

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Currently, most cases of renal cell carcinoma (RCC) are detected incidentally, as no clinically relevant biomarker is available. Patients with symptoms have often progressed to an advanced stage of the disease and thus have poor oncologic outcomes. Diagnosis of RCC typically depends on radiologic features. In some cases, invasive renal biopsy is used to differentiate renal malignancies from benign renal masses. Patients in which small renal masses are detected early are candidates for nephron-sparing procedures, which decrease the risks of chronic kidney disease and cardiovascular events [1]. The significant risk of poor outcomes in patients with delayed diagnosis of RCC suggests that a reliable biomarker is urgently needed.
Hypoxia-inducible factor (HIF) is a key regulator of pathogenesis in RCC. HIF regulates at least 500 to 1,000 genes involved in angiogenesis, glucose metabolism, stimulation of growth factors, and cell cycle control [23]. Although the stability of the HIF expression in most RCC cells is enhanced due to the inactivation of the von Hippel–Lindau (VHL) gene, HIF is rapidly degraded in normal cells via proteasomal degradation [4]. Prolyl hydroxylase (PHD) plays a role in the HIF degradation process via oxygen-dependent hydroxylation [5]. The PHD family enzymes (PHD1–3) share a conserved C-terminal hydroxylase domain, but each PHD isoform differs in function and tissue-specific expression pattern [6]. PHD3 reportedly plays a role in several types of cancer [78]. Previous studies have shown that PHD3 is overexpressed in RCC, suggesting that PHD3 might serve as a biomarker of this disease [91011]. In the present study, we examined the serum levels of PHD3 in a prospectively enrolled cohort including both RCC patients and healthy controls. We aimed to assess the suitability of serum PHD3 as a diagnostic or surveillance biomarker of RCC.
Go to : 
MATERIALS AND METHODS
1. Study participants
Between October 2013 and March 2015, we prospectively recruited participants after obtaining approval from the Institutional Review Board of Severance Hospital (IRB no. 4-2013-0166). Informed consent was obtained from all participants before enrollment in the study. All the study protocols were carried out in accordance with the Declaration of Helsinki Guidelines. The RCC group consisted of 56 patients who underwent radical or partial nephrectomy for RCC during the study period. The control group included 56 healthy kidney donors and 13 patients with benign renal masses. All RCC and benign renal neoplasm diagnoses were pathologically confirmed by surgical resection. The benign renal neoplasms included five angiomyolipomas, four oncocytomas, three adenomas, and one case of pyelonephritis.
2. Preparation of blood samples
Blood was sampled from the RCC patients and controls preoperatively on the day of surgery. To investigate serial changes in PHD3 levels, blood was sampled again 1 and 3 months postoperatively in the RCC group. The blood samples were centrifuged for 15 minutes at 1,000g within 30 minutes of collection, and the serum was then divided into aliquots and stored at −80℃.
3. Enzyme-linked immunosorbent assay (ELISA) for PHD3
For each serum sample, the PHD3 level was analyzed using ELISA. Anti-PHD3 antibody was purchased from Ab-Frontier (mouse monoclonal 28A1, Seoul, Korea). Serum was diluted 2-fold before analysis. Recombinant PHD3 protein and diluted serum were coated onto the surface of 96-well ELISA plates overnight at 4℃ with 0.1 M sodium bicarbonate buffer (pH 9.6). The coated plates were blocked with 5% skim milk in Tris-buffered saline (TBS) for 1 hour at 37℃. After washing with TBS, the wells were then incubated with primary antibody (diluted 1:500 in blocking solution) for 2 hours and subsequently washed and incubated with secondary antibody (diluted 1:3,000 in blocking solution) for 1 hour. After a final washing step, 50 µL of tetramethylbenzidine substrate was added to each well, and the reaction was stopped by the addition of 1 N H2SO4. Absorbance was determined at 495 nm using a spectrophotometer. All assays were performed in duplicate.
