

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Obesity, which is associated with a number of potential health risks, has become a remarkable problem worldwide. Many risk factors are associated with the occurrence of stress urinary incontinence (SUI) [12], including obesity, because it increases the pressure in the abdomen [34]. Obesity is associated with increased pressure on the pelvic floor, which results in damage to the nerves and muscle and a higher prevalence of SUI than occurs in non-obese individuals [5]. Weight has a greater impact on SUI (including mixed incontinence) than urge incontinence, and urinary incontinence improves significantly with weight loss [6].
Midurethal slings, such as retropubic tension-free vaginal tape (TVT) and transobturator tape (TOT) procedures, are the standard treatments for female SUI. However, in cases of SUI due to intrinsic sphincter deficiency (ISD), which has a low treatment rate, there is an increasing trend toward treatment with midurethral sling surgery using a new device. The readjustable midurethral sling (REMEEX system) was introduced as a new device that combines the advantages of a less-invasive approach and the opportunity of sling re-adjustment to increase the success rate and overcome the complications generally reported after the positioning of other compressive pubovaginal slings [7]. Recently, a number of authors published their experience of the REMEEX procedure for the treatment of ISD-type SUI; they achieved remarkable results in terms of cure and complication rates. However, no studies have assessed the surgical outcomes in obese patients, who have a higher prevalence of SUI and more severe symptoms. In this study, we compare the subjective and objective outcomes of overweight, obese, and non-obese patients 1 year after implantation of the REMEEX system.
Go to : 
MATERIALS AND METHODS
1. Patients
From August 2009 to August 2015, we retrospectively analysed the medical records of 104 female patients who had undergone REMEEX surgery for the treatment of SUI due to ISD or recurrent SUI in a single tertiary medical facility. The inclusion criteria were patients who had undergone REMEEX surgery and complained of SUI due to ISD or had previously undergone anti-incontinence surgery but in whom urinary incontinence had recurred. Patients who complained of previous urge incontinence symptoms, presented any pelvic organ prolapse and for whom follow-up records were missing, were excluded. A total 70 of the 104 patients were included in this study. All patients underwent history-taking, anthropometric measurements, physical examination, 1-hour pad test, uroflowmetry and urodynamic study to identify the type of urinary incontinence. Patient data were recorded in a retrospective database that was approved by Soonchunhyang University Bucheon Hospital Institutional Review Board (approval number: SCHBC 2019-03-015), and informed consent was waived because of the study design. The data were abstracted from the patient charts and entered into the database. ISD was defined as a Valsalva leak-point pressure (VLPP) <60 cm H2O or a maximal urethral closure pressure (MUCP) <20 cm H2O. Patients were divided into normal, overweight and obesity groups according to their body mass index (BMI). BMI was calculated as weight in kilograms divided by the square of height in meters; the World Health Organization (WHO) definitions of ‘overweight’ as a BMI >25 kg/m2 and ‘obesity’ as a BMI >30 kg/m2 were employed.
2. Surgical technique
The REMEEX system consists of a suburethral polypropylene prosthesis (35×12 mm) that is connected to a pressure-adjusting device (varitensor) by two traction threads. The patient was placed in the dorsal lithotomy position under general anaesthesia and an 18-Fr. Foley catheter was inserted. A 4-cm abdominal transverse incision was made at the midline, two fingers above the pubic symphysis, the fat was dissected, and the fascia of the anterior rectal abdominal muscles was exposed. Traction threads were implanted in the abdominal site through the anterior vaginal wall at the midurethral level. Subsequently, the bladder integrity was evaluated by cystoscopy. After determining that the bladder was intact, the threads were connected to the varitensor and the manipulator was turned clockwise until it was positioned approximately two fingers' distance over the rectus fascia (Figs. 1, 2). When the varitensor was positioned at its proper location, the surgeon sutured the opening site but kept the incision area open where the manipulator was connected. This approach allowed the manipulator to remain perpendicular to the skin. The day after surgery, 250 mL of saline was injected into the bladder, the urethral catheter was removed and the patient was instructed to perform a Valsalva manoeuver and cough while standing. If a leak was still observed, two clockwise turns were made twice a day on the manipulator until continence was reached (Fig. 3). The patient was subsequently instructed to void urine in the toilet and the residual urine volume was determined using a portable sonar. If the residual urine volume was <100 mL, the manipulator could be disconnected from the varitensor. However, if the residual urine volume was >100 mL, the manipulator was turned anti-clockwise to decrease the sling support. The varitensor stayed implanted above the rectus fascia as a permanent regulation mechanism that could be used to readjust the sling during follow-up care as needed.
