

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spinal infection refers to infectious conditions affecting the vertebral body, intervertebral discs, or other paravertebral tissues.121316) The incidence of spinal infection is increasing owing to increases in non-surgical and surgical treatment options for spinal disease. However, despite the increase in spinal infections, not much development has been made in developing diagnosing tests and assessing the efficacy of antibiotics. Spinal infection is diagnosed through physical examination, laboratory tests, or radiologic studies. Typical laboratory tests performed to diagnose spinal infection include white blood cell (WBC) counts, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP).345101112141516)
Procalcitonin (PCT) is also used as a laboratory biomarker to distinguish bacterial and non-bacterial infections, but research on PCT in spinal infection is lacking.25781220212223) Therefore, this study aimed to compare changes in PCT and other laboratory biomarkers in patients with spinal infection. Moreover, this study also seeks to confirm more sensitive biomarkers of antibiotic efficacy.
Go to : 
MATERIALS AND METHODS
ESR, CRP, WBC counts, and PCT were measured in 29 patients diagnosed with pyogenic spinal infection on radiographic and histological tests conducted at our hospital between May 2016 and December 2018 prior to antibiotic administration. After antibiotic administration, the values were followed up for 4 weeks at 1-week intervals. Patients with comorbid infections in other areas, lacking laboratory results, or with tuberculous spondylitis were excluded through the retrospective review of medical records. This study was conducted with the approval of our Institutional Review Board (CNUH 2019-06-047). The requirement to obtain written informed consent for study participation was waived.
Bacteria were identified through blood culture and tissue from bone biopsy. When bacteria were identified, antibiotics to which the bacteria were sensitive were used, and empirical antibiotic therapy was provided when bacteria were not identified. The serum concentration of vancomycin should be maintained at 15–20 µg/mL.
ESR was measured using the Westergren method, CRP through photometric latex agglutination, PCT through enzyme-linked fluorescent assay, and WBCs through Coulter method on UniCel DxH 800. The laboratory result was averaged each week, and changes in the slope of weekly change were assessed through repeated ANOVA measures, with p-value of <0.05 considered statistically significant. Statistical analysis was conducted using the SPSS version 21.0 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
A total of 29 patients were enrolled, with a mean age of 67.8 years, consisting of 16 men and 13 women. Twenty-five patients had lumbar infections, and two each had cervical and thoracic infections. Regarding the patients' previous medical history, 7 had diabetes, 14 had hypertension, and 1 had chronic kidney disease (TABLE 1).
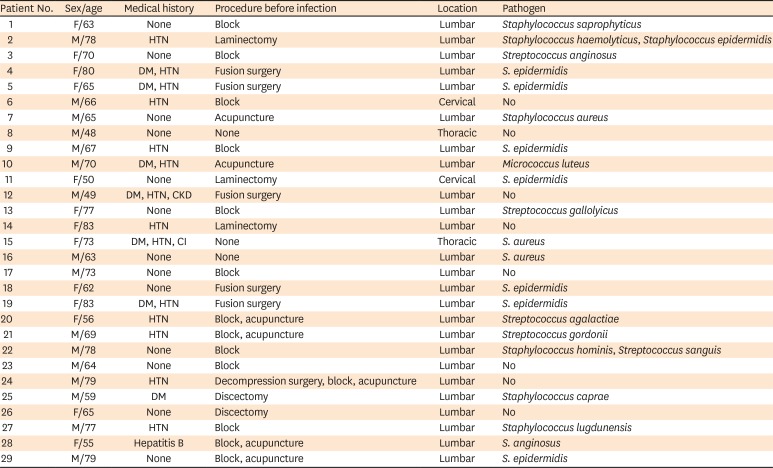
TABLE 1
Demographical and infection characteristics of patients
DM: diabetes melitus, HTN: hypertension, CKD: chronic kidney disease, CI: cerebral infarction, M: male, F: female.
