

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic subdural hematoma is common in the elderly, with a rate of 1–2 per 100,000 population at age 60 and 7.4 at age 70.4) About 80% of patients have head trauma, and most have mild trauma. Treatment consists of pharmacologic therapy and surgical therapy. Pharmacologic therapy includes steroid administration, and anticonvulsant drugs, hyperosmolar solutions such as mannitol, and hyperosmolar treatment, and diuretic can cause water and electrolyte imbalance.
Surgical treatment includes craniotomy, trephination, burr hole drainage, twist drill perforation.131617) The recurrence rate of chronic subdural hematoma was 3.0–37.0%.67) The recurrence risk factors were age, brain atrophy, large hematoma, septum formation in subdural hematoma, alcohol, anticoagulant, renal failure, malignant tumors, and metastasis in the dura mater.1213) It is known that there is a high-risk of recurrence that has accumulated air in hematoma space.1718) In this study, we analyzed the recurrence rate and number of hospitalization days of patients with chronic subdural hematoma in both of burr hole drainage group and small craniotomy group.
MATERIALS AND METHODS
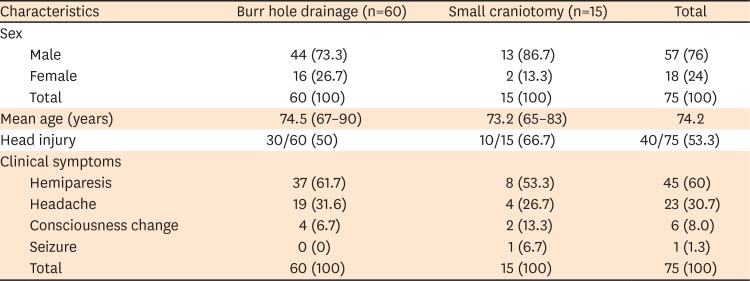
Seventy-five patients who underwent surgery with chronic subdural hematoma in our hospital from January 2016 to December 2018. Patients with risk factors of recurrence such as previous history of ventriculoperitoneal shunt placement, hepatic failure, renal insufficiency, or anticoagulant therapy15) were excluded. As retrospective chart review study, it was granted by the Institutional Review Board of Inje University Busan Paik Hospital. Sixty patients were diagnosed to chronic subdural hematoma with homogeneous and low density on computed tomography (CT) images that was considered liquefied hematoma (FIGURE 1A) and underwent one burr hole drainage (FIGURE 1B & C), and 15 patients with heterogenous or high density on CT images that was considered solid or mixed form hematoma (FIGURE 2A) performed small craniotomy at frontal or parietal area and was done hematoma removal and saline irrigation (FIGURE 2B & C). Drainage catheter was inserted into the subdural hematoma space in both burr hole drainage (FIGURE 1C) and small craniotomy group (FIGURE 2C). The surgical method was determined according to the pattern of hematoma on brain CT images. The recurrence rate and length of hospitalization days were compared between the patients with burr hole drainage and small craniotomy. Statistical analysis was performed using t-test and p-value <0.05 was interpreted to have statistically significance. In 75 patients, male to female ratio was 57:18 and mean age was 74.2 years old (range, 65–90 years old). The incidence of chronic subdural hematoma was higher in male patients. Forty patients (53.3%) had head trauma history, and 35 patients (36.7%) had no history of head trauma. The symptoms that presented when visited in hospital were hemiparesis in 45 patients (60%), headache without other neurologic symptoms in 23 patients (30.7%), and mental deterioration in 6 patients (8.0%), seizure in 1 patient (1.3%) (TABLE 1). Location of subdural hematoma was left frontotemporoparietal area in 36 patients (48.0%), right frontotemporoparietal area in 22 patients (29.3%), and both frontotemporoparietal area in 12 patients (16.0%), right parietal area in 3 patients (6.0%) and left parietal area in 2 patients (2.6%) (TABLE 2).
FIGURE 1
(A) Pre-operative computed tomography showed isodensity crescentic shaped hematoma in left frontotemporoparietal area. (B, C) Seventy-one-year-male patient with chronic subdural hematoma underwent burr hole drainage in left parietal area.

FIGURE 2
(A) Pre-operative computed tomography showed heterogenous, crescentic shaped hematoma in left frontotemporoparietal area. (B, C) Seventy-six-year-male patient with chronic subdural hematoma underwent small craniotomy with drainage in left parietal area.

TABLE 1
Characteristics and clinical findings of patients

RESULTS
Sixty patients underwent burr hole drainage and 15 patients were performed small craniotomy. Of the 60 patients were performed with burr hole drainage, 8 patients (13.3%) were recurred and were operated again. Among the 15 patients were performed small craniotomy, 7 patients (46.7%) were recurred and underwent 2nd operation.
Average number of hospitalization days were 10.3 days (range, 6–29 days) in burr hole drainage group, and 15.7 days (range, 8–42 days) in small craniotomy group (TABLE 3).
TABLE 3
Post-operative recurrence rate and mean hospitalization days