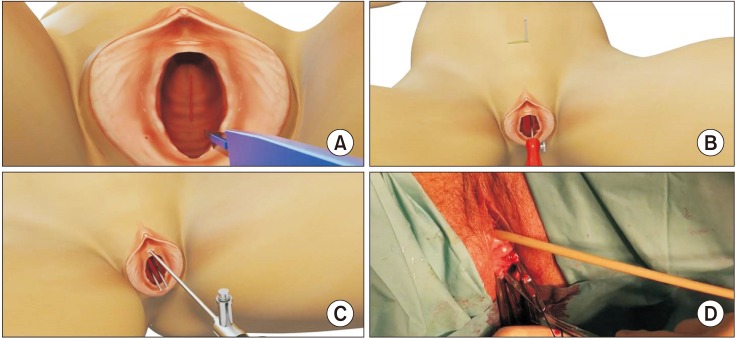 | Fig. 1(A) Make an incision in the anterior vaginal wall at the mid-urethral level. (B) Insert the two needles through the vaginal incision until reaching the abdominal site. (C) Check the bladder integrity by means of a cystoscopy. (D) Connect the traction threads to the needles. Images from Neomedic International.
|
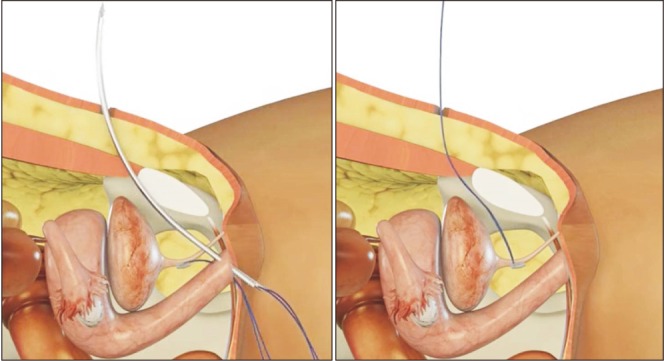 | Fig. 2Traction threads were implanted in the abdominal site through the anterior vaginal wall at the midurethral level (sagittal view). Images from Neomedic International.
|
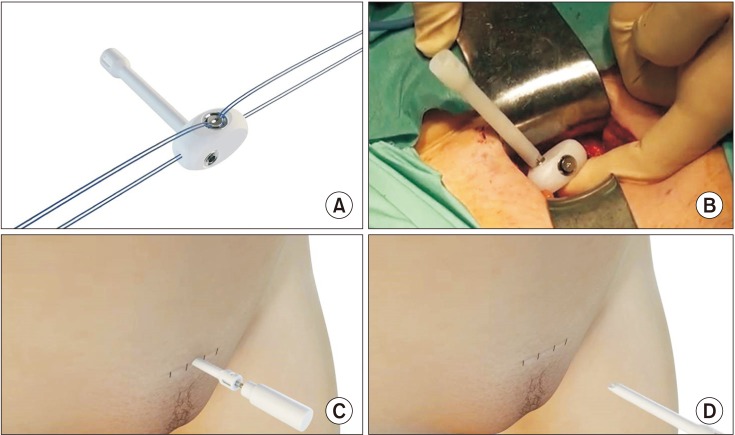 | Fig. 3(A) Passing traction threads through lateral holes of the varitensor. (B) Turning of the varitensor clockwise so it rests tension free on the fascia of rectus abdominis muscles. (C) Adjusting the device by turning the manipulator. (D) Manipulator disconnector. Images from Neomedic International.
|
3. Postoperative evaluations
Postoperative follow-up visits occurred at 1, 3, and 12 months after surgery. Objective patient outcomes were determined according to the results of 1-hour pad tests performed 3 months after surgery as follows: <2 g of urine leakage was considered a ‘cure’, 2 to 50 g of urine leakage was considered an ‘improvement’ and >50 g of urine leakage was considered ‘failure’. Patients completed a severity index for urinary incontinence at 3 months and 1 year after surgery, and the results were defined as follows: a state in which no urinary incontinence was present was defined as ‘cured’, a state in which incontinence symptoms were very rare and inconspicuous or the patient was satisfied with the surgical outcome was ‘improvement’. The presence of severe urinary incontinence after surgery or a patient complaining of dissatisfaction with the outcome of the surgery was defined as ‘failure’ [8].
