

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Spontaneous intracerebral hemorrhage (ICH) is caused by the rupture of small blood vessels in the brain. It is a major health problem with an annual incidence of 10–30 per 100,000 individuals and accounts for 8–30% of total strokes.23) Compared with ischemic stroke, ICH is a critical disease with 2–6 times higher mortality and morbidity.12) According to reports, the 30-day mortality rate of ICH is 30–55% and only 12–39% of survivors have favorable functional outcomes after 6 months.1924)
In patients with ICH, hematoma enlargement is the most critical risk factor that causes poor outcomes and increasing mortality.15) Therefore, prevention of hematoma enlargement is the goal of conservative management. However, except strict control of blood pressure (BP), it is not know how to prevent hematoma enlargement in ICH patients.1518)
According to several articles, the use of anti-fibrinolytic agents has been reported to reduce blood loss during surgery and prevent hematoma expansion.18112732) However, unlike these promising findings, some related randomized controlled trial have shown that antifibrinolytic agents do not affect rebleeding, neurologic deterioration, and mortality for cerebral hemorrhage.2529) In consideration of these discrepancies, we analyzed the risk factors for hematoma expansion in ICH patients and compared the predictability of hematoma expansion in ICH patients with the use of an anti-fibrinolytic agent.
Go to : 
MATERIALS AND METHODS
Patient papulation and hematoma measurement
We assessed 489 patients who were diagnosed with spontaneous ICH from October 2008 to October 2018. We excluded 62 patients with symptoms that developed after 24 hours. We also excluded 25 patients who refused treatment because of old age, chronic diseases, or personal issues, and 62 patients who underwent surgery after the first computed tomography (CT) scan. Eleven patients who did not undergo follow-up CT within 48 hours were excluded. Therefore, 329 who were treated appropriately with conservative management, including strict BP control and pain control, were included in the study. This study was approved by Institutional Review Board of Pusan National University Yangsan Hospital (IRB No. 05-2019-111).
All patients with neurological symptoms were routinely evaluated by neurosurgeons and admitted to our neurointensive care unit or neurosurgical unit. This series of patients did not include those with hemorrhage due to intracranial aneurysms, arteriovenous malformation, arteriovenous fistula, cavernous malformation, moyamoya disease, or tumor bleeding. Most of these diseases could be excluded by taking CT angiography or enhanced CT at the same time during their first CT. When tumor bleeding was suspected, the patient's cancer history was confirmed and magnetic resonance images (MRI) were taken after 2 to 4 weeks. Cavernous malformation was excluded via MRI after the hematoma was absorbed.
The first CT was taken within 30 minutes of arrival to the emergency room, the second CT was taken within 48 hours, and the CT was taken early if there were any changes in neurological symptoms or the Glasgow coma scale score. Hematoma size was measured in the initial and second CT images. The maximal diameter was the longest measured intraparenchymal high density among the CT axial sections. The final lesion volume was calculated by multiplying the area obtained in each section by the slice thickness. Ventricular hemorrhage was excluded in the hematoma volume calculation because of calculation difficulties. Various definition for hematoma expansion has reported to be an increase in the hematoma volume of 20% to 50% from the baseline image to the second CT scan.51316) We defined hematoma expansion as an increase of more than 20% of the maximum diameter or increase of more than 20% in volume.
Since February 2017, we have used antifibrinolytic agents in combination with BP and pain control medications in patients with ICH. When ICH was diagnosed via CT scan, patients immediately received 2 g of tranexamic acid (Transamin-S Injection, an intravenous bolus of 2 g, over a period of 10 minutes). The use of this dose was based on Sorimachi's report,27) which is the well-known study of tranexamic acid-based ICH hemostasis. Therefore, patients who did not receive tranexamic acid from October 2008 to January 2017 were compared with patients who were administered tranexamic acid.
