

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The term “biological treatment” refers to a variety of treatments of natural origin (e.g., vaccines, blood, blood components, gene therapy, and recombinant proteins), but it has typically come to be used in relation to a subgroup of large, complex molecules used for targeted therapy, including monoclonal antibodies (moAbs) and receptor fusion proteins. Unlike small molecules, which have low molecular weight and are capable of crossing the cell membrane and acting intracellularly, these biological agents are high-molecular-weight proteins that have to be injected, because they would be degraded in the gastrointestinal tract if administered orally, and act on the cell surface or extracellularly. Furthermore, they are produced in specialized live cells, whereas small molecules are simpler and can be chemically synthesized.
The nomenclature of receptor fusion proteins and moAbs follows the rules of the International Nonproprietary Names selected by the World Health Organization. The suffix “-cept” is used to identify receptor molecules (e.g., etanercept [ETA]), whereas “-mab” is used to identify moAbs; antibodies of fully human origin have the addition of “-mu-” (e.g., adalimumab [ADA]), whereas those with both human and murine origin are humanized (“-zu-”, e.g., ixekizumab) or chimeric (“-xi-”, e.g., infliximab) [1]. Biological drugs were introduced into clinical practice nearly 20 years ago and have now become powerful means of treating patients with chronic immuno-inflammatory arthritis, such as rheumatoid arthritis (RA), juvenile idiopathic arthritis, psoriatic arthritis (PsA), and spondyloarthritis (SpA), including ankylosing spondylitis (AS) and non-radiographic axial SpA. They are a major alternative for patients with these conditions who do not respond to or tolerate conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs, such as methotrexate, sulfasalazine, and leflunomide). The biological drugs used to treat immuno-inflammatory arthritis are genetically engineered human proteins that inhibit specific components of the immune system involved in enhancing inflammation by neutralizing cytokines via soluble receptors or moAbs, receptor blockade, or anti-inflammatory pathway activation [2]. Table 1 shows the currently available biological agents for treatment of immuno-inflammatory arthritis. However, some patients fail to respond to initial treatment or lose responsiveness, and some patients have to discontinue the biological agents because of side effects.
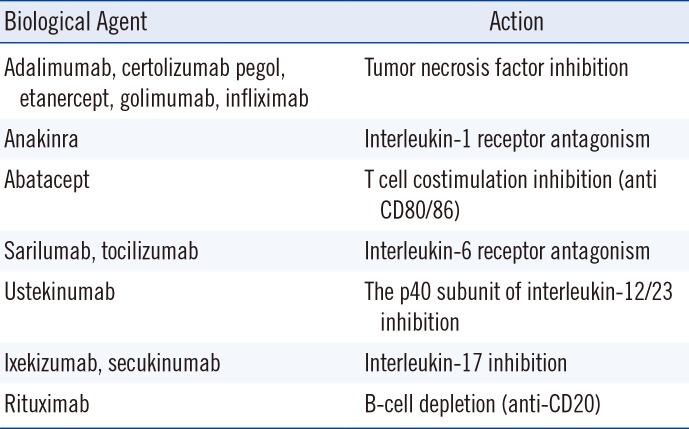
Table 1
The seven currently available classes of biological agents
![]()
Biological agents positively interfere with the structural damage associated with immuno-inflammatory rheumatic diseases, and they have an excellent risk/benefit profile as they significantly decrease cardiovascular risk and mortality. The choice of a specific agent for a particular patient mainly depends on clinical considerations, such as safety profile and dosing frequency of the candidate drug, the route and mode of administration, and the presence of comorbidities. However, it is also influenced by economic consideration, because of the high cost of these drugs and administrative restrictions. Thus, although they are highly effective in the treatment of rheumatic diseases and can be considered cost-effective in patients not responding adequately to conventional treatment, biological agents are unlikely to be prescribed as a first-line or even second-line treatment.
“Biosimilars” have been introduced as a means of increasing access to biological treatment in a more affordable manner. According to the US Food and Drug Administration (FDA), a biosimilar is a pharmaceutical product that is highly similar to its reference product (RP, or originator) “notwithstanding minor differences in clinically inactive components”; therefore, there is “no clinically meaningful difference” between them in terms of safety, purity, or potency [3]. Biosimilars are produced in living systems using complex purification techniques and recombinant DNA technology, and they are pharmacokinetically bioequivalent to their originators [4]. They also require similar storage techniques and transport technology [4]. Originators and biosimilars have dramatically improved outcomes in rheumatic diseases for which they have been used, and have contributed to making remission a realistic target. In addition to being good alternatives for patients who cannot be treated with csDMARDs, they offer additional therapeutic choices for healthcare providers and patients. The competition between originators and biosimilars should increase access to biological treatments. However, challenges, such as the lack of long-term safety data and the need for biological registries, and questions concerning when and how to switch from an originator to a biosimilar remain and should be considered by rheumatologists.
