

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A standard 10- to 12-core transrectal ultrasound (TRUS)-guided biopsy is the most commonly used diagnostic modality for the detection of prostate cancer (PCa) [12]. However, there is a chance of undetected PCa, and even high-grade PCa, in some males with a previous negative result on TRUS-guided biopsy. In addition, although active surveillance (AS) has emerged as a treatment strategy in males with low-risk and very-low-risk PCa [345], TRUS-guided biopsy can miss high-grade or high-volume PCa and is not suitable for AS because of undersampling in the anterior prostate [67]. As a result, a sizeable minority of males initially classified as having low-risk or very-low-risk PCa ultimately receive definite treatment including radical prostatectomy (RP) or progress to metastatic disease and die from PCa [589]. Consequently, TRUS-guided biopsy alone is not sufficient, and a more reliable diagnostic modality that accurately categorizes risk stratification is needed.
Transperineal template-guided saturation prostate biopsy (TPB) is an alternative diagnostic modality for sampling prostate tissues. TPB has the advantage of being able to make a reliable approach to the entire prostate gland, including the anterior prostate and the transitional zone [10]. In addition, because TPB is usually conducted under general anesthesia, during which the prostate is not mobilized, a larger number of cores are obtained while confirming each biopsy position in three dimensions [61112]. Therefore, the outcomes of TPB more precisely reflect subsequent pathologic results of RP, as opposed to those from TRUS-guided biopsy [1314]. However, the clinical implications of TPB in patients with negative results on TRUS-guided biopsy or in those who were candidates for AS have not been fully investigated.
AS for localized PCa requires more precise risk stratification, and detection of missed PCa in patients with negative results on TRUS-guided biopsy is crucial to provide effective treatment options and to predict prognosis. Therefore, in this study, we investigated the clinical utility of TPB for risk stratification after TRUS-guided biopsy in patients with negative results on TRUS-guided biopsy or who were candidates for AS.
Go to : 
MATERIALS AND METHODS
1. Study population
This study was approved by the Institutional Review Board of Samsung Medical Center (approval number: 2018-05-192) and was performed in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived owing to the study design. We retrospectively reviewed a database of 155 consecutive male patients who underwent TPB between May 2017 and November 2018. The indications for TPB were as follows: 1) a persistent suspicion of PCa with rising prostate-specific antigen (PSA) despite a negative result on TRUS-guided biopsy (n=58) or 2) a confirmed or scheduled biopsy in male candidates for AS after TRUS-guided biopsy (n=97). The eligibility criteria for AS were biopsy Gleason grade 6 (3+3), PSA ≤10 ng/mL, clinical stage T1c/T2, PSA density (PSAD) <0.2 ng/mL/cm3, two or fewer positive cores (n=89) [8], and Gleason grade ≤7 (3+4) (n=8). Multiparametric magnetic resonance imaging (mpMRI) was performed in 133 patients before TPB and was scored by using the Prostate Imaging Reporting and Data System version 2 (PI-RADSv2), except in one patient because of the poor quality of the images obtained.
2. Data collection
The clinical, laboratory, and pathologic data of the male patients, including age, PSA, prostate volume, PSAD, number of total and positive cores, and Gleason grade, were reviewed from the electronic medical records of our database. Gleason grade of TRUS-guided biopsy and TPB were examined by the same pathologist who specialized in genitourinary cancer. After TPB, the bilaterality of PCa was examined, and upgrading of Gleason grade was defined as an increase from Gleason grade 6 at TRUS-guided biopsy to Gleason grade 7 (3+4) or greater after TPB. Clinically significant cancer (CSC) was defined as PCa with Gleason grade 7 (3+4) or greater.
