked to poorer results. Finally, regarding the topic of toxic substances and alcohol, Tien et al.10) revealed that patients with brain trauma and alcohol consumption had worse results compared to those who had consumed any of the above. On the other hand, cocaine seems not to play a role in the results and the mortality.13) Our study showed that 44.26% had drunk alcohol and 22.22% combined it with opiates and/or benzodiazepines. The conclusion whether the drugs lead to a poorer outcome will not be reliable because of the existence of other factors and the additional use of alcohol.
It seems that as far as the topic of open/closed trauma is concerned, all of the studies include open traumas.1,5,7,9) Regarding the anatomical localization, the results vary. Andrade et al.1) showed in his study that the most frequently involved parts of the skull are frontal (38%), temporal (28%) and parietal (12.5%). Lin et al.8) in his case-series shows that common localizations are parietal, occipital, temporal bones and skull base. Solmaz et al.9) on the same subject reaches the conclusion that frontal, temporal and parietal bone are the most frequently injured parts, but the trauma of the posterior fossa and the multiple injuries lead almost certainly to death. In the current study we observed that the most commonly injured region is the face, followed by the skull base. These findings are very important not only to determine the trajectory of the gunshot and the cause of death, but also for management planning, including hospital administration and hospital staff organization.
Other findings after/due to penetrating TBI are derived to be subarachnoid hemorrhage, ventricular hemorrhage, subdural hemorrhage, and hematoma, linked to the trajectory of the bullet.1,8) Results with prognostic significance, however, are brain swelling, lesions and vascular events.1) As it is depicted in TABLE 3 & 4, our study also reports a great number of hematomas, subdural hemorrhages and brain swelling. At this point it should be mentioned that, no other study has revealed similar findings after the autopsy in addition to the number of head injuries as the ones derived from this particular which is thoroughly described above.
Go to :
CONCLUSION
In conclusion, brain trauma due to gunshot is one of the most dangerous kinds of brain injuries. Tracking the 10-year cadaveric findings among 2 nations suggests that indeed there are differences among the nations, including trajectory, age and alcohol consumption, but also there is a common fact that there should be present better preventative measures, including gun control and healthcare system.
Go to :
 XML Download
XML Download