Go to : 
SERUM DRUG LEVELS, ANTI-DRUG ANTIBODIES, AND CLINICAL RESPONSES
Several studies have evaluated the correlation between anti-tumor necrosis factor (TNF) drug antibodies, serum drug levels, and clinical responses (Table 2). The RISING study [5] assessed the effect of infliximab (IFX) plus methotrexate (MTX) on radiographic and clinical responses in 334 patients with RA (including patients with active RA despite treatment with MTX for more than 12 weeks) attending 88 Japanese medical centers. It compared maximum (10 mg/kg) and minimum (3 mg/kg) IFX doses, and investigated whether the effects on responses were related to trough serum IFX levels. All the patients received 3 mg/kg of IFX plus MTX in weeks zero, two, and six, after which they were randomized to receive 3, 6, or 10 mg/kg of IFX every eight weeks plus stable doses of MTX. The primary end points were the attainment of American College of Rheumatology (ACR) responses (ACR20, ACR50, and ACR70), a change in the 28-joint Disease Activity Score (DAS28), and a change in the European League Against Rheumatism (EULAR) response criteria. Radiographic progression was assessed using the Modified Total Sharp Score (TSS). Physical function was evaluated using the Health Assessment Questionnaire (HAQ). Trough serum IFX levels were measured by ELISA and a moAb against IFX, and were subsequently correlated with DAS28 and TSS results obtained in week 54.
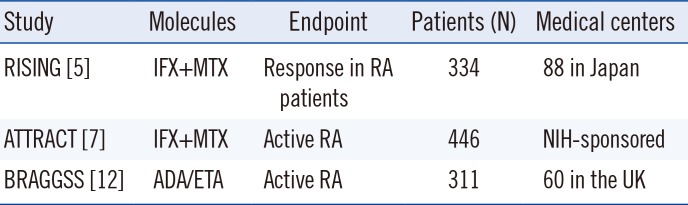
Table 2
Studies evaluating correlations between anti-TNF drug antibodies, serum drug levels, and clinical responses
| Study | Molecules | Endpoint | Patients (N) | Medical centers |
|---|---|---|---|---|
| RISING [5] | IFX+MTX | Response in RA patients | 334 | 88 in Japan |
| ATTRACT [7] | IFX+MTX | Active RA | 446 | NIH-sponsored |
| BRAGGSS [12] | ADA/ETA | Active RA | 311 | 60 in the UK |
![]()
Of the 334 patients, 272 completed the study; the main causes of withdrawal from the study were adverse events, similar to those in the three treatment groups. Trough serum IFX levels in the 3, 6, and 10 mg/kg groups were 0.4, 2.3, and 5.5 µg/mL, respectively, indicating dose dependency, and were significantly associated with clinical response; a better EULAR response was observed in patients with higher trough serum levels (P<0.0001). Higher trough serum levels were also observed in the patients achieving remission (P<0.0001), and trough serum levels were significantly correlated with DAS28 remission (P<0.0001). Patients with lower trough serum levels more frequently experienced progressive joint damage, and there was no improvement in their TSS; no joint damage progression was observed in the patients with trough serum IFX levels of >10 µg/mL. The inhibition of joint damage progression was directly related to the increase in trough serum IFX levels: the median trough serum level was <0.1 µg/mL in non-responders and 1.1 µg/mL in responders, suggesting that a trough serum level of 1.0 µg/mL is the threshold for a clinical response. Trough serum IFX levels are affected by serum clearance of IFX and the production of anti-IFX antibodies [6], which seems to have the greatest effect on the efficacy of IFX treatment. The relationship between trough serum IFX levels and the incidence of adverse events was not investigated.
The ATTRACT trial [7] aimed to establish the relationship between serum IFX levels and clinical improvement, and included 428 patients with active RA. IFX was administered at 3 mg/kg or 10 mg/kg every four or eight weeks in combination with weekly MTX (pharmacokinetic models were used to predict the trough serum levels of the doses not directly tested in the trial). Serum IFX levels were measured by ELISA one hour after infusion to approximate the maximum drug level. Trough serum levels directly correlated with the intravenous dose, with the group receiving 10 mg/kg having the highest median level, and a few patients having undetectable trough levels. Clinical improvement was measured using ACR20, ACR50, and ACR70 responses. The ACR20 response rate was similar in the treatment groups, whereas the ACR50 response rate was significantly lower in the group receiving 3 mg/kg every eight weeks; the highest proportions of ACR50 and ACR70 responses were observed in the patients with the highest trough serum IFX levels (both P<0.001). Serum levels were also correlated with laboratory measures and radiographic scores: higher trough levels were associated with a reduction in C-reactive protein (CRP) levels (P<0.001) and less progressive joint damage (P=0.004). Within the groups, there was individual variability in serum IFX levels because of drug clearance; non-responders tended to eliminate IFX more rapidly than responders. The lack of a response to anti-TNF drugs is often due to the development of anti-drug moAbs, which reduces the treatment response and lead to treatment discontinuation [89]. The 2013 research agenda of the EULAR task force for the management of RA included investigating whether serum drug and/or drug antibody levels are clinically useful variables [10]. When considering the results of immunogenicity studies, it is important to bear in mind that wide variation in anti-drug antibody frequency may be due to patient-related factors, associated treatments, such as the concomitant use of csDMARDs, differences in detection methods, and differences in free drug levels. RIAs seem to be less susceptible to drug interference than ELISAs [11], and drug interference can be avoided by using trough serum drug and anti-drug antibody levels obtained immediately before the administration of the next scheduled dose.