3. MRI protocol and interpretation
mpMRI was performed by using a 3.0 T MRI instrument (Intera Achieva TX; Philips Healthcare, Best, The Netherlands) with a six-channel, phase-array body coil. The protocols for mpMRI were based on the European Society of Urogenital Radiology guidelines [15] and included T1-weighted, T2-weighted, and diffusion-weighted imaging with b values of 0, 100, and 1,000 s/mm2, and dynamic contrast-enhanced imaging after intravenous injection of gadolinium diethylenetriamine pentaacetic acid (Gadovist; Schering, Berlin, Germany).
The MR images were loaded by using a picture archiving and communication system (Centricity; GE Healthcare, Barrington, IL, USA) and were reviewed by a radiologist with more than 10 years of experience in prostate MRI interpretation who was blind to the clinical and pathologic information. The reviewer scored an index lesion with PI-RADSv2 by using a 5-point scale in each patient. PI-RADSv2 assessment categories were defined as follows: score 1, clinically significant cancer is highly unlikely to be present; score 2, clinically significant cancer is unlikely to be present; score 3, the presence of clinically significant cancer is equivocal; score 4, clinically significant cancer is likely to be present; and score 5, clinically significant cancer is highly likely to be present [10].
4. TPB technique
Prior to TPB, a blood test for prothrombin time and activated partial thromboplastic time was examined to evaluate the coagulation profile. Patients were asked to stop oral anticoagulants for 1 week before the biopsy. All biopsies were performed on an inpatient procedure. Patients received Yal solution (docusate sodium 10 mg) and a bisacodyl suppository as a rectal preparation. For prophylactic treatment, oral cephalosporin and/or quinolone was given for 1 week from the day before the biopsy, and aminoglycoside (amikacin 500 mg) was administered intramuscularly a few minutes before biopsy.
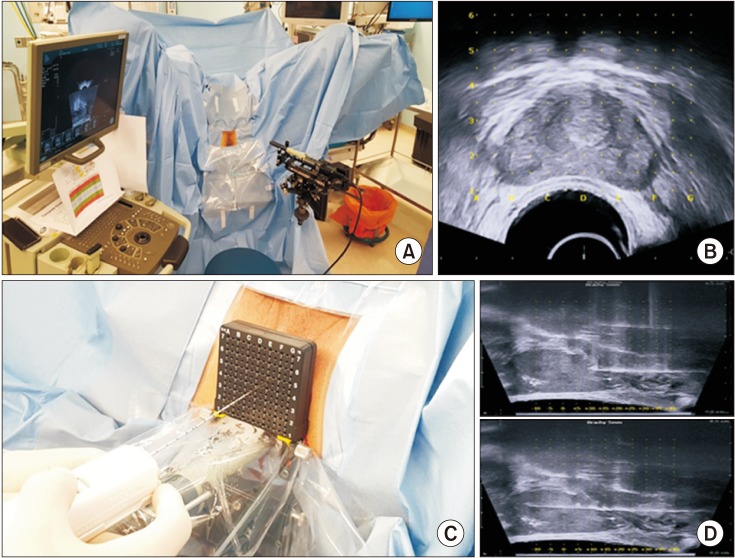
TPB was performed with the patients under general anesthesia to immobilize the prostate during the procedure. Patients were repositioned to an extended lithotomy position (Fig. 1A), and a Foley catheter was inserted. A digital rectal examination was performed. Then, TPB was performed using a biplanar TRUS 8848 brachytherapy probe (BK Medical, Herlev, Denmark) covered with a water-filled brachytherapy balloon and Classic STEPPER™ device (CIVCO, Kalona, IA, USA) (Fig. 1B). Systemic biopsies were collected through the perineum using an 18-G, 20-cm long biopsy needle (ACECUT; TSK Laboratory, Tochigi, Japan) via a standard brachytherapy grid at 5-mm intervals, from the medial to the lateral plane in the anterior, mid, and posterior sectors (Fig. 1C), which were divided into right and left sides [1617]. Depending on the distance from the prostate apex to the base, a single longitudinal biopsy was performed when the prostate length was less than 2 cm, whereas double longitudinal biopsies were conducted when the length was more than 2 cm (Fig. 1D). As such, the number of biopsy cores obtained was directly dependent on the size of the prostate. The patients were discharged the morning after the procedure, after confirmation that they could pass urine.