The success rate was defined as the sum of the cure and improvement rates. The subjective satisfaction of the patients was determined by selecting one of the five levels of the Likert scale (very satisfied, satisfied, neither satisfied nor unsatisfied, unsatisfied and very unsatisfied) at 1-year follow-up.
4. Postoperative complications
We reviewed the medical record of the patients to investigate the intraoperative and postoperative complications. All complications were classified according to the modified Clavien complication classification system.
5. Statistical analysis
The baseline characteristics and postoperative outcomes were compared according to body weight. The frequencies and proportions of each categorical variable were compared using chi-square test or Fisher's exact tests, as appropriate. For continuous variables, means and standard deviations were compared using one-way analysis of variance (ANOVA) after normality and variance-equivalence tests. For abnormally-distributed continuous variables, median values and interquartile ranges were compared using Kruskal-Wallis tests. All statistical tests were conducted at a two-sided significance level of 0.05 using R (version 3.1.3; The R Foundation for Statistical Computing, Vienna, Austria).
Go to :
RESULTS
Of the 104 patients who underwent REMEEX surgery, 70 patients who were followed up for 1 year were included in this study. Of these, 64 (91.4%) were diagnosed with SUI due to ISD and 6 (8.6%) had recurrence after undergoing midurethral anti-incontinent surgery. There were 26 normal weight women, 31 overweight women, and 13 obese women. The baseline characteristics of the patients are summarised in Table 1. The mean BMIs of patients in the normal, overweight, and obese groups were 23.0±1.5 kg/m2, 27.1±1.2 kg/m2 and 31.9±1.9 kg/m2, respectively. A comparison of the characteristics among groups found no statistically significant differences in age, gravidity, parity, obstetrical history and the presence of menstruation (p>0.05).
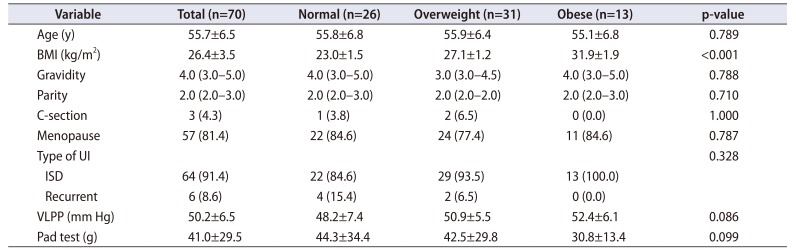
Table 1
Baseline characteristics according to body weight
Values are presented as mean±standard deviation, median (interquartile range) for continuous variables, or number (%) for categorical variables.
BMI, body mass index; UI, urinary incontinence; ISD, intrinsic sphincter deficiency; VLPP, Valsalva leak-point pressure.
p-values were calculated using one-way ANOVA or Kruskal-Wallis tests for continuous variables and chi-square or Fisher's exact tests for categorical variables, as appropriate.
![]()
The mean VLPP value in preoperative urodynamic study was 48.2±7.4 mm Hg in the normal weight group, 50.9±5.5 mm Hg in the overweight group and 52.4±6.1 mm Hg in the obese group. The mean results of the 1-hour pad test were 44.3±34.4 g in the normal weight group, 42.5±29.8 g in the overweight group and 30.8±13.4 g in the obese group. There was no significant difference in the results of the preoperative VLPP and 1-hour pad test among groups. (p=0.086 and 0.099, respectively).
