

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The subdural hematoma occurs with a probability of 5–29% of all head trauma patients, and this is largely due to rupture of cerebral cortical artery or vein, or rupture of bridging vein between cerebral cortex and dura mater.27819) Most cases occur with trauma, but anticoagulation medication or blood dyscrasia may cause hematoma without trauma.10161719) The acute subdural hematoma (ASDH) can be observed without operation if the neurologic deficits are mild or the amount of hematoma is small. However immediate operation is necessary if patients show poor mental state, worsening of neurologic signs, or a large amount of hematoma. The principle surgical method of ASDH is a craniotomy or craniectomy with hematoma removal, but there may be complications from general anesthesia and the procedure itself. The aged patients and in cases of bleeding tendency such as medication of antithrombotics and chronic alcoholism, the craniotomy may also have a risk potential of hemorrhage. Hence, we operated primarily those cases with burr hole drainage under local anesthesia after 1–2 weeks waiting. The coagulated hematoma requires those durations for a liquefaction and become subacute subdural hematoma. The trephination with drainage is often difficult to remove hematoma completely. So, we instilled urokinase (UK) into the subdural space and adjusted the dosage according to the amount of remnant hematoma and computed tomography (CT) findings. This approach may be particularly valuable for patients who present with comorbidities or can't endure highly invasive surgical procedures. We report the results of trephine drainage of ASDH in subacute stage with UK instillation to hematoma in limited cases.
Go to : 
MATERIALS AND METHODS
Between January 2016 and December 2018, delayed operations of ASDH in subacute stage using UK were performed in 9 patients. Those patients are the cases of ASDH that clinical symptoms and signs were not significant enough to be treated conservatively at the time of admission. We selected the patients who had good mentality regardless of age and head injury, including those who were expected to have complications such as hemorrhage due to antithrombotic medications (antiplatelets, anticoagulants). During conservative treatment, we decide to perform operation in the following situations: 1) worsening of neurologic conditions (mental deepening, development of hemiparesis or severe headache), 2) aggravation of midline shifting and/or change of high-density hematoma into low-density in serial CT scans regardless of clinical status. If clinical symptoms improved, or the mass effect decreased on CT scans after initial trephine drainage, UK instillation was not done at that moment. And those cases were excluded in this study.
All cases were ASDH except one concurrent with a small frontal intracerebral hematoma. The patient who had ASDH and intracerebral hematoma was 90 years old and decrepit, so we performed trephine surgery instead of craniotomy (case 7). And 4 patients were operated because of aggravation of midline shifting on serial CT findings although Glasgow Coma Scale (GCS) score was 15. The other 4 patients whose GCS score were deteriorated to 14 and accompanied by midline shifting were underwent operation.
After local anesthesia with 1% lidocaine, the scalp incision and trephination was performed at the lesion site. After incision of dura mater, we confirmed the hematoma from the subdural space and inserted a 12.5 French double-lumen catheter to a depth of about 5 cm. The double-lumen catheter has a small another lumen attached to main catheter which is designed for drug injection. After the operation, we waited until the drainage of the liquefied hematoma cease, and the CT scans were rechecked for the evaluation of remnant hematoma. When the high density hematoma remained, UK was instilled. The mixture of 5 mL of normal saline and UK dried powder (20,000 IU) was used. The time interval from initial operation to injection of UK was 1 to 4 days. UK injection was done once or twice a day according to CT findings and it lasted up to 4 days. The clamping time of catheter after injection of UK was 8–12 hours, after then liquefied hematoma was not aspirated but drained. The timing of catheter removal was variable depending on the amount of remaining hematoma seen on the CT scans. We stopped antithrombotic medication during admission and restarted after discharge. Although discontinuation of these drugs may adversely affect patients with cerebral infarction or heart disease, but we thought that treatment of ASDH was more important at that situation.
We analyzed the following clinical information (TABLE 1): clinical symptoms, trauma and medical history, antithrombotic medication, amount of UK instillation. The patient conditions were evaluated using the GCS and assessed immediately before surgery. The outcomes were evaluated by the Glasgow Outcome Scale (GOS) at discharge.
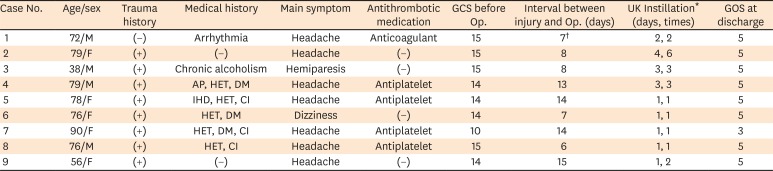
TABLE 1
Summary of clinical features of 9 operated cases
AP: angina pectoris, CI: cerebral infarction, DM: diabetes mellitus, GCS: Glasgow Coma Scale, GOS: Glasgow Outcome Scale, HET: hypertension, IHD: ischemic heart disease, Op.: operation, UK: urokinase.
