

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Diabetes mellitus (DM) is a common metabolic disorder that increases blood glucose levels. The number of patients with DM has steadily increased over the past several decades due to population growth, higher average age of the population, and increasing prevalence of DM by age. Furthermore, the worldwide prevalence of DM increased from 4.7% in 1980 to 8.5% in 2014, which increased or remained almost unchanged in all countries during that period. In 1814, the World Health Organization estimated that 422 million adults will suffer from DM in 2014 worldwide, reaching 108 million in 1980.12) Because of the constant increase in the number of patients and the high penetration rate, care for patients with DM is critical and very relevant for the management of patients undergoing spinal surgery.
Several previous studies demonstrated that DM has been associated with poor postoperative outcomes and high postoperative complications.34567891011) Lumbar fusion is extensively used in various pathological conditions, and complications are more common than other spinal surgery due to a wide range of scales.34) Among the various complications of spinal surgery, surgical site infection (SSI) is one of the most common that results in severe problems that increase social, economic, and personal expenditure. Some studies reported that DM is a significant risk factor for SSI after spinal fusion.79121314)
Because DM is a chronic disease that causes postoperative complications in patients undergoing spinal surgery, adequate blood glucose levels should be maintained over a long time period. The management of patients with DM can be monitored in many ways, such as the use of glycated hemoglobin A1c (HbA1c), traditionally used as an indicator of adequate blood glucose control.15) HbA1c levels are simple objective laboratory figures that provide a comprehensive view of the patient's blood glucose status over 2–3 months.16) However, studies on how glucose control affects the risk of SSI after lumbar surgery, as evidenced by the HbA1c, has been limited.717)
There are many reports of increased risk of SSI with diabetes. On the other hand, if the diabetes were strictly controlled, the risk of SSI would be diminished much less than when not adjusted. So, we used HbA1c as an indicator of regulation, we present a relationship between diabetes control and infection and cutoff values that divide it.
Go to : 
MATERIALS AND METHODS
Patients
From January 1, 2009, to December 31, 2015, medical records of 251 patients who underwent lumbar interbody fusion with recorded preoperative HbA1c levels were retrospectively reviewed. The inclusion criteria were divided into 3 parts: single-level fusion, patients with DM, and conventional open screw-technique with posterolateral fusion surgery. The fusion segment was L4/5 or L5/S1. The HbA1c level was evaluated throughout the pre-surgical state until 4 weeks postoperatively. All enrolled patients were divided into 2 groups based on the occurrence of SSI. The demographic and clinical data between the 2 groups were compared.
Data collection
The patient's age, sex, body mass index, hospitalization date, smoking history, preoperative HbA1c, American Society of Anesthesiologists (ASA) classification, fusion level, follow-up period, estimated blood loss (EBL), and transfusion during surgery were analyzed.
Identification of postsurgical infection
SSI was defined as a deep surgical infection that occurred within 1 year after the implant placement, a superficial infection that occurred within 30 days, using the Centers for Disease Control and Prevention guidelines.18)
Statistical analysis
The χ2 test or Fisher's exact test was performed for categorical values, and Student's t-test or Mann–Whitney U test for independent continuous samples, as appropriate. To determine the cut-off value of HbA1c, receiver operating characteristic (ROC) curve analysis was used, which showed that HbA1c level increases the risk of SSI. In this study, the optimal threshold was defined as the point on the ROC curve where the product of sensitivity/specificity pair reached its maximum value. Subsequently, preoperative HbA1c level was converted to a binary variable (above and below the threshold). To determine the independent risk factors for SSI, multivariate binomial logistic regression analysis was used to control the effects of confounding variables. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA).
Ethics statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of Institutional Review Board (IRB) of the hospital (IRB No.05-2018-044) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study protocol was approved by the IRB of the local hospital; the requirement for informed consent was waived due to the retrospective nature of this study.
Go to :
RESULTS
A total of 92 patients were included in this study and divided into SSI (group S, n=24) and SSI-free group (group NS, n=68) (FIGURE 1). Univariate analysis showed no significant difference between the 2 groups, except for HbA1c levels and hospitalization period (TABLE 1). Preoperative HbA1c levels were significantly higher in patients with SSI (6.78%) than those without (5.99%, p=0.003). The hospitalization period was 45.8 days in group S and 19.3 days and 2.4 hours in the NS group (p=0.003). Three of 24 (12.5%) patients developed deep SSI requiring surgical irrigation and resection. The other 21 cases had surface incision type SSI, and no patients had organic SSI.