Table 2 shows the clinical outcomes of the REMEEX procedure. The results of the 1-hour pad tests performed 3 months after surgery, which were considered the objective outcome, revealed that urine leakage was 2.6±2.5 g in the normal weight group, 1.8±1.8 g in the overweight group and 1.5±1.7 g in the obese group (p=0.331). The objective cure rate according to the 1-hour pad test was 11 patients (42.3%) cured and 15 (57.7%) improved in the normal weight group, 16 (51.6%) cured and 15 (48.4%) improved in the overweight group. Six (46.2%) cured and 7 (53.8%) improved in the obese group (p=0.78). No patients in any group sustained >50 g urine leakage. The success rate (the sum of cure and improvement) at 3 months after surgery was 100% in all groups. However, the 1-year postoperative, success rate was 91.5% in the normal weight group, 93.5% in the overweight group and 92.3% in the obese group. All groups exhibited similar success rates. A total of 84.7%, 77.4%, and 77.0% of normal weight, overweight and obese women were very satisfied or satisfied 1 year after surgery. Conversely, 15.4% of the normal weight group, 22.6% of the overweight group and 23.1% of the obese group were ‘neither satisfied nor unsatisfied’, ‘unsatisfied’ or ‘very unsatisfied’ 1 year after surgery. Patient satisfaction was not significantly different among the BMI groups (p=0.948).
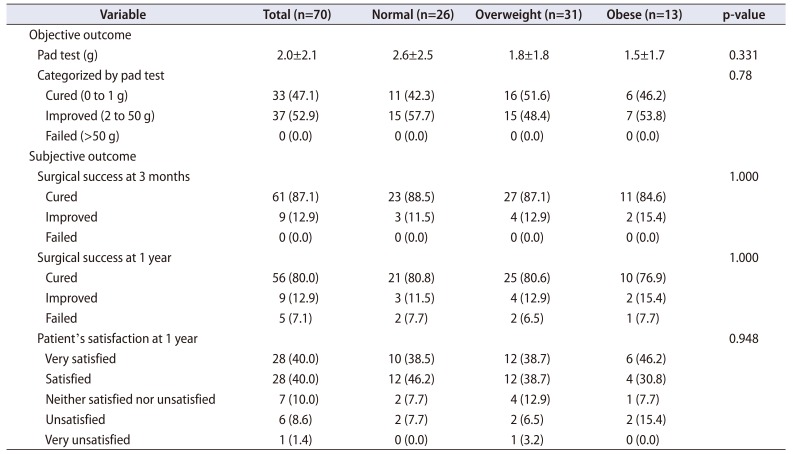
Table 2
Postoperative outcome after REMEEX according to body weight
![]()
In our study, a total of 34 cases of complications occurred in 26 patients (37.1%). According to the modified Clavien system, 19 complications (27.1%) were classified with grade I complications, 4 complications (5.7%) were classified as grade II, and 11 complications (15.7%) were classified with grade III (Table 3). Three bladder perforation (4.3%) were observed during surgery and were solved by reinsertion of trocar immediately. There were 6 hematomas (8.6%), which were managed by conservative treatment without additional intervention. In the Foley catheter removal on the day after surgery, acute urinary retention occurred in 5 patients (7.1%). Three of these patients were resolved naturally, but two patients had early read-justment on the second day of operation. Five patients (7.1%) experienced de novo urgency, requiring treatment with anticholinergic drugs. None of the patients complained of recurrence of urinary incontinence until 3 months postoperatively. However, 11 patients (15.7%) complained of recurrence of urinary incontinence during follow-up, and these patients required delayed sling readjustment under local anesthesia. Fortunately, none of the patients in our study needed removal of the remex system due to the occurrence of surgical site infection. There was no need for statistical analysis because of the small number of complications.
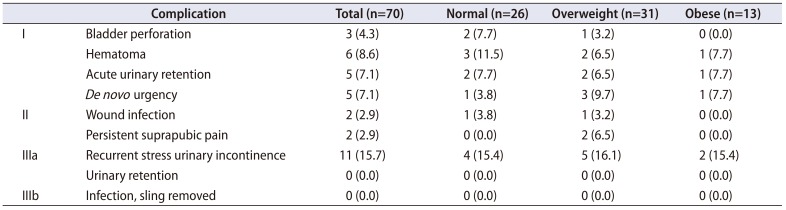
Table 3
Postoperative complications
![]()
Go to :
DISCUSSION
Since the first description of TVT as a modified sling surgery method by Ulmsten et al. [9] in 1996, many reports have been published on the effects of mid-urethral tape surgery. In a multi-centre study by Ulmsten et al. [10], who reported more than 1 year follow-up data from patients undergoing mid-urethral sling tape surgery, 91% of patients were cured and 7% of patients had improved. In 2001, Delorme [11] described an alternative approach using TOT to avoid major complications. The cure rates achieved with TVT and TOT procedures were similar, ranging from 90% to 95% [12]. Thus, midurethral sling surgery is widely used as a standard treatment for stress incontinence in women; it is simple to perform, yields a high treatment success rate, low complication rate and is highly cost-effective.