![]()
Regarding the procedures performed on patients before the bacterial spinal infection, 14 received nerve block, 7 had acupuncture, 6 had laminectomy and discectomy, 5 had fusion surgery, and 2 underwent no prior procedure.
Blood culture was conducted for all 29 patients, and bacteria were identified from the blood in 7 patients. Seventeen patients received bone biopsy, and bacteria were identified in 16 of them. Revision surgery was performed in 6 patients, and bacteria were identified in all of them. Staphylococcus epidermidis was the most common bacteria, identified in 8 patients. Staphylococcus aureus was the second most common bacteria, which was found in 3 patients. No bacteria were identified in 8 patients; therefore, they were treated with empirical antibiotic therapy.
The mean ESR, CRP, PCT, and WBCs decreased at week 4 of antibiotic treatment compared to their baseline values (FIGURE 1). However, ESR was found to increase at weeks 2 and 3 when graphed. PCT notably decreased after the initiation of antibiotic treatment, but changes found thereafter in weeks 1–4 were unremarkable. In contrast, CRP and WBCs were gradually decreased until 4 weeks compared to before treatment. Statistically, CRP and WBCs were significantly decreased after 4 weeks of treatment compared to before treatment. The mean ESR and PCT was not statistically significant compared to pretreatment and after antibiotic treatment (p-value>0.05).
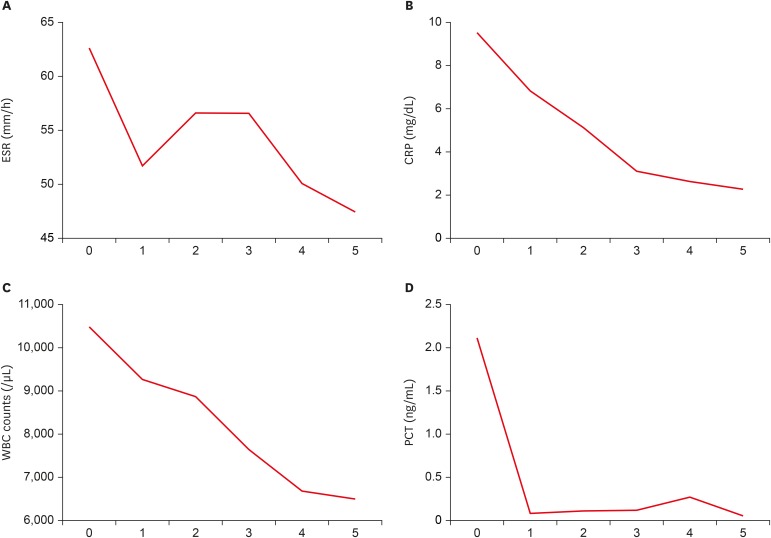 | FIGURE 1Changes of biomarker over time before and after antibiotic treatment. (A) ESR, (B) CRP, (C) WBC counts, and (D) PCT. The basal value of CRP and WBC counts before antibiotics treatment were compared with those of each week, and statistical significance was noted (p-value<0.05). 0, Before antibiotic treatment; 1, 3 days after antibiotic treatment; 2, 1 weeks after antibiotic treatment; 3, 2 weeks after antibiotic treatment; 4, 3 weeks after antibiotic treatment; 5, 4 weeks after antibiotic treatment.ESR: erythrocyte sedimentation rate, CRP: C-reactive protein, WBC: white blood cell, PCT: procalcitonin.