5. Statistical analysis
Quantitative variables are presented as medians (range) or means±standard deviation, and qualitative variables are presented as absolute values (percentage). Descriptive statistics were obtained for demographic variables. All statistical analyses were performed by using IBM SPSS for Windows, version 23.0 (IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
The baseline demographics and characteristics of the 155 patients who underwent TPB are summarized in Table 1. The patients' median (range) age at TPB was 65.0 (47.0–79.0) years. Median PSA and prostate volumes were 5.74 (0.56–42.76) ng/mL and 41.0 (12.3–233.0) cm3, respectively. Of the 97 candidates for AS, Gleason grade in TRUS-guided biopsy was 6 (3+3) in 89 patients (91.8%) and 7 (3+4) in 8 patients (8.2%).
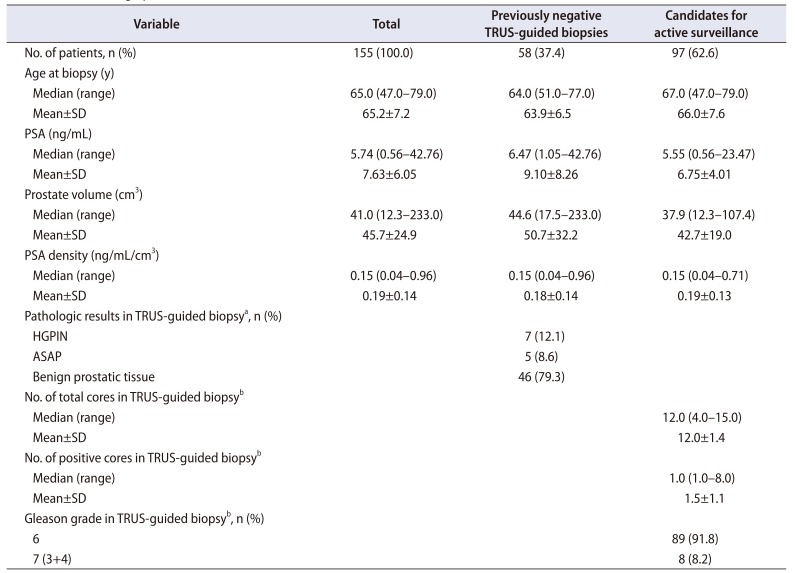
Table 1
Patient demographics and characteristics at baseline
![]()
The results of TPB are presented in Table 2. The median (range) duration of TPB was 25 (15.0–40.0) minutes. The median (range) number of TPB cores was 36.0 (13.0–40.0), and PCa was identified in 85 patients (54.8%) overall. Of the 58 males with a previous negative result on TRUS-guided biopsy, PCa was detected in 17 (29.3%), including 8 with CSC. Of the 97 candidates for AS, PCa was detected in 68 (70.1%); overall, the Gleason grade of 31 patients (32.0%) was upgraded after TPB, including 20 with Gleason grade 7 (3+4), 6 with Gleason grade 7 (4+3), and 5 with Gleason grade 8 (4+4). In addition, a total of 40 patients (41.2%) were diagnosed with bilateral PCa.