The Biologics in Rheumatoid Arthritis Genetics and Genomics Study Syndicate (BRAGGSS) study [12] involved 311 patients with active RA enrolled from 60 centers in the UK and investigated treatment responses in relation to anti-drug antibodies. All the patients were prescribed ADA or ETA at enrollment, and serum levels and disease activity were measured after three, six, and 12 months during routine clinic visits. Therapeutic responses were evaluated using the EULAR response criteria and/or a change in DAS28. Serum non-trough drug levels were tested in serial samples using ELISA. The presence of anti-drug antibodies was determined by RIA, with serum anti-drug antibody titers of >12 arbitrary units (AU)/mL being considered positive in both treatment groups. Anti-ADA antibodies were detected in 24.8% of the patients and were significantly associated with lower serum ADA levels (P<0.0001). Most patients with anti-drug antibodies (90.3%) developed immunogenicity within six months. The main baseline difference between the patients who developed anti-drug antibodies and those who did not was the median dose of MTX, which was significantly higher in the latter. Further, disease duration before biological treatment was longer in the patients with anti-drug antibodies.
Serum ADA levels and anti-ADA antibody status were significantly associated with a change in DAS28 after 12 months (P<0.0001), whereas the 12-month EULAR response was associated positively with serum ADA levels but negatively with anti-ADA antibody status. The ADA concentration—effect curve showed that a drug level of <5 mg was associated with a smaller change in DAS28, and that the optimal therapeutic window was 5–8 µg/mL; no EULAR response was observed in the patients with drug levels of <0.1 mg (P<0.0001). The strongest predictor of low drug levels over time was anti-drug antibody status (P<0.003). Serum ETA levels were associated with a 12-month EULAR response, but this association seemed to lose significance after adjusting the confounders of age, sex, body mass index (BMI), disease duration, and drug adherence. Moreover, the ETA concentration—effect curve did not reveal a clear therapeutic window to indicate an optimal treatment response. These results suggest that non-trough ADA and anti-ADA antibody status are useful for predicting no EULAR response after 12 months, whereas non-trough ETA levels are not. These findings are consistent with those of other studies demonstrating that treatment failure is higher in patients developing anti-drug antibodies to moAbs [813]. The study also showed an inverse correlation between anti-drug antibody and drug levels, suggesting that measuring anti-drug antibodies may be useful in orienting the therapeutic option in non-responders. Interestingly, the patients receiving lower MTX doses were more likely to develop immunogenicity. BMI and adherence also influenced drug pharmacokinetics and thus treatment responses.
ADA can induce anti-ADA antibodies, which are associated with low free drug levels and a clinical non-response. Most of the assays used to detect these antibodies may be affected by serum drug levels, but the sensitivity of an ELISA can be improved by using acid to dissociate the ADA-mAb immune complexes [1314]. One study measured the clinical usefulness of acid dissociation by monitoring 238 serum samples taken every three to six months from 116 ADA-treated patients over a period of three years [15]. Trough serum ADA and anti-ADA antibody levels were measured by ELISA, and 32 samples from 22 patients with sub-therapeutic ADA levels were analyzed before and after acid dissociation. Before acid dissociation, these patients were found to be antibody-negative, but dissociation led to the detection of anti-ADA antibodies in 17 of the 32 samples. In case of low antibody titers, most of the antibodies are bound with the drug, whereas high titers lead to more free antibodies, which are easier to detect. Furthermore, the increase in antibody detection after acid dissociation is significant in the presence of low ADA levels. This means that acid dissociation may aid in clinical decision making in the case of a reduced response, as the presence of anti-ADA antibodies is one of the major causes of a loss of therapeutic effect.