The target systolic BP was lower than 140 mmHg. This value was determined according to several ICH guidelines.3141530) BP was monitored continuously through the arterial line. Initial high BP was controlled by a diltiazem or nicardipine bolus intravenous injection, and to maintain systolic BP under 140 mmHg, continuous intravenous administration of nicardipine was used in the neurosurgical intensive care unit during the first 48 hours after admission. For better BP control, we made great efforts to reduce pain by using non-steroidal anti-inflammatory drugs and various analgesics (e.g., narcotic or patch type analgesics). The visual analog scale was utilized to quantify pain. Analgesics were used when the patient complained of pain, including headache. In unconscious patients, analgesics were used when BP was controlled but not controlled.
Data collection
We collected well-known risk factors for hematoma expansion from patients' data by using electric medical records and the PACS system: patient's age and sex, location of hematoma, level of consciousness, systolic BP at admission, medical history (e.g., hypertension, diabetes, dyslipidemia, cardiovascular disease and chronic kidney disease [CKD]), alcohol consumption, smoking status, use of an antiplatelet agent, use of anticoagulants, and hematoma volumes.
Statistical analysis
All statistical analyses were performed using SPSS statistics (version 22.0; IBM Corporation, Armonk, NY, USA). Continuous variables are presents as means±standard deviations. Categorical variables are presented as numbers and percentages. Student's t-test, χ2 analysis, and the Fisher's exact test were used to assess between-group differences. Receiver operating characteristic (ROC) curves were created to determine the optimal hematoma volume and maximal diameter cut points, sensitivity, and specificity in hematoma expansion according to the second CT. Univariate and multivariate logistic regression analyses were used to assess risk factors for hematoma expansion. Multivariate logistic regressions were performed with independent variables selected from all factors with a value of p<0.1 in univariate analyses. The results are presented as odds ratios with a 95% confidence interval (CI). Statistical significance was set at p<0.05.
Go to :
RESULTS
Tranexamic acid was applied according to the protocol in 67 of 329 patients. TABLE 1 shows the characteristics of patients who did and did not receive tranexamic acid. There was no statistically significant difference between the 2 groups in mean age, sex, size and volume of hematoma, spot signs on hematomas, BP, medical history (hypertension, diabetes mellitus, dyslipidemia, cardiovascular disease, stroke, alcohol), and drug use (antiplatelet or anticoagulant), except smoking status and CKD.
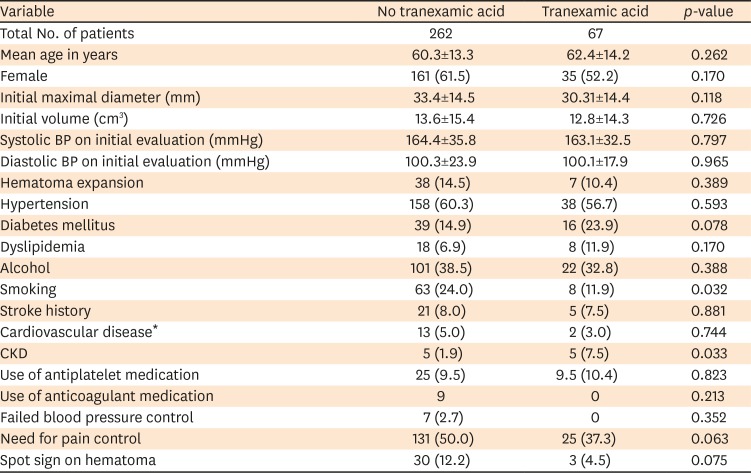
TABLE 1
Clinical characteristics of patients with and without tranexamic acid
Values represent the number and percentage of patients or, where otherwise indicated, the means±standard deviations.
BP: blood pressure, CKD: chronic kidney disease.
*Cardiovascular disease is a myocardial infarction, angina or coronary artery disease.
![]()
Although there was no significant difference in the characteristics of the patients between the 2 groups, the use of tranexamic acid did not show a significant reduced incidence of hematoma expansion. Hematoma expansion was observed in 7 patients (10.4%) in the tranexamic acid group and 38 patients (14.5%) in the control group.