*It means duration of UK treatment and total times of UK instillation. One dosage is a mixture of 5 mL normal saline and UK dried powder (20,000 IU); †Interval between onset of symptom and operation.
![]()
Go to :
RESULTS
The mean age of patients was 71.6 years (range, 38–90 years). Of which, 4 was the male patients while the rest of 5 was female. Eight patients had trauma history but one does not (case 1). He had a cardiac arrhythmia and was taking warfarin, and the laboratory finding of prothrombin time international normalized ratio was prolonged (2.59) at admission. We estimated that the cause of ASDH was coagulopathy. The medical history was as follows: hypertension in 5 patients, diabetes mellitus in 3, cerebral infarction in 3, cardiac disease in 3 and chronic alcoholism in 1. The main clinical feature at admission was headache in 7 patients, dizziness and hemiparesis in one each. Four patients were taking the antiplatelet and one patient the anticoagulant at the time of admission. The hematoma was located unilaterally in all cases. The laboratory findings of all patients except one were normal for prothrombin time, partial thromboplastin time and platelet counts in peripheral blood. The interval from trauma to surgery was from 6 to 15 days (mean, 10.2 days). During the treatment period, UK was the least injected once, and the most injected was 6 times during 4 days. The total duration of catheterization was from 3 to 7 days (mean, 4.6 days). The preoperative GCS was 14 or 15 in all cases except one. The oldest patient had a small frontal intracerebral hematoma, whose GCS was 13 at admission and deteriorated to 10 preoperatively (case 7). The GOS score was 5 in 8 patients at discharge, and 3 in one who had an intracerebral hematoma. During the admission there were no complications like infection and/or recurrent hemorrhage. And UK related bleeding in other organs was not found.
Illustrative case (Case 3)
A 38 years old male patient was admitted with a left hemiparesis after he drank and slipped the day before. His mental state was mild drowsy (GCS 14) and accompanied by mild dysarthria. The initial CT scan showed an ASDH in the right frontotemporoparietal lobe without midline shifting (FIGURE 1A). He was a chronic alcoholic without systemic disease in his medical history. No abnormalities were found on the laboratory findings. The GCS had become 15 and the hemiparesis was recovered slowly on the day of admission. He was treated conservatively because of good mental status and no neurologic deficit. On the 7th day of hospitalization, the patient developed symptoms of increased intracranial pressure, including left hemiparesis and deepening of mental status (GCS 14). The follow-up CT scan showed increase of a mixed density subdural hematoma and severe midline shifting toward the left about 13 mm (FIGURE 1B). A subdural drainage after trephination was performed under local anesthesia, and dark liquefied hematoma was drained about 160 mL. When the flow of draining hematoma stopped 2 days after operation, we checked the serial follow-up CT scan for confirming of clotted hematoma and injected UK daily into the subdural space. Total amount of drained hematoma was about 520 mL during 3 days, which was result of UK (20,000 IU) instillation daily for 3 days. A CT scan 6 days after trephination, represented marked decrease of the subdural hematoma and resolution of the mass effect (FIGURE 1C). The catheter was removed 6 days after operation and the GOS score was 5 at discharge. No recurrence of the hematoma was found on CT scan taken 1 month after operation (FIGURE 1D).
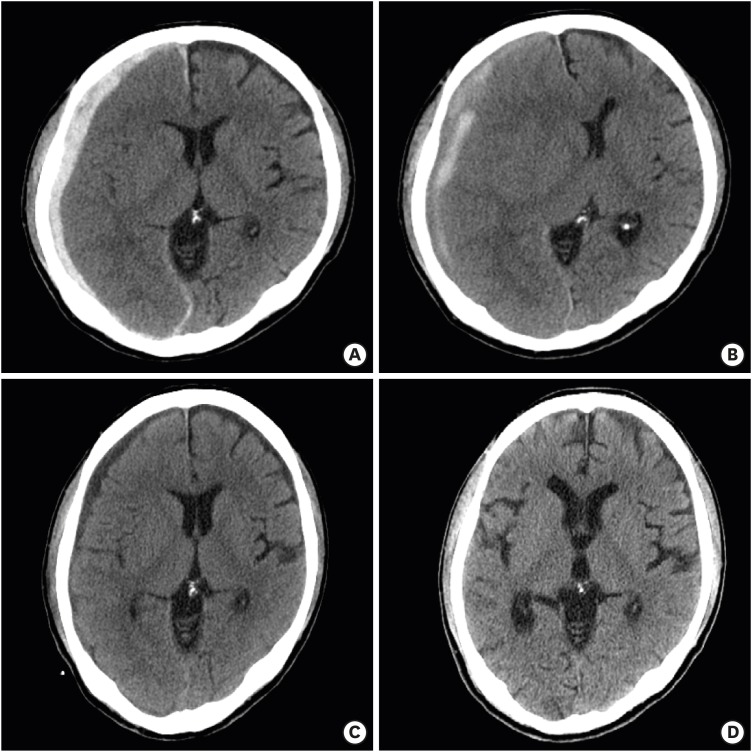 | FIGURE 1A 38-year-old male patient was admitted with headache after a slip down. (A) At admission, a CT scan showed a hyperdense subdural hematoma (SDH) at right frontotemporoparietal lobe. (B) On the 7th day of admission, the hemiparesis and mild mental deterioration had been developed. The follow-up CT scan showed increase of a mixed density SDH and severe midline shifting. (C) A CT scan 6 days after trephination (after instillation of urokinase: 3 times for 3 days), representing marked decrease of the SDH and resolution of the mass effect. (D) A follow-up CT scan at postoperative 1 month showed no residual hemorrhage and mass effect.CT: computed tomography, SDH: subdural hematoma.