ADA, IFX, and ETA can induce the development of anti-drug antibodies, which are also responsible for side effects, such as injection-site and infusion reactions, thromboembolic events, and serum sickness. Up to 44% of IFX-treated patients develop anti-IFX antibodies during the first six months of treatment [1617], and the same is true of up to 19% of ADA-treated patients [18]. The incidence of generally non-neutralizing anti-ETA antibodies is 0–7%, and some studies failed to confirm the drug's immunogenicity [81920]. One international, cross-sectional study assessed the immunogenicity of ETA, ADA, and IFX and its impact on trough serum drug levels and clinical responses in 600 patients with active RA divided into approximately equal treatment groups [21]. The patients were monitored by disease activity assessments, patient-reported outcomes, and trough serum drug (ELISA) and antidrug antibody (RIA) levels. The baseline characteristics and mean duration of treatment were similar in the three groups. None of the ETA-treated patients had detectable anti-ETA antibodies, whereas 31.2% of those treated with ADA and 17.4% of those treated with IFX did (P<0.0001), indicating the greater immunogenicity of ADA and IFX. The incidence of anti-drug antibodies was higher in the patients treated for 6–12 months than in those treated for 12–18 or 18–24 months, and lower in those receiving concomitant MTX, although the difference between those who received and did not receive MTX was not statistically significant. Pooled data for all three TNF inhibitors showed that patients with low disease activity were more often negative for anti-drug antibodies: 66.5% of the patients treated with ETA, 64.5% of those treated with ADA (of whom 65.2% had no detectable antibodies), and 51.6% of those treated with IFX (of whom 53.3% had no detectable antibodies). In total, 44.1% of patients were in remission, and a significant proportion of them (44.1%, P=0.0046) were antibody-negative. Trough serum ADA and IFX levels were lower in the patients with detectable anti-drug antibodies (80.5% and 98%, respectively; P<0.0001). Composite disease activity measured based on the DAS28-erythrocyte sedimentation rate (ESR), DAS28-CRP, the Clinical Disease Activity Index, and the Simplified Disease Activity Index was relatively higher in the patients with detectable anti-drug antibodies. There was no significant difference in the proportion of patients with or without detectable anti-drug antibodies in the IFX and ADA groups. Overall, the patients treated with ADA or IFX who developed anti-drug antibodies had significantly lower trough serum drug levels and higher CRP levels and a higher ESR, but there was no significant correlation with DAS28-ESR remission or the Health Assessment Questionnaire Disability Index (HAQ-DI). However, trough serum ADA levels negatively correlated with DAS28-CRP, DAS28-ESR, HAQ-DI, Euro Quality of Life Health Status (EQ-5D), and the 36-Item Short Form Health Survey (SF-36) general health score, indicating that lower trough serum ADA levels—which may be due to the development of anti-drug antibodies—is related to greater disease activity and an impaired quality of life. In contrast, trough serum IFX levels did not significantly correlate with treatment efficacy or health outcome measures. In brief, although further prospective studies are required, these findings suggest that anti-drug antibodies develop in a higher proportion of patients receiving an anti-TNF moAb (ADA or IFX) than in those treated with a TNF receptor fusion protein (ETA). Furthermore, the presence of anti-ADA or anti-IFX antibodies is associated with lower serum drug levels and poorer efficacy outcomes. Treatment failure is more frequent in patients developing anti-drug antibodies to moAbs, and there is an inverse correlation between anti-drug antibodies and drug levels, suggesting that measuring anti-drug antibody levels may be useful in non-responders.
Go to :
IMMUNOGENICITY OF ANTI-TNF AGENTS IN RA
bDMARDs, an important class of drugs that are frequently used to treat RA, have significantly reduced disease activity levels and improved the quality of life of patients who did not respond to csDMARDs [22]. However, up to 30% of the patients treated with bDMARDs show no or inadequate response to initial treatment (primary failure), and more than 30% of initial responders experience a loss of response over time (secondary failure) or develop potentially therapy-limiting adverse events [23].
Five anti-TNF agents have been licensed in Europe for the treatment of RA: IFX (a mouse-human chimeric moAb against TNF) and ETA since 1998; ADA since 2003; and, more recently, golimumab (GLM) and certolizumab pegol (CZP) [24]. Since the expiry of the patents of the first three anti-TNF agents, their biosimilars have also been used. All these anti-TNF drugs are high-molecular-weight proteins and are therefore inherently immunogenic, and the generation of anti-drug antibodies is related to treatment failure or the development of adverse events [25].
Two recent systematic reviews revealed that the proportion of RA patients who develop treatment-induced anti-drug antibodies varies: the incidence is the highest in those treated with IFX (0–83%), followed by those treated with ADA (0–54%), CZP (3–25%), GLM (0–19%), and ETA (0–13%) [1326]. The antibodies may appear as early as during the first months of exposure (in up to 44% of RA patients treated with IFX and in 19% of those treated with ADA) [1718]. Their frequency depends on not only the type of TNF inhibitor but also the measurement method used. Moots, et al. [21] have recently investigated the occurrence of anti-ETA, anti-ADA, and anti-IFX antibodies in a relatively large, multinational, cross-sectional real-world population of RA patients on stable treatment for 6–24 months, and found that none of the patients treated with ETA had detectable antibodies, whereas 24.4% of those in the pooled ADA/IFX group did, indicating the greater immunogenicity of ADA and IFX. Interestingly, almost all patients concomitantly treated with MTX developed antibodies, the rate of which may increase over time. The risk factors for developing anti-ADA/IFX antibodies in one cohort of RA patients—most of whom were naive to anti-TNF treatment and were co-treated with MTX—were a longer disease duration, higher baseline DAS28 values, and lifetime smoking (which may be associated not only with the development of anti-citrullinated protein antibodies but also with overall B-cell responses) [27]. Magill, et al. [28] have recently shown the direct involvement of memory B cells in anti-drug antibody formation; they found that a reduced level of signal regulatory protein α/β (SIRP α/β)-positive memory B cells before ADA treatment predicts the development of anti-ADA antibodies after 12 months of follow-up. However, whether this is exclusively a biomarker of response or biologically related to anti-ADA antibody development is still unknown. Bartelds, et al. [29] observed that RA patients previously treated with IFX who switched to ADA after developing anti-IFX antibodies seemed to develop anti-ADA antibodies more frequently than switchers without anti-IFX antibodies, and the highest rates of response to ADA were observed mostly in switchers without anti-IFX antibodies. These findings suggested that patients who develop antibodies against a first bDMARD are more likely to develop antibodies against a second [29] (Fig. 1).