Clinically, women with ISD have more severe incontinence and a lower surgical success rate than do women with stress incontinence and normal urethral function [13]. In addition, the surgical failure rates increase four- to six-fold when there is evidence of ISD [14]. The United States and European guidelines recommend urethral bulking agents, suburethral slings and artificial urethral sphincters for the treatment of SUI with ISD [1516]. In cases of SUI caused by ISD, most tension-free anti-incontinence devices have low or ineffective therapeutic efficacy, and fixed urethra ISD has a very lower therapeutic efficacy and the highest failure rate [1718].
Many studies have revealed that SUI due to ISD is challenging for many urologists because of the relatively low success rate of treatment. Recently, middle urethral sling operations using the REMEEX system were performed for the treatment of SUI due to ISD. With the REMEEX system, the operator can immediately adjust the urethral sling tension and also perform delayed readjustments in cases of treatment failure to achieve a lower rate of complications. Reports of the surgical outcomes and complications of the REMEEX procedure have recently been published. Moreno Sierra et al. [19] followed a group of 683 women with mixed incontinence (30.2%), ISD (73.1%) and recurrent SUI (35.7%) who underwent the REMEEX procedure for a mean of 23 months (range, 6–93 months). The authors reported that the cure rate was 92.2%, with 6.9% reporting improvement and 0.9% reporting failure. Eighty patients (11.7%) underwent readjustment between 6 and 8 months after surgery. Errando et al. [20] prospectively reported a mean follow-up of 38 months in 125 patients with SUI because of ISD (55/125, 44.0%) and recurrent SUI (70/125, 56.0%) who underwent REMEEX surgery. The pad test results revealed that 87% of the patients were cured, 6% needed re-adjustment and 7% needed re-adjustment but refused the procedure because they were satisfied with the operation. Giberti et al. [21] used the REMEEX system on 30 patients with SUI and ISD for a mean of 60.6 months (range, 22–96 months). They reported that 26 (86.7%) patients were cured, 2 (6.7%) had improved, and 2 (6.7%) had failed treatment. Two patients (6.7%) required sling tension readjustment. Park et al. [22] reported the surgical outcomes obtained using the REMEEX system (mean follow-up, 27.6 months; range, 14–56 months). They reported that the cure, improvement and failure rates were 89.2% (91/102 patients), 5.9% (6/102) and 4.9% (5/102), respectively. In addition, 80.0% of patients were very satisfied or satisfied with the operation results at the 1-year follow-up. In addition, recent published research results are summarized in Table 4 [19202122232425]. In the current study, the short-term results of 70 patients with SUI (64 cases of SUI due to ISD and 6 recurrent SUI cases) who underwent REMEEX surgery revealed a subjective cure rate of 92.9% and an objective cure rate of 100%.