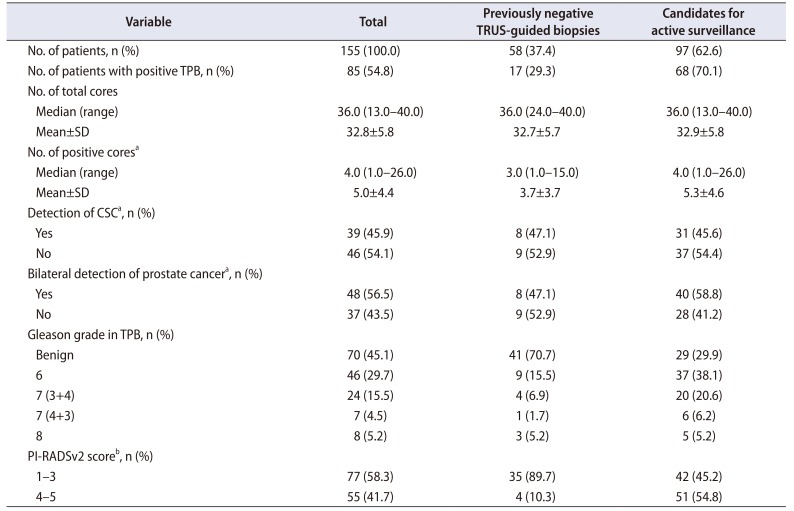
Table 2
Results of transperineal template-guided saturation prostate biopsies and PI-RADSv2 scores
![]()
The total complication rate after TPB was 16.8% (26/155), including acute urinary retention (12.3%, 19/155) that required temporary Foley catheter indwelling, post-voiding residual urine (0.6%, 1/155) that required clean intermittent catheterization, gross hematuria (3.2%, 5/155) with overnight bladder irrigation, and hematospermia (0.6%, 1/155). There were no Clavien–Dindo grade 3 to 5 complications, such as transfusion, acute prostatitis, or readmission.
Pathologic correlation between TPB and RP specimens is summarized in Table 3. After TPB, a total of 30 patients underwent RP, and upgrading of Gleason grade was identified in 5 patients (16.7%). However, 20 patients (66.7%) showed the same Gleason grade of TPB after RP.
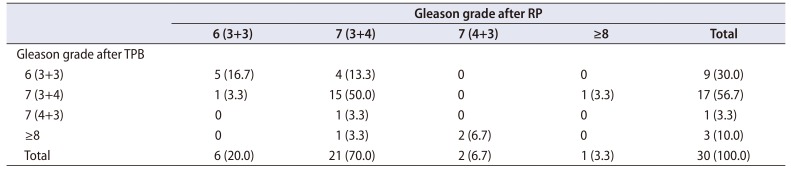
Table 3
Comparison of Gleason grade after transperineal template-guided saturation prostate biopsy and pathologic results after radical prostatectomy
![]()
The outcomes of TPB stratified by PI-RADSv2 score in mpMRI are depicted in Fig. 2. Of the 39 patients with a previously negative result on TRUS-guided biopsy, a PI-RADSv2 score of 1 to 3 was given in 35 (89.7%), and PCa was detected in 7 (20.0%), including 3 with a Gleason grade of 7 (3+4). Of the remaining 4 patients with a PI-RADSv2 score of 4 to 5, PCa was found in 3 (75.0%), and one had Gleason grade 8 (4+4). Of the 85 candidates for AS with Gleason grade 6 (3+3), a PI-RADSv2 score of 1 to 3 was identified in 38 (44.7%), in whom PCa was detected in 20 (52.6%), including 11 (28.9%) who were upgraded to Gleason grade 7 (3+4) or greater. When the PI-RADSv2 score was 4 to 5, 38 patients (80.9%) were diagnosed with PCa, of whom 15 (31.9%) were upgraded to Gleason grade 7 (3+4) or greater after TPB.