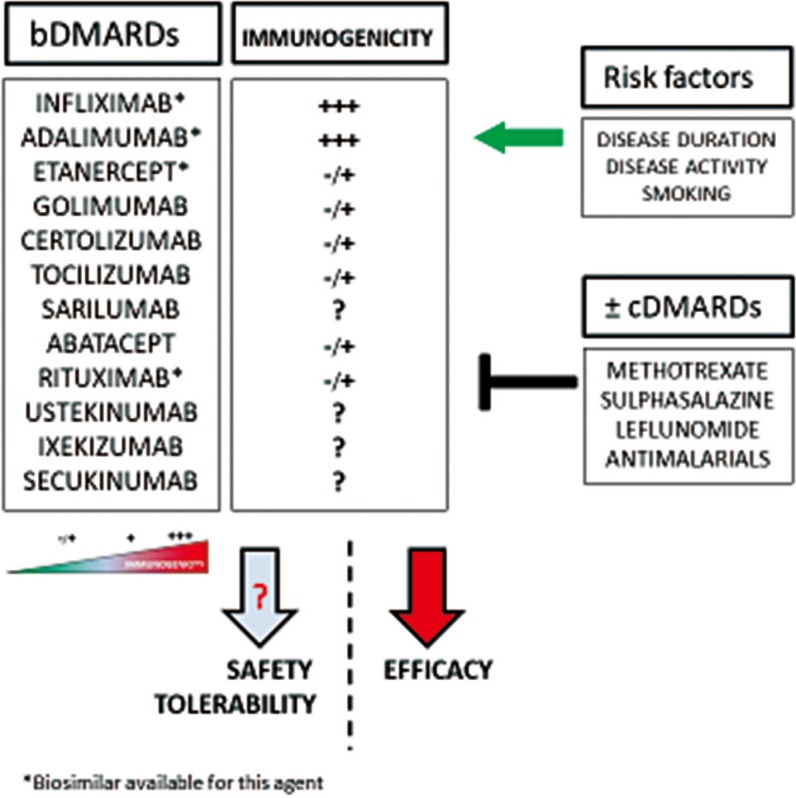 | Fig. 1Biological disease-modifying anti-rheumatic drugs (bDMARDs) are associated with immunogenicity, leading to the development of anti-drug antibodies that affect drug efficacy and may affect drug safety and tolerability. The development of anti-drug antibodies seems to be influenced by multiple risk factors and may be modulated by the concomitant use of conventional synthetic DMARDs (cs-DMARDs).
|
Anti-ADA, anti-CZP, and anti-GLM antibodies act by targeting idiotypes close to the epitope-binding portions of the Fab regions of the mAbs, thus preventing their binding to TNF and finally reducing the effects of the drugs. Moreover, the complex formed by an anti-TNF drug and its specific antibody may affect its pharmacokinetics by increasing its clearance and lowering its serum level, thus having a potentially negative impact on clinical responses. A recently reported randomized controlled trial (RCT) and real-life data showed that anti-drug antibody-positive patients treated with ADA, IFX, CZP, or GLM had lower serum bDMARD levels than those who are anti-drug antibody-negative [2130313233]. However, although one study found that serum IFX levels were low (<0.5 µg/mL) in one-quarter of RA patients, no more than 11% had detectable anti-IFX antibodies, suggesting that additional factors may be responsible for the reduced efficacy of IFX [34].
Anti-drug antibody-positive RA patients treated with anti-TNF bDMARDs have higher inflammation marker levels and greater disease activity, show less improvement in disease activity, and are less likely to achieve a clinical response even in the earliest phases of treatment [16182135]. A meta-analysis of 12 prospective cohort observational studies revealed that the presence of anti-drug antibodies reduces the rate of clinical responses to ADA or IFX by 68%, an effect that was attenuated by the concomitant use of MTX [8], which is associated with a dose-dependent reduction in the immunogenicity of anti-TNF agents, including non-chimeric agents, such as ADA [3236]. These data have been confirmed in a recent meta-analysis of 68 studies (38 RCTs and 30 observational studies) [37]. Finally, a meta-analysis of 10 studies involving 1,806 RA patients revealed that anti-drug antibody positivity was significantly associated with a reduced clinical response at all follow-up time points [38]. Antibodies against anti-TNF drugs are associated with the safety and tolerability of mainly IFX as they are related to infusion- site or other adverse drug reactions [394041].