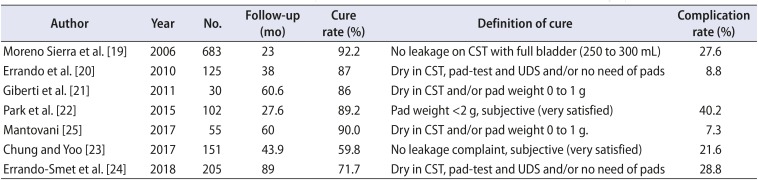
Table 4
Comparison of the published series of female urinary incontinence patients who underwent the Remeex surgery
| Author | Year | No. | Follow-up (mo) | Cure rate (%) | Definition of cure | Complication rate (%) |
|---|---|---|---|---|---|---|
| Moreno Sierra et al. [19] | 2006 | 683 | 23 | 92.2 | No leakage on CST with full bladder (250 to 300 mL) | 27.6 |
| Errando et al. [20] | 2010 | 125 | 38 | 87 | Dry in CST, pad-test and UDS and/or no need of pads | 8.8 |
| Giberti et al. [21] | 2011 | 30 | 60.6 | 86 | Dry in CST and/or pad weight 0 to 1 g | |
| Park et al. [22] | 2015 | 102 | 27.6 | 89.2 | Pad weight <2 g, subjective (very satisfied) | 40.2 |
| Mantovani [25] | 2017 | 55 | 60 | 90.0 | Dry in CST and/or pad weight 0 to 1 g. | 7.3 |
| Chung and Yoo [23] | 2017 | 151 | 43.9 | 59.8 | No leakage complaint, subjective (very satisfied) | 21.6 |
| Errando-Smet et al. [24] | 2018 | 205 | 89 | 71.7 | Dry in CST, pad-test and UDS and/or no need of pads | 28.8 |
![]()
Obesity is an independent risk factor for the development of SUI; however, its mechanism is unclear. In a study of 2,589 women aged 30 to 59 years, Mommsen and Foldspang [4] reported that BMI was positively correlated with urinary incontinence, independently of other risk factors, especially SUI. Higher intrabdominal pressures have been observed in patients with a greater BMI, with a mean 4.9 mm Hg pressure observed in non-obese patients compared with 8.9 mm Hg in morbidly obese patients [26]. The increased abdominal pressure in obese patients is thought to contribute to the development of SUI by increasing the bladder pressure, increasing the pressure at maximum bladder capacity, decreasing the pressure transmission from the bladder to the urethra when coughing and reducing VLPP [3262728]. Obesity-induced neurogenic effects on the pelvic floor may also contribute to urethral dysfunction and the resulting UI [3].
There is concern that even if the midurethral sling is highly effective for the treatment of SUI, its efficacy may be reduced in overweight or obese patients. Killingsworth et al. [29] reported the results of patients who underwent TVT (195 patients; 68 normal weight, 65 overweight, and 62 obese). At the 1-year fullow-up, 18%, 14%, and 19% of patients in the obese, overweight and normal weight groups experienced SUI symptoms, respectively; there were no statistically significant differences among groups. More recently, Brennand et al. [30] reported the results of a randomized controlled study that evaluated the effects of BMI on the objective and subjective cure rate for 12 months after midurethral sling surgery. Sixty-one obese and 121 normal weight patients were enrolled. The objective and subjective cure rates were lower in the obesity group than in the normal weight group (67.8% vs. 85.6%, p=0.006 and 70.7% vs. 85.8%, p=0.016; respectively). However, there was no difference in the quality of life, as assessed using validated questionnaires, between the two groups [30]. Therefore, the results of midurethral sling operations in obese patients have been well documented, but the results are controversial because they differ from study to study.
To our knowledge, no studies have compared the surgical outcomes of midurethral sling surgery using the REMEEX system according to BMI. In the current study, there were no differences in surgical outcome using the REMEEX system in patients with ISD-type SUI or recurrent SUI according to BMI; there was also no difference in patient satisfaction.
The current study does have some limitations. First, it was not a prospective controlled trial. However, we did rely on prospective data collected for a clinical database using standardized surgical protocols. This allowed us to ensure that all women had the same perioperative and follow-up assessments, which, in our opinion, strengthens the outcome of the analysis despite the retrospective design. Second, this study includes only short-term follow-up data. Although there were no differences among groups at 1-year after surgery, the overweight and obese patients have consistently high pressure in the pelvic area, which suggests that the long-term success rate might decrease. Therefore, later studies on the long-term results are needed.
Go to :
CONCLUSIONS
The current study demonstrated that the REMEEX procedure achieves similar outcomes in women with ISD or recurrent SUI, regardless of obesity. Both obese and non-obese women had sustained cure rates at the 1-year follow-up and were satisfied with the outcome. We conclude then that REMEEX seems to be an effective and safe procedure for stress incontinence, regardless of BMI. Nevertheless, long-term follow-up results should also be obtained.
Go to :
 XML Download
XML Download