We further analyzed risk factors involved in hematoma expansion. TABLE 2 compares the 2 groups who experienced hematoma expansion. There was a significant difference in the maximal diameter of the hematomas and the presence of spot sign between the 2 groups. Although there was no statistical significance, there seemed to be an association of initial hematoma volume, smoking, and need for pain control with a hematoma expansion. Therefore, a multivariate logistic regression analysis was performed to determine the risk factors of hematoma expansion including these variables. TABLE 3 shows the results. The maximal diameter of the hematoma and the presence of spot sign were found as significant risk factors for hematoma expansion.
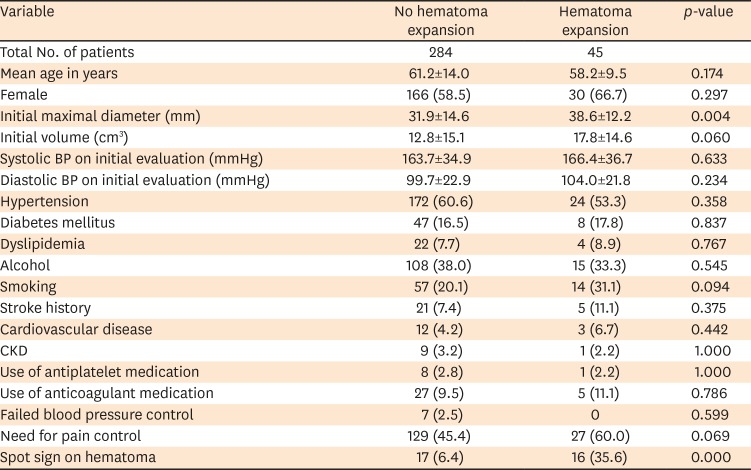

TABLE 2
Clinical characteristics of patients with and without hematoma expansion
Values represent the number and percentage of patients or, where otherwise indicated, the means±standard deviations.
BP: blood pressure, CKD: chronic kidney disease.
![]()
TABLE 3
Multivariate logistic regression analysis of risk factors of hematoma expansion
Multivariate logistic regressions were performed with independent variables selected form all factors (Table 2) with a value of p<0.1 in univariate analysis.
OR: odd ratio, CI: confidence interval.
![]()
Hematoma volume and maximal diameter were 17.8±14.6 cm3, 38.6±12.2 mm in the hematoma expansion group and 31.9±14.6 mm, 12.8±15.1 cm3 in the non-hematoma expansion group, respectively. Based on the ROC curve, the optimal cut points to achieve the maximal sensitivity and specificity of the maximal diameter and hematoma volume were 40.5 mm and 10.1 cm3, respectively. TABLE 4 provides the optimal cut-off value and area under the ROC curve (95% CI). As the area under the ROC curve is 0.635, the cutoff value of 10.1 cm3 for the hematoma volume demonstrated poor discriminatory ability for hematoma expansion.20)

TABLE 4
Association between hematoma expansion and hematoma volume, maximal diameter
| Factor | AUC | Sensitivity (%) | Specificity (%) | Optimal cutoff value | Discrimination |
|---|---|---|---|---|---|
| Maximal diameter | 0.851 (0.798, 0.903) | 75.6 | 75.4 | 40.5 | Good |
| Hematoma volume | 0.635 (0.553, 0.718) | 60.0 | 60.9 | 10.1 | Poor |
ROC: receiver operative characteristic, AUC: area under the receiver operative characteristic curve.
![]()
Of the 45 patients with hematoma expansion, 17 patients underwent conservative management, 17 patients received hematoma aspiration, and 11 patients received craniotomy and ICH removal.