In conclusion, the development of anti-drug antibodies in RA patients is probably frequent and related to the molecular structure, dose, and administration regimen of the bDMARDs involved, the concomitant use of MTX, and individual autoimmunity profiles (i.e., the presence of B-cell subsets), which affect not only treatment response rate but also drug safety and tolerability.
Go to :
IMMUNOGENICITY OF OTHER BIOLOGICAL AGENTS
Other agents used in the management of inflammatory diseases include abatecept (ABA, a T-cell activation inhibitor/costimulation modulator), rituximab (an anti-CD20 mAb), tocilizumab [an interleukin-6 receptor (IL-6R) antagonist], secukinumab (an IL-17A antagonist), and ustekinumab (an IL-12/23 blocker), all of which have unique protein structures and induce different immune responses. The immunogenicity of ABA has been evaluated in 10 studies; eight of these were in patients with RA and two in patients with juvenile rheumatoid arthritis (JRA). Of the first eight studies, two lasted less than 24 weeks, and six more than 24 weeks. Of the 10 studies, six assessed immunogenicity using an ELISA and four used an electrochemiluminescent (ECL) immunoassay. The receptor fusion protein ABA show immunogenicity to the linker between the soluble receptor and the Fc portion, which may partially explain the low incidence of anti-drug antibodies (2–20% in RA patients and 2–11% in JRA patients) and the absence of neutralizing activity [264243]. The immunogenicity of rituximab has been evaluated in 12 studies, seven of which lasted less than 24 weeks, and five more than 24 weeks. ELISA was used in six studies and ECL immunoassay in four, while two used unknown methods. The frequency of anti-drug antibodies was 0–21% in RA patients [2644454647].
The immunogenicity of tocilizumab has been evaluated in 22 studies, eight of which lasted less than 24 weeks, and 14 more than 24 weeks, and all of which used ELISA. The frequency of anti-drug antibodies was 0–16% in RA patients and 1–8% in JRA patients, a low incidence that may be partially explained by the fact that IL-6 is necessary for an antibody response or the poor sensitivity of the assay in the presence of circulating drug levels [26444546].
The immunogenicity of secukinumab has been evaluated in 11 studies; two involving patients with SpA, two involving patients with PsA, and seven involving patients with psoriasis. Of these, four studies lasted less than 24 weeks, and seven more than 24 weeks; six studies used ELISA, five used an ECL immunoassay. The frequency of anti-drug antibodies was 0–0.3% in SpA patients, 0–0.1% in PsA patients, and 0–1% in psoriasis patients [264445464748].
The immunogenicity of ustekinumab has been evaluated in 15 studies; 11 involving patients with psoriasis, two involving patients with Crohn's disease (CD), and two involving patients with PsA. Among these, 12 studies lasted more than 24 weeks, three less than 24 weeks. Six studies used ELISA, five an ECL immunoassay, and four RIA. The frequency of anti-drug antibodies was 0–1% in patients with CD, 8–11% in those with PsA, and 4–8.6% in those with psoriasis [26444546474849].
Go to :
IMMUNOGENICITY OF BIOSIMILARS
A biosimilar is a biological product approved on the basis of the totality of evidence demonstrating that it is highly similar to an approved biological RP in terms of its physicochemical and biological properties, clinical efficacy, and safety [50]. CT-P13 (Remsima®; Inflectra®) was the first biosimilar of INF-RP Reference Product (Remicade®) to be approved by the European Medicines Agency (EMA) and the FDA. In the pivotal randomized controlled trials that led to its approval (PLANETAS and PLANETRA), anti-drug and neutralizing antibodies (NAbs) were assessed using ECL and automated Gyros™ immunoassays, respectively. Anti-drug antibodies were detected at a higher rate in RA patients than in patients with AS, but these proportions were comparable in those treated with CT-P13 and those treated with the RP; furthermore, the antibodies persisted throughout the study period in 80–90% of the patients in whom they were detected [5152]. Thirteen studies on CT-P13 have been published to date (seven on RA, four on SpA, and two on CD), and anti-drug antibodies have been detected in 26–52% of RA patients, 27% of SpA patients, 24% of ulcerative colitis (UC) patients, and 21% of CD patients. Twelve studies lasted more than 24 weeks; three used ELISA and nine an ECL immunoassay. One recent study demonstrated that antibodies against CT-P13 recognize and bind the RP, and vice versa, indicating that the two drugs share immunodominant epitopes. The findings of this study are consistent with the previously reported close biosimilarity between CT-P13 and the RP and suggest that marketed kits for detecting anti-drug antibodies against infliximab can be used to detect both [53].