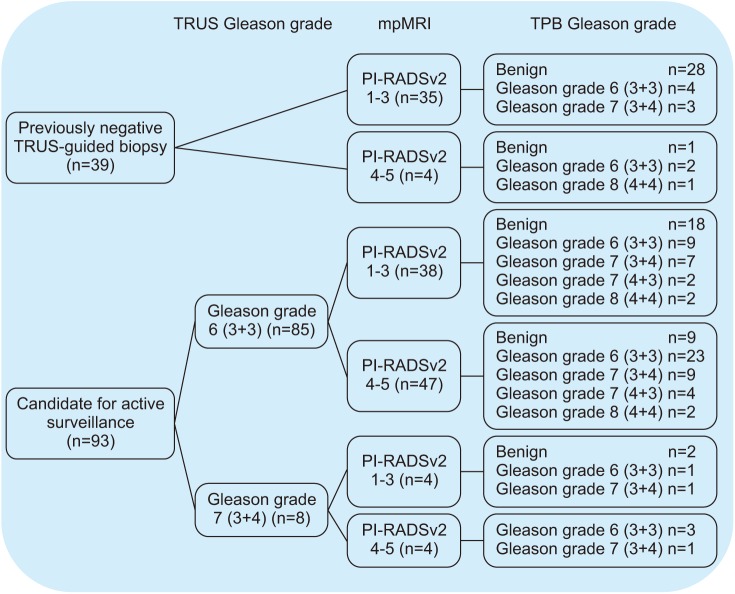 | Fig. 2Association between Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) score and results of transperineal template-guided saturation prostate biopsy (TPB) in males with a previous negative result on transrectal ultrasound (TRUS)-guided biopsy or who were candidates for active surveillance. mpMRI, multiparametric magnetic resonance imaging.
|
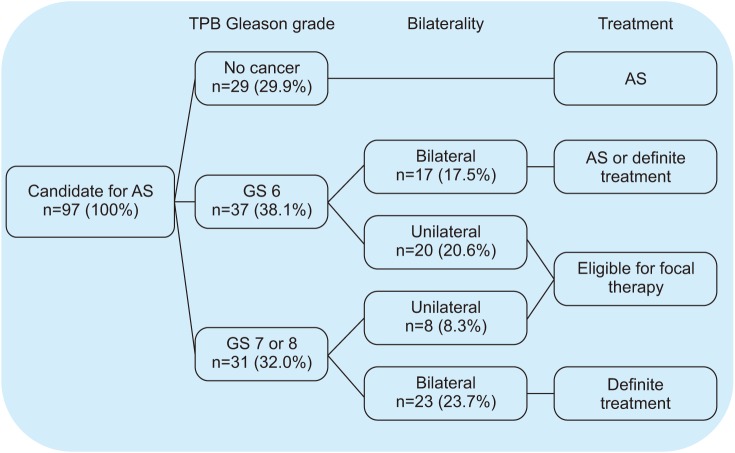
The treatment strategy in patients who were candidates for AS according to the results of TPB is shown in Fig. 3. Of the total 97 patients, 29 (29.9%) with benign pathology at TPB remained on AS. Of the 37 (38.1%) with Gleason grade 6 (3+3), AS or definite treatment including RP could be considered when cancer was identified bilaterally (n=17, 17.5%), whereas focal therapy was considered if cancer was confirmed unilaterally (n=20, 20.6%). Of the remaining 31 males (32.0%) with Gleason grade 7 or 8, definite treatment was required. However, when an indication for focal therapy was expanded to males with a unilaterally identified Gleason grade of 7 (3+4), 8 additional males (8.3%) were included, and 28 (28.9%) were eligible for focal therapy overall.
Go to :
DISCUSSION
In this study, of the 58 patients with negative results on TRUS-guided biopsy, PCa was identified in 17 (29.3%), including 8 with Gleason grade 7 (3+4) or greater. In addition, of the 97 candidates for AS, an upgraded Gleason grade was identified in 31 (32.0%). Furthermore, in 28 patients (28.9%) with unilaterally identified PCa with Gleason grade 6 (3+3) or 7 (3+4), focal therapy could be considered. These results suggest that TPB can classify the risk of PCa previously missed or underdiagnosed by TRUS-guided biopsy. Therefore, TPB can be used as a diagnostic tool to determine risk stratification of PCa and can be used to help counsel patients with regard to treatment strategy. To the best of our knowledge, this is the first study to analyze the clinical utility of TPB for risk stratification after TRUS-guided biopsy in Korean males.
