

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Active surveillance culture (ASC) can elucidate hidden reservoirs, which may be delayed or entirely missed in culture results obtained during routine clinical care [1]. To date, there is no consensus regarding the routine use of ASC for extended spectrum β-lactamase-producing Enterobacteriaceae (ESBL-E) in a non-epidemic situation. In most Korean hospitals, ASC has not been routinely recommended because of the low prevalence and cost. However, as the epidemiology changes continuously, the usefulness of ASC should be evaluated considering local epidemiological data and patient vulnerability.
Klebsiella pneumoniae isolates are a common cause of infections in intensive care unit (ICU) patients, and colonizers in the gut could be a source of infection [2]. According to a Korean Global Antimicrobial Resistance Surveillance System (Kor-GLASS) report based on 2017 data, the resistance rate to cefotaxime was 27% in K. pneumoniae blood isolates from May 2016 to April 2017 in six sentinel hospitals [3]. The antimicrobial resistance rate to cefotaxime in K. pneumoniae isolates from ICU patients is higher than that of non-ICU patients [2].
Society for Health Care Epidemiology of America recommends screening methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci carriers, based on early research conducted in the mid-2000s [4]; however, there was not enough evidence for the usefulness of screening ESBL-E [5]. To fill this gap and add to the existing knowledge, we aimed to evaluate the prevalence and risk factors for ESBL-producing K. pneumoniae (ESBL-Kpn) colonization in ICU patients. We hope this data will provide the background evidence for applying routine active surveillance for ESBL-Kpn colonization in high-risk patients as an infection-control policy. The study was approved by the Institutional Review Board of National Health Insurance Service Ilsan Hospital, Goyang, Korea (NHIMC 2018-04-001), which waived the need for informed consent.
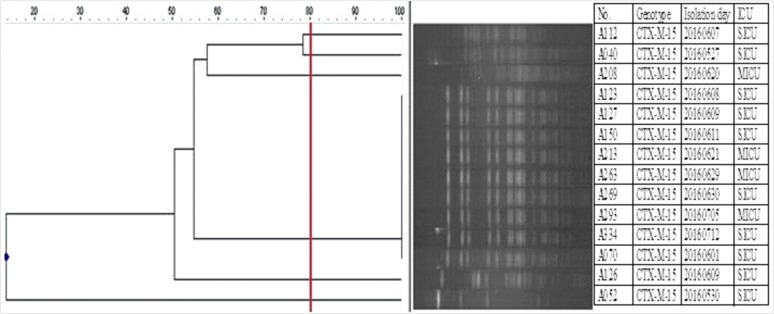
From May to July 2016, ESBL-Kpn colonization was screened prospectively within 48 hours for all 281 patients admitted to a surgical or medical ICU at a general hospital in Gyeonggi-do province, Korea. ASC was carried out on perirectal swab samples, which were then inoculated on MacConkey agar supplemented with 2 µg/mL ceftazidime. Identification and susceptibility testing were performed using a MicroScan WalkAway plus system (Beckman Coulter Inc., West Sacramento, CA, USA) and a MicroScan Neg Breakpoint Combo Type 44 panel (Siemens Healthcare Diagnostics Inc., West Sacramento, CA, USA). Antibiotic susceptibility was interpreted using the CLSI guidelines [6]. ESBL-genes were identified by PCR and direct sequencing using gene-specific primers [7]. Cases with a discrepant phenotype and genotype, which showed a positive ESBL result by MicroScan without detection of ESBL genes, were confirmed using a double-disk synergy test [8]. Pulsed-field gel electrophoresis (PFGE) was performed, and the patterns were analyzed using InfoQuest FP software (Bio-Rad, Hercules, CA, USA) to generate a dendrogram based on the unweighted pair-group method, with an arithmetic average (UPGMA) based on Dice's coefficient with 1% band-position tolerance and 0.5% optimization settings [9].
For risk factor analysis, a case-control study with a 1:4 ratio (18 cases and 72 controls) was conducted. The control group included randomly selected patients without ESBL-E isolation in ASC. Clinical information (age, sex, hospital stay, site of acquisition, previous antibiotic use within 90 days before ASC, and ICU types) was collected by reviewing the medical records. Sites of acquisition were identified as described by Friedman, et al. [10] with some modifications. Briefly, hospital-acquired infection/colonization was defined by a positive culture obtained from patients who had been hospitalized for 48 hours or longer. Community-onset infection/colonization was defined by a positive culture obtained at the time of hospital admission or within 48 hours post admission. Community-onset consisted of two groups: community-onset healthcare-associated and community-associated. Community-onset healthcare-associated cases had any of the following histories: attended a hospital or hemodialysis clinic or received intravenous chemotherapy in the last 30 days; hospitalized in an acute-care hospital for two or more days in the last 90 days, or were transferred-in from another healthcare facility before K. pneumoniae isolation. The remaining cases were defined as community-associated.