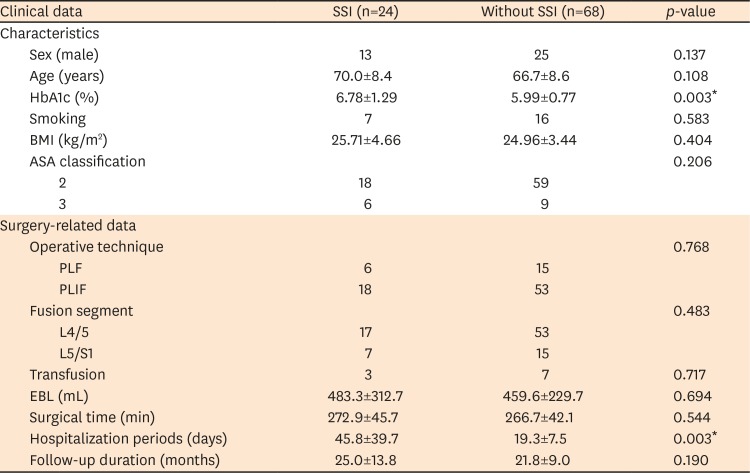
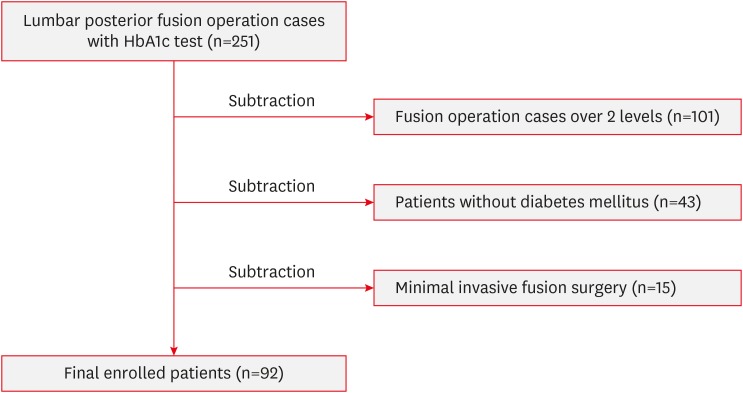
TABLE 1
Demographic and clinical characteristics of the study groups
Student's t-test, Mann–Whitney U test, χ2 test, or Fisher's exact test was used, as appropriate.
SSI: group of patients with surgical site infection, Without SSI: group of patients without surgical site infection, BMI: body mass index, HbA1c: hemoglobin A1c, ASA: American Society of Anesthesiologists, PLF: posterolateral fusion, PLIF: posterior interbody fusion, EBL: estimated blood loss.
*Statistically significant value.
![]()
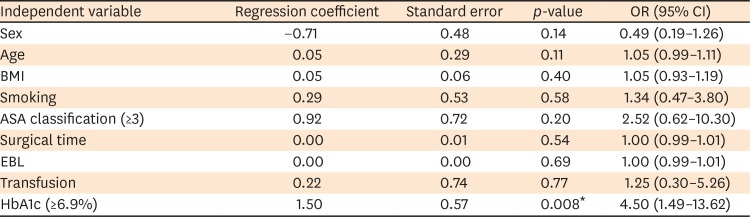
The result of ROC analysis showed that the optimal threshold was HbA1c level of ≥6.9% (p=0.003; AUC, 0.708; sensitivity, 62.5%; specificity, 70.6%), when the risk of SSI was significantly increased (FIGURE 2). The significance and possible confounding factors were assessed by performing a multivariate binomial logistic regression to bisect HbA1c and calibrate all other covariates using thresholds (HbA1c <6.9% and HbA1c ≥6.9%). Eventually, only the HbA1c threshold level was significantly associated with SSI (p=0.008; odds ratio [OR], 4.50; 95% confidence interval [CI], 1.49–13.62) (TABLES 2 & 3).