The widespread use of PSA screening for PCa has led to the detection of low-risk and very-low-risk PCa, and these patients are eligible for various treatment options other than RP, including AS or focal therapy [18]. However, approximately one-third of males on AS ultimately have experienced delayed treatment within the first few years [6], and misclassification at diagnosis was the most likely cause of treatment failure rather than disease progression [1119]. Therefore, accurate diagnosis of PCa is essential for optimal patient selection, and a more dedicated biopsy strategy to compensate for the insufficiency of existing diagnostic tools is required.
In our study, PCa was identified in 17 patients (29.3%), including 8 with CSC, after TPB in 58 patients with a previous negative result on TRUS-guided biopsy. There is no consensus for repeat biopsy strategies after an initial negative result. In a study by Nafie et al. [20], 42 patients with previous negative results on TRUS-guided biopsy underwent simultaneous 12-core TRUS and 36-core perineal biopsy. In that study, TPB showed a significantly higher PCa detection rate than did TRUS-guided biopsy (45% vs. 15%, p=0.01). However, that meta-analysis study, which included 12 studies of TRUS-guided biopsy and 14 studies of TPB as a repeat biopsy strategy, reported that cancer detection rates were 30.0% and 36.8% for TRUS-guided biopsy and TPB, respectively [21].
In addition, several studies that have analyzed the role of TPB for risk stratification after TRUS-guided biopsy in patients for AS are summarized in Table 4 [611121622232425]. Of the eight recently published studies, a commonly reported significant rate for tumor upgrading after TPB ranged from 29.2% to 41.7% [611121622232425]. In our study, 32.0% of patients (31/97) were upgraded after TPB, and the median TPB core density (a ratio of the number of biopsy cores to prostate volume) was 0.88 cores/cm3, which suggests that the prostate was comprehensively sampled. Although the results of our study agreed with those of previous studies, our rate of upgrading was on the lower end of the spectrum because the criteria for eligibility for AS were more rigorous than in other studies. In a study by Voss et al. [11], a total of 208 patients (Gleason score ≤3+4=7, PSA ≤15 ng/mL, T1–T2, and ≤50% positive cores) enrolled in AS underwent TPB, and 39.9% (83/208) were upgraded. However, when restricted to the most strict Epstein criteria [26], the rate of upgrading decreased to 29.0%, which is similar to our results. Taking all these results into account, TPB could be considered in patients with suspected PCa due to persistent elevation of PSA after a negative result on TRUS-guided biopsy or in candidates for AS for risk confirmation after TRUS-guided biopsy.
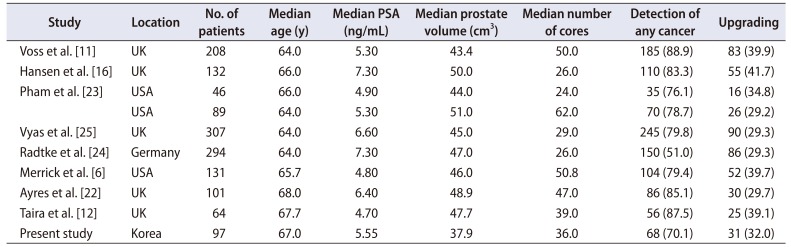
Table 4
Comparison of results from studies evaluating the role of transperineal template-guided saturation prostate biopsies in active surveillance
| Study | Location | No. of patients | Median age (y) | Median PSA (ng/mL) | Median prostate volume (cm3) | Median number of cores | Detection of any cancer | Upgrading |
|---|---|---|---|---|---|---|---|---|
| Voss et al. [11] | UK | 208 | 64.0 | 5.30 | 43.4 | 50.0 | 185 (88.9) | 83 (39.9) |
| Hansen et al. [16] | UK | 132 | 66.0 | 7.30 | 50.0 | 26.0 | 110 (83.3) | 55 (41.7) |