Go to :
DISCUSSION
Tranexamic acid
Tranexamic acid is a synthetic derivation of the amino acid lysine. It serves as an antifibrinolytic by reversibly binding to 4 or 5 lysine receptor sites on plasminogen molecules. This binding completely blocks the interaction of plasminogen and plasmin with lysine residues on the surface of fibrin, thereby preventing proteolytic action of plasmin on fibrin and inhibiting fibrinolysis at the bleeding site.10) With this mechanism, tranexamic acid has been used for decades in multiple surgical disciplines for its ability to reduce intraoperative blood loss and the need for blood transfusions.17) Evidence suggests that tranexamic acid may also reduce postoperative edema and ecchymosis.21)
Tranexamic acid also passes through the blood-brain barrier and may be effective in hemorrhage diseases, including intracranial hemorrhages.29) In light of these concepts, some researchers have reported that tranexamic acid reduces rebleeding in aneurysmal subarachnoid hemorrhages (SAH); although it has been reported that thromboembolic events or delayed cerebral ischemia also increases.821) In addition, recent systemic reviews have reported that the use of tranexamic acid in patients with nontraumatic SAH reduces mortality; however, this finding was not statistically significant.2) In another intracranial hemorrhage study, Sorimachi et al.26) reported that the combination of rapid administration of tranexamic acid and strict BP control may prevent hematoma growth in patients with ICH.22) To the best of our knowledge, there is no evidence to show the effect of tranexamic acid in ICH aside from this study. Recently, several well-designed clinical trials, including those evaluating TICH-2, have been planned and conducted, but they have not shown statistically satisfactory results including reduce hematoma expansion and clinical outcomes.2233) Therefore, our study investigated the effect of tranexamic acid on ICH in a way similar to Sorimachi's study.27) Our results showed that there was no statistical significance in ICH patients with rapid administration of tranexamic acid and strict conservative management, but the rate of patients who experienced hematoma expansion was reduced (14.5% vs. 10.7%).
The use of tranexamic acid in cardiac, orthopedic, and spinal deformity surgeries has shown reduced hemorrhage and intraoperative transfusion. However, in the above-mentioned surgeries, hemorrhage occurs mainly in muscle and connective tissues, but most ICHs occur in small blood vessels. Therefore, a direct comparison is not appropriate.
The safety of tranexamic acid is also controversial. The primary issue with the use of tranexamic acid is the potential for an increased risk of thromboembolic events, such as myocardial infarction, ischemic stroke, deep vein thrombosis, and pulmonary embolism.631) However recent literatures, including a meta-analysis, demonstrated that tranexamic acid was not associated with an increased incidence of thromboembolic events.31) In addition to these complication, tranexamic acid has complications such as nausea, vomiting and abdominal pain, but it had been difficult to evaluate in our patients. The present study showed a limited observation duration and number of cases, but we did not observe such complications.
Risk factors of hematoma expansion
Our study showed that the maximal diameter of hematomas and the presence of spot sign are risk factors for hematoma expansion. These variables are risk factors for well-known hematoma expansion. Our study suggests that if the maximal diameter of the hematoma is greater than 40 mm, it should be closely monitored because of the possibility of hematoma expansion. Other previous studies identified hematoma volume as a predictor of hematoma expansion,49) however our study failed to concur, possibly because researchers did not directly calculate volume according to the CT slice thickness. In contrast, maximal diameter of hematoma could be predicted by hematoma expansion because this was easily measured and accurate.
Spot sign has been studied extensively in the last decade and might be the strongest individual predictor for subsequent hematoma expansion. One believable explanation is that spot sign might represent active bleeding or rebleeding in ruptured vessels, which reflects contrast extravasation on CT or MRI scans.7) Recently, modified spot sign and black hole sign on non-enhance CT scans have been proposed as radiologic markers similar to spot sign, and these markers are also strongly associated with hematoma expansion and prognosis.28)
Other parameters including anticoagulant and antiplatelet medication did not indicate statistical significance. These results suggest that we had a small number of cases and those adjustable parameters, including BP and pain, were strictly managed according to the guidelines.
Our study has several limitations including the retrospective nature of data collection and small population. The results of well-designed and randomized, controlled ongoing clinical trials will prove the value of our findings.
Go to :
CONCLUSION
In this retrospective study, there was no statistical significance between patients who experienced ICH with rapid administration of tranexamic acid and those with strict conservative management, but the rate of patients who experienced hematoma expansion was reduced. We also found the importance of the spot sign in the risk factor analysis and hematomas size greater than 40 mm, should be closely monitored because of the possibility of hematoma expansion.
Go to :
 XML Download
XML Download