|
Go to :
DISCUSSION
Because of the increment in cardiac and cerebral disease, the patients taking antithrombotic medications (antiplatelets or anticoagulants) are recently increasing. In addition, ASDHs or chronic subdural hematomas caused by minor injuries are increasing by aging population. Especially in the elderly who take these medications, ASDH is reported to occur well.1016171819) The hematomas should be removed immediately in acute cases by craniotomy or craniectomy if the neurologic signs get worse with increased intracranial pressure, or if the thickness of the hematoma is more than 10 mm with midline shifting over 5 mm in CT scan.2) That is the principle operation method of ASDH with general anesthesia. However, the morbidity of surgery for head injury can rise in elderly patients because body's ability to maintain homeostasis decreases with aging, and various underlying diseases can easily lead to complex systemic complications.922) Age is a major determinant of outcome from ASDH. It is estimated that the probability of a poor outcome increases by 40–50% with every decade of life.12) Furthermore, mortality appears to be 4 times more likely in patients who are over 65 years of age than in adults who are under 40 years of age.12) There are several risk factors associated with surgery, those are complications from the general anesthesia due to medical disorders, the surgery itself and excessive blood loss due to antithrombotic medication. So, we can try delayed operation in those cases if patients have clear mentation or mild mental deterioration, or if CT findings show minimal midline shifting despite a significant amount of hematoma. The pathomechanism of these findings can be presumed as follows: 1) the bleeding take place slowly, causing the brain compression to slow down. 2) In the elderly, brain atrophy leads to a low intracranial pressure and a slow increase of it.
ASDH occur within 72 hours after injury, and subacute subdural hematoma is occurring between 4 to 20 days after receiving an injury.811) A hematoma may increase suddenly in the subacute stage during conservative treatment of ASDH, requiring operation. The principal mechanism of rapid expansion of those hematomas may be an influx of cerebrospinal fluid into the subdural hematoma cavity from a torn arachnoid membrane and lysis of the subdural hematoma. Impaired autoregulation in the hyperperfused state was proposed to explain the development of a subacute subdural hematoma.620) At that time, the hematoma may be partially liquefied, so we propose a trephination with drainage using UK under local anesthesia if neurologic condition of the patient is good state. When the drainage flow of liquefied blood stops during catheterization, instill UK into the subdural space after CT confirming of coagulated hematoma. Even if a small amount of blood is drained, the intracranial pressure can be significantly reduced, so brain can withstand the compression effect of hematoma. The advantage of using UK is that it takes less time to remove the hematoma than spontaneous liquefaction of clot, which shortens the duration of treatment. After the partial drainage of hematoma, draining only the liquefied hematoma and leaving the rest of the coagulated hematoma may worsen the clinical state, because the remnant coagulated hematoma can expand again. So, using UK is much more useful. The dosage and injection times of UK may be variable depending on the degree of hematoma liquefaction and midline shifting in serial CT scans. In our cases, we injected up to 6 times for 4 days.
Trephine drainage using UK is usually performed as safe method to reduce the intracranial pressure or remove hematoma by draining cerebrospinal fluid or hematoma in spontaneous acute intraventricular or intracerebral hemorrhage.351321) We think that UK instillation after trephine hematoma drainage can be a good minimal invasive treatment method for the patients with good GCS score regardless of age, the patients who had a risk of bleeding due to antithrombotic medication, and it may be more helpful for aged decrepit patients.
Several reports revealed also good results in the treatment of chronic subdural hematoma or traumatic epidural hematoma or subdural hematoma that does not require emergency craniotomy with UK using trephination.141415) Because this study was based on a small number of cases, more cases are needed for further analysis of the effectiveness and usefulness of this surgical procedure. In addition, it may also be necessary to compare with craniotomy for hematoma removal with ASDH.
Go to :
CONCLUSION
It is thought to be useful operation method in selected patients with ASDH that the subdural drainage in subacute stage with UK instillation under local anesthesia. It was safely performed in patients with subacute or chronic subdural hematoma as reported in other studies. This is a minimally invasive and effective method for patients not suitable for general anesthesia, especially the elderly and might be another useful option for the patients with good mental state regardless of age and the patients with a risk of bleeding due to antithrombotic medications.
Go to :
 XML Download
XML Download