| Pham et al. [23] | USA | 46 | 66.0 | 4.90 | 44.0 | 24.0 | 35 (76.1) | 16 (34.8) |
| USA | 89 | 64.0 | 5.30 | 51.0 | 62.0 | 70 (78.7) | 26 (29.2) | |
| Vyas et al. [25] | UK | 307 | 64.0 | 6.60 | 45.0 | 29.0 | 245 (79.8) | 90 (29.3) |
| Radtke et al. [24] | Germany | 294 | 64.0 | 7.30 | 47.0 | 26.0 | 150 (51.0) | 86 (29.3) |
| Merrick et al. [6] | USA | 131 | 65.7 | 4.80 | 46.0 | 50.8 | 104 (79.4) | 52 (39.7) |
| Ayres et al. [22] | UK | 101 | 68.0 | 6.40 | 48.9 | 47.0 | 86 (85.1) | 30 (29.7) |
| Taira et al. [12] | UK | 64 | 67.7 | 4.70 | 47.7 | 39.0 | 56 (87.5) | 25 (39.1) |
| Present study | Korea | 97 | 67.0 | 5.55 | 37.9 | 36.0 | 68 (70.1) | 31 (32.0) |
![]()
Recently, mpMRI scored with PI-RADSv2 has emerged as a promising modality in the diagnosis of PCa, and PI-RADSv2 scores of 4 to 5 were found to increase the predictive accuracy of upgrading [27]. In our study, of 55 patients with PI-RADSv2 scores of 4 to 5, PCa was confirmed in 45 (81.8%), of which 17 (37.8%) were upgraded to Gleason grade 7 (3+4) or greater at TPB. Of 45 patients with PCa, the concordance rate of location of the PCa lesion was 84.4% (38/45). However, there is a chance of missing invisible or unclear significant PCa in mpMRI. In fact, of the 77 males with a PI-RADSv2 score of 1 to 3, a total of 15 (19.5%) were identified as harboring PCa with Gleason grade 7 (3+4) or greater. Therefore, when interpreting the PI-RADSv2 score, it is necessary to consider other clinicopathologic parameters, such as PSAD, number of positive cores, and maximum percentage of cancer per core [27].
Urinary retention, which is main complication, was identified in 19 patients (12.3%) in our study. A recent systemic review reported that the occurrence of acute urinary retention was slightly higher after TPB, ranging from 1.7% to 11.1%, than after TRUS-guided biopsy (0.4%–6.0%) or MRI-guided target biopsy (0%–1.0%) [28]. However, urinary retention is usually transient and improves in most patients with the temporary placement of a Foley catheter.
Despite the potential clinical implications of our study, it had several limitations. First, our study included a relatively small number of patients, and a large, multi-institutional, and confirmatory study is warranted. However, our study was the first to evaluate the clinical utility of TPB in Korean males and provides a basis for further research. Second, we did not perform correlation analysis between the PI-RADSv2 score and TPB results for index lesions. Furthermore, we did not have final pathologic results for patients who underwent definite treatment. However, a previous study reported that TPB accurately detected true PCa after RP [14]. Finally, because we did not have data on long-term follow-up, we could not confirm whether the detection of more aggressive cancer resulted in an improvement of prognosis, such as cancer-specific survival.
Go to :
CONCLUSIONS
After TPB, 29.3% of males with negative results on TRUS-guided biopsy were diagnosed with PCa, and 32.0% of males who were candidates for AS showed upgrading of Gleason grade. Therefore, TPB stratifies the risk of PCa that was previously missed or underdiagnosed by TRUS-guided biopsy. TPB could be used as a diagnostic tool to determine risk classification and to help counsel patients with regard to treatment decisions.
Go to :
 XML Download
XML Download