Overall rates of anti-drug antibody positivity and consequent immunogenicity were similar in the recipients of SB2, another biosimilar of INF-RP (Remicade®), and those receiving IFX-RP (62.4% vs 57.5% by week 54) [54]. During the switching period, immunogenicity remained similar between the two treatment groups. Of the patients who were anti-drug antibody-negative up to week 54, antibodies developed in 14.6% of those who switched from the RP to SB2, 14.9% of those who remained on the RP, and 14.1% of those of who remained on SB2 [54]. Data on SB4, a biosimilar of etanercept RP (Enbrel®), were published in a 52-week study of patients with RA [55]. The anti-drug antibody detection rate was significantly lower in the SB4 group than in the etanercept RP group during the first 24 weeks of treatment (0.7% vs 13.1% of patients; P<0.001) [55] and at the end of the 52-week study (1.0% vs 13.1% of patients; P<0.001) [56]. However, the EMA identified confounding factors that may have introduced a bias towards SB4 and declared that it was premature to conclude that SB4 is less immunogenic than the RP [57]. The overall incidence of anti-drug antibodies after week 52 was 0.8% in the SB4/SB4 group and 0.9% in the RP/SB4 group [58]. Only one patient in the RP group developed NAbs.
GP2015, a biosimilar of ADA, has been tested for immunogenicity only in the dermatological EGALITY trial [59]. Anti-drug antibodies (all low-titer and non-neutralizing) were detected in six patients, including five etanercept RP recipients (1.9%) who tested positive during the first four weeks of the 24-week treatment period, but negative at subsequent time points. The incidence of anti-drug antibodies against CT-P10, a biosimilar of rituximab, and the rituximab RP is similar. In a phase 1 trial involving RA patients, 17.6% of the recipients of either had detectable anti-drug antibodies by week 24 after one course of treatment. Anti-drug antibodies were detected in 5.1% of CTP10 and 3.2% of rituximab RP recipients over a period of 12 weeks [6061]. In another study of RA patients [62], binding anti-drug antibodies developed in 16.5% of patients receiving GP2013, another biosimilar of rituximab, and in 15.1% of rituximab RP recipients [62], but 7.1% and 9.6%, respectively, of the cases were transient. Nabs were detected in 3.9% of the GP2013 recipients and 0.6% of the RP recipients.
Go to :
THERAPEUTIC MONITORING OF BIOLOGICAL AGENTS: THE ROLE OF THE LABORATORY
Biological agents, especially TNF inhibitors, have been a major support in the management of rheumatic diseases, but most of the therapeutic proteins induce a complex immune response and the formation of antibodies, which lead to loss of efficacy by eliminating the pharmacological action of the drug or altering its pharmacokinetics. Therefore, it is very important to use sensitive, specific, and validated methods for assessing immunological responses. Therapeutic drug monitoring (TDM) has emerged as an effective means to optimize treatment to maximize its benefits. TDM can inform medical decisions in the case of primary failure or secondary loss of response and should also be considered periodically in patients in clinical remission or those for whom a drug holiday is contemplated. Drug and anti-drug antibodies monitoring can help clinicians to understand the cause(s) of treatment failure, a sub-optimal response, infusion reactions, or secondary failure [6131763]. Screening assays should be sensitive, specific, and capable of detecting all isotypes of antibodies against a given biological drug and the available analytical assays include ELISA, RIA and new platforms, such as ECL and the automated Gyros technology [1351526465]. However, the detection and measurement of antidrug antibodies is complex, and the results can be affected by the assay used. Bridging ELISA with the antigen immobilized on the plate is a simple approach that is acceptably sensitive, but it is also associated with a very high false positivity rate, and anti-drug antibodies measurement can be confounded by the presence of rheumatoid factor and anti-hinge antibodies [1366].
Interference by the circulating drug is another major challenge for immunogenicity assays because it may lead to false-negative results as the current antibody assays only measure unbound antibodies and not those bound in immune complexes. Therefore, when interpreting antibody assessment results, the drug dose, timing of administration, and serum drug level should be considered [67]. To minimize interference in anti-drug antibody assays, blood samples should be collected immediately before the next administration, when drug levels are at their lowest [68]. New technologies allow the identification of specific isotypes of anti-drug antibodies with excellent sensitivity, allowing smaller sample volumes, minimizing the use of critical reagents, and saving time, while limiting the cost of consumables [69]. However, the short incubation time for neutralization and bridging reactions may not be sufficient if low-affinity antibodies are present in the sample.
Repeated testing is useful to determine whether the antibodies are transient or persistent and may also be appropriate for patients who respond to treatment, but initially have low antibody titers. Confirmatory assays are necessary to eliminate false-positive results and a common approach is to add an excess of antigen to the sample, which should reduce the positive signal of truly positive samples [70]. The determination of NAbs is an important part of an immunogenicity assessment and is usually done using cell-based and non-cell-based assays [71]. Given the difficulty in detecting anti-drug antibodies and determining the relationship between serum levels of biological drugs and the development of immunogenicity, it seems that testing trough serum drug levels may not only allow personalized drug dosing but it could also be cost-effective [72]. In the case of a lack or loss of efficacy of a biological agent, the drug level can provide important information: in the case of a low trough serum level, an insufficient dose or immunization against the drug should be considered. If the serum drug level is sufficient, it is likely that the choice of the target is not appropriate and switching to another biological drug class should be considered.
