

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An arachnoid cyst (AC) is a developmental anomaly often diagnosed in childhood as incidental findings on imaging.1) It is usually asymptomatic but occasionally produces symptoms because of increasing size or a newly appearing hematoma.16) It is now generally accepted that young patients with ACs are at a higher risk of developing a chronic subdural hematoma (CSDH) after minor head injuries.5) Although there have been controversies associated with the treatment, many researchers have considered the two as separate lesions and recommend draining only the CSDH when the AC is asymptomatic.21017)
ACs usually remain unchanged after the removal of a CSDH.29101113) However, we recently experienced a case in which an AC completely disappeared after only draining the CSDH. In this case report, we discuss possible mechanisms of such a phenomenon and the proper management of patients with both a CSDH and an AC with a review of relevant literature.
Go to : 
CASE REPORT
A 15-year-old man visited our hospital for a facial contusion that occurred during a bicycle accident. He was alert and showed no focal neurologic deficits or signs. His brain computed tomography (CT) showed only an AC located at the right high frontal convexity, and no trauma-related lesion was observed (FIGURE 1A). He recovered well.
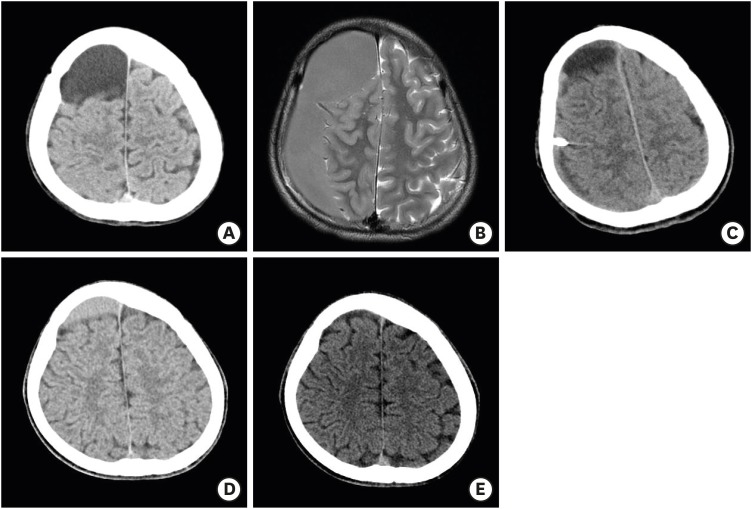 | FIGURE 1(A) Brain CT taken immediately after a facial contusion after the initial bicycle accident. An AC at the right high frontal convexity with an inner-skull indentation without any trauma-related lesions was observed. (B) Brain T2-weighted axial magnetic resonance imaging performed 2 months after the initial facial injury. A CSDH at the right cerebral convexity with midline shifting was observed. The signal intensities of both the AC and the CSDH were the same, and no membrane between them was observed. (C) Brain CT taken immediately after the surgery. The CSDH was well drained, and the AC showed a decrease in size with a cerebrospinal fluid-like density. (D) Follow-up brain CT scan taken 4 months after the surgery. The CSDH disappeared completely, and the size of the AC was more decreased. A change in the fluid density of the AC was noted. (E) Follow-up brain CT scan taken 7 months after the surgery. The AC had disappeared completely with full brain expansion.CT: computed tomography, AC: arachnoid cyst, CSDH: chronic subdural hematoma.
|
Two months later, the patient suffered a mild head trauma during exercise at school, and a severe headache followed. No focal neurologic deficits were observed. His brain magnetic resonance imaging revealed a CSDH at the right convexity with midline shift to the left. The fluid signal intensity of the AC was the same as that of the CSDH (FIGURE 1B). We performed a burr hole drainage of the CSDH without any manipulation of the AC membrane. The immediate postoperative CT scan showed that much of the hematoma was removed. The size of the AC was decreased, and its fluid density was changed so that it was close to that of the cerebrospinal fluid (FIGURE 1C). The headache improved immediately after the surgery. His hospital stay was uneventful, and he was discharged 8 days later. A follow-up CT scan, performed 4 months after the surgery, revealed a larger decrease in the size of the AC, and the fluid component changed again, similar to a subacute hematoma (FIGURE 1D). Three months later, another follow-up CT scan showed that the AC had completely disappeared with full brain expansion (FIGURE 1E).
This report had been reviewed after gaining the Institutional Review Board approval for the patient consent exemption.