The age and hospital days were summarized as median, and other variables as N (%) of patients. Continuous variables, such as age, were analyzed using the Mann-Whitney U test. Categorical variables were compared using the chi-squared test to identify independent risk factors. Odds ratio (OR) and 95% confidence interval (CI) were calculated for binomial variables. Variables with P<0.1 in univariate analyses were included, if multivariate logistic regression analysis was needed to identify independent risk factors for ESBL-Kpn colonization. Statistical significance was defined as P<0.05. Data were analyzed using SPSS version 23 (IBM Corp., Armonk, NY, USA).
The ESBL-Kpn colonization rate among the 281 patients at ICU admission was 6.4% (18/281), and blaCTX-M-15 was detected in all isolates. ESBL producers also showed resistance to fluoroquinolone (38.9%, 7/18). The PFGE profiles showed one clustered group and other heterogeneous patterns with 80% similarity (Fig. 1).
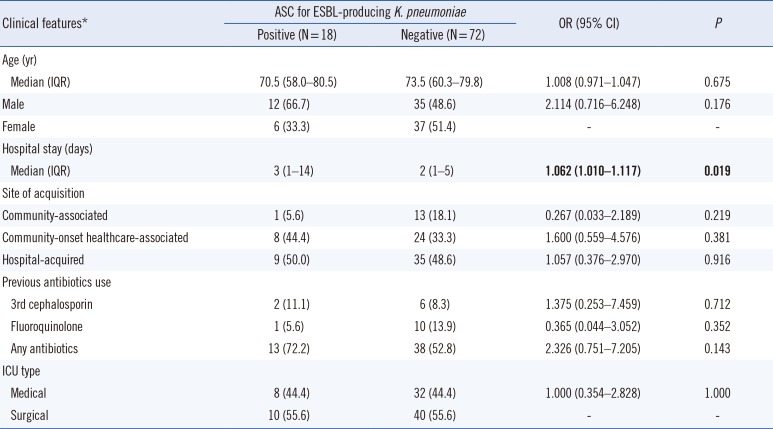
In univariate analysis, the only significant risk factor for ESBL-Kpn colonization over the control was hospital stay (OR=1.062; P=0.019). Other factors, such as site of acquisition, previous antibiotic use, and ICU type were not statistically significant (Table 1).
Gastrointestinal colonization by K. pneumoniae has been confirmed as a significant risk factor for infection in ICUs; a half of K. pneumoniae infections originate from patient microbiota [11]. Disruption of normal barriers, for example by gastric acidity and colon microflora, facilitates the overgrowth of pathogens; many mechanisms, including bacterial translocation from the gut and exogenous translocation via contaminated skin, can contribute to these infections [12]. Furthermore, patient with gastrointestinal problems, such as fecal incontinence and diarrhea, could result in the spread of pathogens into the health-care environment, and treatment with antibiotics places a higher selective pressure on colonization by the pathogen [12].
Infections by a multi-drug resistant pathogen, such as ESBL-Kpn, which usually carries resistance to other classes of antibiotics, could fail to respond to treatment, increasing medical costs, prolonging hospital stays, and elevating the socioeconomic burden [13]. K. pneumoniae is one of the most important hospital pathogens, with a high mortality rate, particularly due to multidrug-resistant ESBL-producing strains [14]. Moreover, K. pneumoniae is known to be 3.7-fold more transmissible than Escherichia coli in mathematical modeling analysis, although the underlying factors of this higher transmissibility have not been elucidated [15]. In our study, the prevalence of ESBL-Kpn colonization was 6.4% at ICU admission. In previous studies, ESBL-Kpn carriage rates ranged from 45% (18/40) to 6.9% (24/347) in ICU patients [1617].
The ESBL-Kpn isolates in our study had the same genotype (blaCTX-M-15), and nine of the 14 isolates showed identical PFGE patterns, suggesting cross-transmission without a documented outbreak. A limitation of this study was that we used ceftazidime in ASC, which could result in the low detection of CTX-M-14 type because the hydrolysis of ceftazidime is lower than that of cefotaxime with this CTX-M type. We could not detect carbapenem-resistant K. pneumoniae; although the prevalence of carbapenem-resistant Enterobacteriaceae (CRE) is still low in Korea [18], the recent sharp rise in CRE caused by carbapenemase-producing Enterobacteriaceae (CPE) has created challenges for infection control in Korea [19]. K. pneumoniae is the most common bacterial type of CPE, carrying various types of carbapenemases, such as K. pneumoniae carbapenemase, New Delhi metallo-β-lactamase, and OXA-type carbapenemases [20]. Given that CPE may emerge in Korea, the routine application of ASC not only for ESBL-Kpn but also for CPE for ICU patients should be considered in the near future.
 XML Download
XML Download