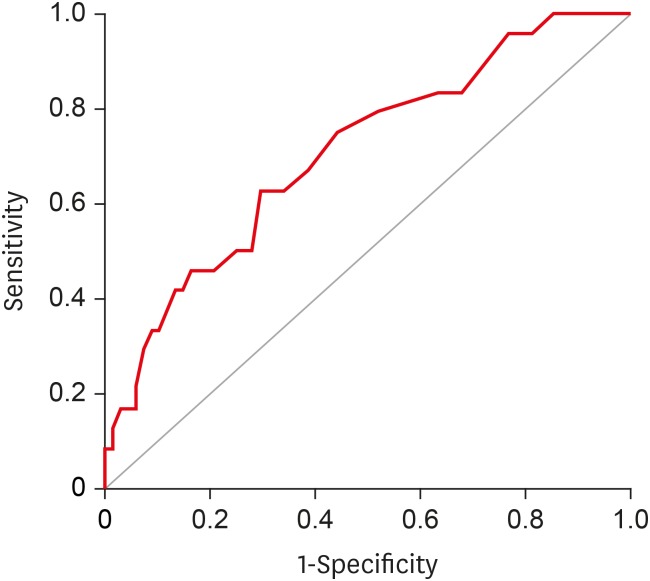 | FIGURE 2Result of the ROC analysis; the optimal threshold was HbA1c of ≥6.9% (p=0.003; area under the curve, 0.708; sensitivity, 62.5%; specificity, 70.6%), when the risk of surgical site infection was significantly increased.ROC: receiver operating characteristic, HbA1c: hemoglobin A1c.
|
TABLE 2
Univariate logistic regression analysis of SSI
SSI: group of patients with surgical site infection, OR: odds ratio, CI: confidence interval, BMI: body mass index, HbA1c: hemoglobin A1c, ASA: American Society of Anesthesiologists, EBL: estimated blood loss.
*Statistically significant value.
![]()
TABLE 3
Multivariate logistic regression analysis of SSI
| Independent variable | Regression coefficient | Standard error | p-value | OR (95% CI) |
|---|---|---|---|---|
| HbA1c (≥6.9%) | 1.50 | 0.57 | 0.008* | 4.50 (1.49–13.62) |
SSI: group of patients with surgical site infection, OR: odds ratio, CI: confidence interval, HbA1c: hemoglobin A1c.
*Statistically significant value.
![]()
Go to :
DISCUSSION
DM is a well-known underlying disease that remains a burden on the healthcare system. Moreover, with the increasing trends of older populations and DM prevalence, spinal surgeons or other healthcare providers commonly face patients with DM. In particular, SSI is one of the most common and severe postoperative complications, and patients with DM may have a much higher risk of SSI than the general population. Recent systematic reviews and meta-analyses have reported a 53% increase in the proportion of SSI in patients with DM.19) The prevalence of infectious complications in patients with spinal stenosis varies from 0.7% to 12%. The National Nosocomial Infections Surveillance study reported that infectious complications occurred in 2.1% of patients with spinal arthrodesis.820) Several studies have identified DM as one of the high-risk factors for SSI after a spinal fusion.79121314) Therefore, to reduce the risk of SSI, it can be inferred that strict preoperative glucose control is necessary for patients with DM undergoing spinal fusion.
Various methods are available to assess blood glucose control in a planned patient with DM. Among these methods, HbA1c is the most preferred because it allows an integrated assessment of blood glucose control status for 2–3 months.16) Many studies have also been conducted on the relationship between preoperative HbA1c levels and postoperative infectious complications in various types of surgery. For example, in the orthopedic literature, strictly maintained HbA1c levels had been demonstrated to be associated with reduced frequency of postoperative infectious complications after a total arthroplasty.212223242526) However, only few studies evaluated the glucose control level using HbA1c levels as a risk factor for SSI after this kind of lumbar surgery.717)
Besides, there is no evidence to date that such HbA1c level markedly increases the risk of SSI in patients with DM undergoing lumbar fusion surgery. To the best of our knowledge, this is the first study to examine the association between SSI and preoperative HbA1c levels after single-level lumbar interbody fusion in patients with DM. A ROC analysis was also performed to determine the optimal threshold of HbA1c levels for significantly increased risk of SSI.