Go to :
DISCUSSION
CSDHs are commonly associated with cerebral atrophy, and they tend to occur in elderly patients with a history of mild head injuries. It is a rare manifestation in children and young adults, and it is extremely rare for one to occur without a trauma. The presence of an AC puts young patients at an increased risk of developing a CSDH after a minor head injury.3) With cumulative evidence, the causal relationship between ACs and CSDHs has been widely accepted.25101617) Data have shown that patients at their 2nd decade of life have the highest risk of AC-associated CSDH.17)
Many authors have proposed the underlying mechanism of AC-associated CSDH.24581516) These hypotheses are based on two basic observations.17) One observation is the intraoperative finding of small bridging vessels between the dura and outer membrane of the AC or vessels that transverse the AC membrane. The other observation is the lower compliance of AC compared with normal brain tissue, resulting in reduced intracalvarial cushioning following a mild head injury. When a head injury occurs, the bridging vessels or the AC membrane can easily rupture, which leads to an asymptomatic hemorrhage, which will later become a CSDH.
Although there have been many reports on AC-associated CSDH and its treatments,24589101113151617) few authors have been interested in the fate of the AC after surgery. We think this disinterest is because most ACs were asymptomatic at the time of CSDH symptom presentation, and postoperative clinical outcomes were favorable in most cases regardless of the surgical methods. However, we retrospectively found that in several reports, ACs remained unchanged after surgery.29101113) In addition, based on this observation, we presume that many authors who have recommended only draining a CSDH without manipulating the AC membrane regard ACs and CSDHs as separate lesions.2)
There have been few reports of a decrease or disappearance in ACs after a minor head injury.67121418) Intracystic or subdural hemorrhage occurred in some cases. Unlike our case, most of them did not need surgical intervention. Most authors agree that AC resolution can be attributed to the rupture of the AC membrane. The arachnoid membranes of the cyst are easily torn by minor head injuries.67) The fluid content of the cyst may then flow into the subdural space, forming a subdural fluid collection. This phenomenon may result in a CSDH by a rupture of the bridging vessels.6) After the removal of the CSDH by either surgical evacuation or spontaneous absorption, the cyst cannot be maintained due to the disruption of its membrane, and it disappears as the brain expands. We think that a similar process occurred in our case. It is unclear whether the CSDH occurred inside or outside of the cyst. However, either situation led to the rupture of the AC membrane, and the AC disappeared after the burr hole drainage of the CSDH with subsequent brain expansion (FIGURE 2). However, the exact mechanism has not been elucidated since the disappearance of an AC is a rare event, and we do not yet know under what conditions the AC might disappear after the removal of a CSDH.
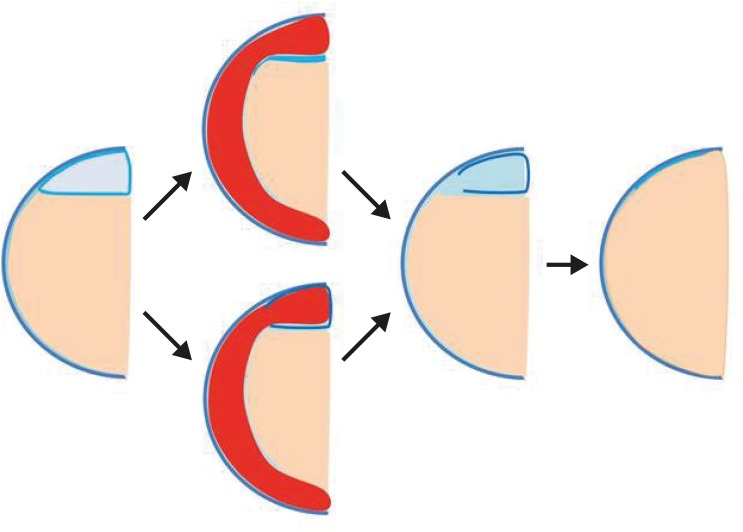 | FIGURE 2Illustrations of the AC associated with the CSDH. A CSDH (2nd step, drawn as red color) may occur either outside or inside the AC after a head injury. CSDH occurring outside (2nd step, upper), the AC would be crushed flat and rupture. CSDH occurring inside (2nd step, lower), it would expand and rupture. In either case, a connection between the cyst and the subdural space is established. After the removal of CSDH, the pressure of the AC disappears (3rd step). Gradual brain expansion follows, leading to disappearance of the AC (4th step).AC: arachnoid cyst, CSDH: chronic subdural hematoma.
|
In summary, an AC might disappear after the removal of an AC-associated CSDH, and the probability may increase when the cyst membrane is ruptured. Therefore, in such patients, planning serial follow-up examinations is recommended since the presence of an AC is still a risk factor for developing another CSDH. For the treatment of an AC-associated CSDH, it seems more reasonable to drain only the CSDH irrespective of the fate of the AC after the surgery. Since there have been some reports of spontaneous absorptions of AC-associated CSDHs,67) careful observations without surgical intervention could be favored if any CSDH-related symptoms are not present.
Go to :
 XML Download
XML Download