| Characteristics | Burr hole (n=60) | Craniotomy (n=15) | p-value |
|---|---|---|---|
| Recurrence (%) | 8 (13.3) | 7 (46.7) | 0.03* |
| Mean hospitalized days | 10.3 (6–29) | 15.7 (8–42) | 0.03* |
There were no complications such as acute bleeding, infection, or neurological deficit related to surgery in both groups.
DISCUSSION
Chronic subdural hematoma is a common disease in neurosurgery. It is generally known to occur in the elderly population, and is reported to be the highest incidence in the 60s and 70s. In addition, as the age increases, the incidence is increased sharply. In the 70s, there are 7.35 cases per 100,000 population, and the incidence of chronic subdural hematoma is likely to increase due to the increase in the elderly population.2) Chronic subdural hematoma is known to be caused by various causes such as trauma, alcohol and anticoagulant administration, hemorrhagic disease.22) 60 to 80% occur after head trauma. Head trauma is often mild and patients may not be aware of it.20) In this study, 46.7% of patients denied head trauma.
The formation and growth mechanism of chronic subdural hematoma has not been fully elucidated yet.215) The most common reason for elderly people affected well is physiological brain atrophy, which enlarges the space between the brain cortex and the dura mater, so tension of bridging vein increases and venous congestion occurs in the cerebral cortical vein, and dura mater is detached from the arachnoid membrane, that subdural hematoma occurs due to rupture or leakage of bridging vein, and patient is older, hemostatic function is decreased so hematoma can develop and grow easily.1230)
Symptoms of chronic subdural hematoma include hemiparesis, headache, loss of consciousness, and seizures, and presented symptoms was reported hemiparesis in 58%, headache in 14–80%, seizures in less than 6%, and unconsciousness in 36%.227) The incidence of symptoms was similar in our study.
The treatment of chronic subdural hematoma is variable from pharmacologic therapy to operative therapy. However, most patients are operated if the patient is not inoperable condition or a small amount of hematoma with no symptom.922) In chronic subdural hematoma, burr hole drainage is the most commonly used operative method. The overall morbidity rate is reported 0–2% and recurrence rate is 5–30%. Burr hole drainage is known to be the most effective method for treatment of chronic subdural hematoma with less complication.92123) On the other hand, if repeated recurrences, solid hematomas or septum in subdural hematoma are present, a small craniotomy can be performed.32) Especially, when presents multiple compartmentalized lesions in subdural hematoma, burr hole drainage may result in incomplete drainage, and acute hemorrhage may be occurred due to injury of the cortical vein during insertion of the drainage catheter, so these cases, small craniotomy should be performed.132425)
Santarius et al.5) compared burr-hole evacuation with drains group versus no drains after burr-hole evacuation. The recurrence rate was lower in the drain group than in the no drain group. And at discharge of the hospital, neurological status was better and the mortality rate was lower at 6 months in drain group. So, burr hole drainage has been accepted as a general treatment strategy of chronic subdural hematoma, recently. Okada et al.31) reported that to avoid infection, drainage for 2 days appears to be sufficient. So, in our study, the draining catheter was inserted subdural space in all patients who performed burr hole drainage and was removed 2 days after the operation.
In our study, 60 patients were performed burr hole drainage with irrigation. Zakaraia et al.19) and Gurelik et al.10) reported no difference in clinical efficacy and recurrence rate between the irrigation and non-irrigation groups. However, some studies reported a higher recurrence rate in the irrigation group. Okada et al.31) compared the patients who were performed burr hole drainage and burr hole irrigation in terms of recurrence and hospitalization. In patients who were treated with burr hole irrigation was revealed higher recurrence rate and longer hospitalization. The intracranial pressure is decreased due to irrigation, and the inflation of air into the subdural space can interfere the brain expansion. In the drainage group, there is a relatively low-risk of recurrence, because the intracranial pressure is relatively slowly changed and the bridging vein is less damaged.262933) In addition, there is also a report that rapid changes in the intracranial pressure may lead to complications such as epilepsy, cerebral edema, and cerebral hemorrhage in irrigation group.1134)
Mondorf et al.27) conducted a retrospective study about treatment effect and recurrence of 193 patients with chronic subdural hematoma. Craniotomy were performed in 151 patients and burr hole drainage were performed in 42 patients. In that study, recurrence was developed in 27.8% of patients who underwent craniotomy and 14.3% in patients who underwent burr hole drainage. The complete neurologic recovery at the discharge was 52.3% in patients with craniotomy and 64.3% in patients with burr hole drainage. In that study, burr hole drainage was reported to be better in terms of recurrence rate and recovery of symptoms than craniotomy. In our study, recurrence rate is 26.7% in small craniotomy group, and 13.3% in burr hole drainage group. And average number of hospitalization days were 10.3 days in burr hole drainage group and 15.7 days in small craniotomy group. Patients who underwent burr hole drainage showed a lower recurrence rate and shorter hospitalization days than patients who underwent small craniotomy. We performed burr hole drainage in chronic subdural hematoma that showed homogenous and low-density CT images, and performed small craniotomy in patients with chronic subdural hematoma that revealed septum formation, and heterogenous or high density on CT images. The risk factor of recurrence of chronic subdural hematoma was reported with large amounts of hematoma, bilateral hematoma formation, present of septum in hematoma on CT images.814222829) Ko et al.15) also reported that heterogenous and high density in subdural hematoma on CT scan indicate a risk of recurrence. Because of these preconditions, the recurrence rate is considered to be higher in small craniotomy group in our study.
CONCLUSION
In patients with chronic subdural hematoma, burr hole drainage is considered safe and effective treatment method because of lower recurrence rate and short hospitalization days than small craniotomy. But if complete drainage may be difficult when performing burr hole drainage, in selective cases like that subdural hematoma has solid portion or multiple septum in CT findings, small craniotomy could be considered although small craniotomy has higher recurrence rate and longer hospitalization days than burr hole drainage in overall cases.
 XML Download
XML Download