|
Go to :
DISCUSSION
Spinal infection refers to microbiological infection in the vertebral body, intervertebral discs, or paravertebral tissues caused by medical reasons, such as the procedure or surgery.1316) Spinal infection accounts for 2–7% of all musculoskeletal infections,16) and post-spinal surgery incidence of 0.7–12% is reported in adults.619) Despite the development of new antibiotics and progress made in surgical methods, the incidence has been on an increasing trend owing to increases in spinal surgery and procedure.12)
ESR, CRP, and WBCs are important markers used to diagnose and evaluate treatment responses in infectious conditions in humans.121316) ESR is a nonspecific test used for various conditions, such as inflammation, trauma, and cancer. Although ESR has a low specificity for diseases, it is used to diagnose and follow up various cases, including infection, inflammatory diseases, malignant tumor, and trauma. Due to its non-specificity, ESR is used to evaluate the activity of a given disease or monitor its progression, rather than its diagnosis.41618) CRP increases in response to pneumococcal infection, stress, trauma, infection, inflammation, postoperative changes, and tumor, and has a higher sensitivity compared to other acute-phase reactive proteins.416) PCT is a peptide consisting of 116 amino acids and is produced by parafollicular cells of the thyroid gland.5920) PCT is a more specific marker for bacterial infections because PCT production is attenuated by interferon gamma in viral infections.20) Serum PCT concentration is <0.05 µg/dL in healthy adults and increases in the context of bacterial infections, with correlation between the magnitude of increase and infection severity.20) PCT becomes detectable 3–4 hours after the onset of infection and peaks 6–12 hours after the onset, and its half-life is approximately 24 hours.920) Since PCT increases early in bacterial infection and decreases rapidly after antibiotic treatment, PCT is reported to be higher than the CRP in early diagnosis and monitoring of infectious dieseases.1220)
However, reports on the usefulness of PCT in spinal infection have been limited. Chung et al.5) reported that the measurement of serum PCT is useful in post-spinal surgery fever of unknown origin. Jeong et al.12) reported that serum PCT is less sensitive than CRP in spinal infection and that other infections than spinal infection should be confirmed when the serum PCT increases in order to provide appropriate antibiotic treatment.123101114) Maus et al.17) reported that PCT is a biomarker that is unsuitable for diagnosis and monitoring of spinal infection. Yoon et al.24) reported that there were statistically significant differences between WBCs and CRP in tuberculous spondylitis versus pyogenic spondylitis but PCT was not statistically different between the 2 groups.
The utility of CRP and PCT help to reflect the severity of infection and determine the suitability of the antibiotics for infection control.1237102122) Among the biomarkers that are measured in patients with infections, ESR, CRP, and WBCs have been used for a long time in clinical settings although they are not sensitive for bacterial infection.41216) Increases in biomarkers are sometimes observed even during antibiotic treatment, casting doubts on the therapeutic efficacy. In our study, changes of PCT was greatest among the 4 biomarkers after 1 week of antibiotic use. This was not statistically significant, but it can be indirectly estimated that the initially determined antibiotic was effective. As well as in this study, elevated ESR, a declining trend in CRP, WBCs and normal PCT level at 3 weeks of antibiotic treatment may be assumed to have no worsening of infection or an antibiotic effect. Since several factors other than bacterial infection can influence the increase in ESR and WBCs values, biomarkers that sensitively change in response to the onset, improvement, or exacerbation of bacterial infections should be identified. CRP and PCT are thought to be a marker that responds sensitively to bacterial infection and can be known as a good biomarker that can evaluate exacerbation of infection even in cases where unexplained increase in ESR is observed.
Moreover, changes in each biomarker may differ between patients treated with antibiotics with bacteria found in their blood culture, bone biopsy, and revision surgery and patients treated with empirical antibiotic therapy without bacterial identification. In such cases, the clinical usefulness of PCT should be re-evaluated.
Go to :
CONCLUSION
The effect of antibiotics on pyogenic spondylitis cannot be compared with only one biomarker, and it is necessary to observe the changes of various biomarkers. Among several biomarker, CRP and WBCs are biomarkers that can aid early evaluation of the effects of antibiotic treatment in pyogenic spondylitis. Although PCT did not have statistical significance, it can be used as a biomarker that reflects the effect of antibiotic and severity of infection.
Go to :
 XML Download
XML Download