Various analytic techniques are used to measure the levels of anti-TNF drugs, such as ELISAs, RIAs, functional cell-based reporter gene assays, and homogeneous mobility shift assays. However, there is no single gold standard technique and, although drug levels measured using different assays may correlate with each other and lead to the same clinical decision, there are some systematic differences [7374757677787980818283]. A recent meta-analysis revealed that 20–30% of test results are likely to be incorrect because different tests use different cut-off values, suggesting that more clinical trial evidence from test-based studies is needed to optimize their use in clinical practice [84]. To improve therapeutic decision making, the same assay should be used during follow-up of a patient [85]. Finally, commercially available IFX ELISAs can also be used to quantify biosimilars without the need for any adjustment [8687]. As most of the ELISAs used for TDM require the analysis of multiple samples simultaneously, it takes at least one or two weeks before the results become clinically available in a cost-effective manner. Furthermore, as blood samples are collected immediately before an infusion, TDM results become available only at the time of the next scheduled infusion. In an attempt to overcome this drawback, some rapid tests for measuring serum IFX levels have been introduced and quantitatively and qualitatively validated in comparison with conventional ELISAs. These point-of-care tests may be advantageous in the case of non-responding patients as they allow low IFX levels to be detected by a nurse, physician, or researcher during the course of a single outpatient visit, which means that the treatment can be adjusted immediately rather than at the subsequent infusion, which is usually six to eight weeks later [888990] (Table 3).
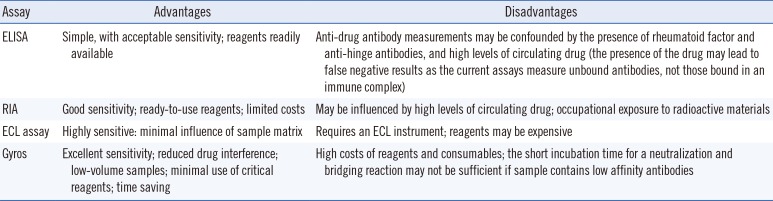
Table 3
Summary of useful antibody-detecting assays
![]()
The real prevalence of anti-drug antibodies is still unknown because differences in the specificity and sensitivity of the available assays make it very difficult to compare studies and has led to considerable variability in the published figures [9192]. However, numerous attempts have been made in the areas of standardization and harmonization, such as the production of high-quality internal quality controls to validate routine drug and anti-drug antibody assays and to reduce intra laboratory variability, and external quality control to reduce interlaboratory variability. Moreover, it is expected that biosimilars will become a significant growth driver for the pharmaceutical industry, mainly because of the current market penetration of biological agents and the need to save costs in comparison with original drugs. Nevertheless, studies validating immunogenicity assays are urgently needed to support the further development of biosimilars.
Go to :
CONCLUSIONS
This review aimed to highlight the role of laboratories in ensuring appropriate use of biological drugs, which have become increasingly important in the treatment of diseases ranging from rheumatic diseases and other chronic conditions involving various organs and systems to various types of cancer. We focused on rheumatic diseases because they represent one of the main targets of biological drugs, which are often used in combination with csDMARDs. Biological treatment is quite safe, at least in the short to medium term, but some unwanted effects are possible. A reduced immune response may lead to the onset of infections which although generally not serious, may become severe in patients with latent infections; injection-site cutaneous reactions or a vasomotor crisis may occur during intravenous infusion; and autoantibodies associated with manifestations typical of an autoimmune disease may appear.
Unlike synthetic pharmacological molecules, biological drugs are produced in cells, and their production requires such precise procedures that even a small change in any part of the process can significantly alter the molecular structure and consequently, drug efficacy and safety. Therefore, the production and distribution of biological drugs needs to be carefully controlled, bearing in mind that difficulties inherent to the production techniques increase with the complexity of the molecule. Further, as they are proteins (and as such, immunogens), they may be recognized as non-self and thus induce an immune reaction that neutralizes their effectiveness or even have more serious consequences. Many factors can influence the risk of immunogenicity: the quality of the biological drug (e.g., the possible presence of contaminants arising from the production process that may interfere with drug activity), the characteristics of the production process, the duration of treatment, the site of drug administration, and patient characteristics (e.g., the condition of the immune system, genetic profile).
Biological drugs can interfere with cytokines. Chronic inflammatory diseases are characterized by an imbalance in favor of inflammatory over anti-inflammatory cytokines, and biological drugs act by blocking the activity of the former, which are produced in large quantities by patients with RA or other chronic inflammatory diseases [9394].
Many biological drugs are currently on the market, and their different mechanisms of action and possible drug-related events may affect their tolerability, efficacy, and safety due to their differential immunomodulatory action. This is where clinical laboratories play a pivotal role.
Go to :
 XML Download
XML Download