Following another study, the occurrence of SSI and HbA1c level was associated with posterior thoracic and lumbar surgery.7) Among 36 patients with DM, the prevalence of HbA1c was significantly higher in patients with SSI (7.6%) than those without SSI (6.9%: p=0.006). In this study, patients were also classified as having controlled (HbA1c <7.0%) and uncontrolled DM (HbA1c ≥7.0%) according to the criteria described by Adams et al.21) SSI occurred in 6 out of 17 patients (35.3%) with uncontrolled DM but not in the controlled DM group (p=0.006). Therefore, preoperative uncontrolled DM acts as an independent risk factor for SSI after a posterior spinal arthroplasty. This study identified a significant difference in preoperative HbA1c levels between patients with and without SSI; however, its clinical relevance was limited by the lack of statistical power to assess the outcome as a threshold.
A similar study was conducted to assess the relationship between glucose control and postoperative infection in patients with DM undergoing a single-level decompression.17) Likewise, we identified a national database of patients who underwent primary and single-level lumbar decompression in patients with DM who had had preoperative HbA1c levels within 3 months of surgery. The group analyzed a total of 5,194 patients and evaluated postoperative infection rates that required surgical intervention within 1 year of exponential surgery. The results of this study showed that HbA1c levels increase the risk of severe postoperative infection after a single-level lumbar decompression in patients with DM (p=0.012). ROC and multivariate regression analysis showed that the preoperative HbA1c level of >7.5 mg/dL was significantly associated with deep infection (p<0.0001; OR, 2.9; CI, 1.8–4.9).
However, since this study used the diagnostic and procedural codes of the management database, non-coding and miscoding can cause severe errors and limit its clinical applicability. Studies have also been conducted using HbA1c levels, patient demographics, and medical complications; however, other actual surgical factors affecting the SSI risk were excluded because they could not be extracted from the database.
In the current study, the prevalence of HbA1c levels was significantly higher in patients with SSI than in 6.0% (p=0.008) (6.8%), as also reported by Hikata et al.7) Our ROC analysis showed that the prevalence of HbA1c of ≥6.9% might be the effective threshold value when the SSI risk significantly increased (p=0.003; AUC, 0.708; sensitivity, 62.5%; specificity, 70.6%).
Contrary to Cancienne et al.'s17) report, we investigated surgical factors such as ASA classification, operative time, EBL, and transfusion, and then performed a multivariate logistic regression analysis to identify potential disturbances. As a result, only the HbA1c threshold level showed statistically significant association with SSI (p=0.008; OR=4.500; 95% CI, 1.486–13.624).
In patients undergoing elective surgery, determining the appropriate goal of preoperative glucose control is clinically significant; however, there is no objective and reliable threshold for HbA1c. Concerning the current HbA1c level goals, the American Diabetes Association recommends less than 7.0%, and the American Clinical Endocrinologists Diabetic Guidelines recommends 2.13 years, less than 6.5%.2728)
These goals are consistent with the results of this study, as well as those mentioned above. In this study, the institutional database allows the collection of homogeneous groups of patients who underwent a single-level lumbar back fusion. Our statistical analysis itself might have insufficient diagnostic value of HbA1C threshold because of the low AUC value. However, it might be helpful to determine the optimal threshold of HbA1c to prevent the SSI risk increase.
We acknowledge that some limitations are inevitable in this study. First, despite satisfactory statistical results in a separate analysis, the sample size was considered small, and results should be carefully interpreted in advance. Second, this study is limited to a single institution and may require additional validation in future multicenter studies. Third, specific information about DM itself (e.g., DM type, treatment method, and duration of illness) was not included. Fourth, between-group differences regarding our data on SSI risk were not significant; however, other important factors such as nutritional status, steroid therapy, and previous spinal surgery were not controlled. Finally, this study is limited to a retrograde analysis; therefore, data can be subject to selection bias and negotiation. However, the expected error has been tried to minimize by including all consecutive cases that meet the selection criteria within the specified baseline time as possible criteria. More prospective studies are needed to confirm our results and SSI risk reduction with improved blood glucose control.
Go to :
CONCLUSION
The specific HbA1c level in patients with DM is an independent risk factor for surgical infection after a single lumbar fusion surgery. Furthermore, ROC analysis can be used as a threshold for a significant increase in the risk if preoperative HbA1c level is >6.9%. In conclusion, preoperative HbA1c level is a reliable predictor of SSI after single a lumbar fusion surgery; therefore, blood glucose control based on HbA1c level of <6.9% is recommended for patients undergoing surgery.
Go to :
 XML Download
XML Download