4. Statistical analysis
To investigate the effects of age and sex on serum PHD3 level, the results in the control group were analyzed according to sex and age (≤50 years vs. >50 years). As the patients in the RCC group were significantly older than the participants in the control group, we performed multivariate linear regression analysis to evaluate whether the presence of RCC affects the serum level of PHD3 independently of age. In the RCC group, changes in the serum PHD3 level were evaluated according to tumor size, pathologic stage, Furmann grade, and histology. To evaluate the diagnostic utility of serum PHD3 level, quantification results were compared between the RCC and control groups. Receiver operating characteristic (ROC) curves were constructed, and the data were analyzed based on the area under the curve (AUC). The optimal cutoff value (indicating maximum sensitivity and specificity) was calculated using the Youden index. ROC curves were also generated for subgroups of RCC patients with tumor size >2 cm or clear-cell histology. To investigate the utility of serum PHD3 level for RCC monitoring, PHD3 levels were compared pre- and postoperatively. Differences in quantitative values were compared using Student's t-test or one-way ANOVA. Differences in qualitative variables were compared using the chi-square test or Fisher's exact test. Preoperative and postoperative PHD3 levels were compared using the paired t-test. Statistical analyses were performed using the PASW Statistics for Windows version 18.0 (SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered indicative of statistical significance, and all p-values were two-sided. ROC analyses and graphics plotting were performed using R, version 3.2.5 (https://www.r-project.org).
Go to :
RESULTS
1. Patient characteristics
The characteristics of the study cohort are summarized in Table 1. The control group consisted of 56 healthy kidney donors and 13 patients with benign renal masses. Patients in the RCC group were significantly older than the controls. However, the PHD3 level did not differ according to age (≤50 vs. >50 years, 0.73±0.09 ng/mL vs. 0.73±0.10 ng/mL; p>0.05) or sex (male vs. female, 0.73±0.09 ng/mL vs. 0.74±0.10 ng/mL; p>0.05). Additionally, no significant difference in PHD3 level was observed between healthy kidney donors and patients with benign renal masses (healthy donors vs. benign renal mass patients, 0.73±0.09 ng/mL vs. 0.73±0.09 ng/mL; p>0.05). Of the 56 patients with RCC, 43 (76.8%) had T1a disease, and 44 (78.6%) had clear-cell histology RCC. Non-significant trends of higher PHD3 levels were observed in patients with larger-size, higher-grade, and T2-stage tumors, and in those with clear-cell histology (Table 2).
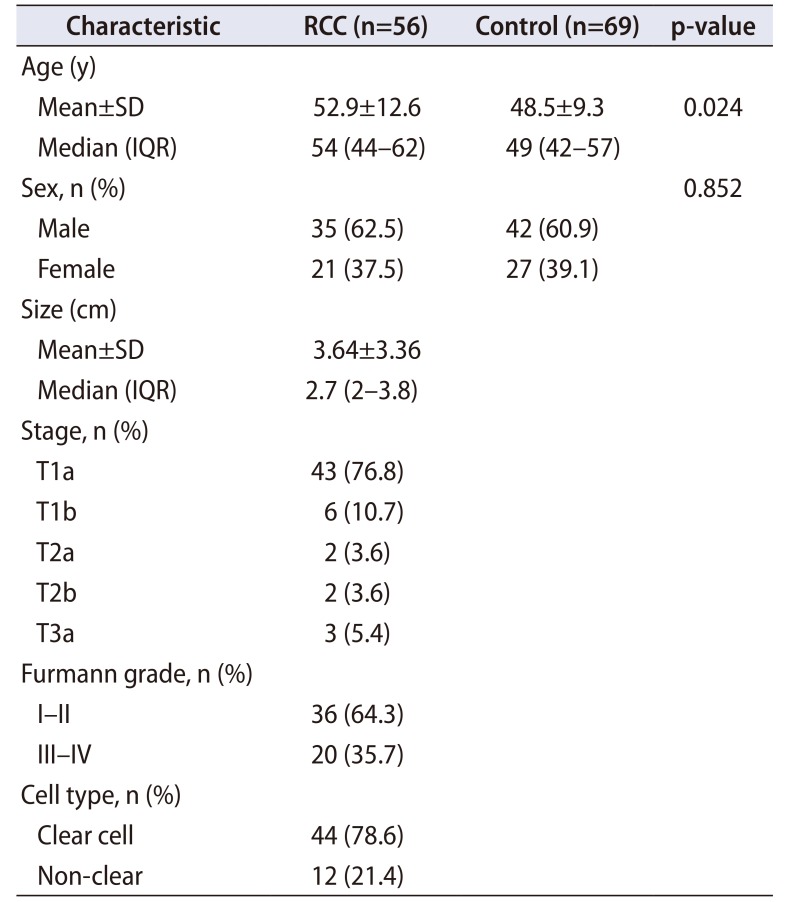
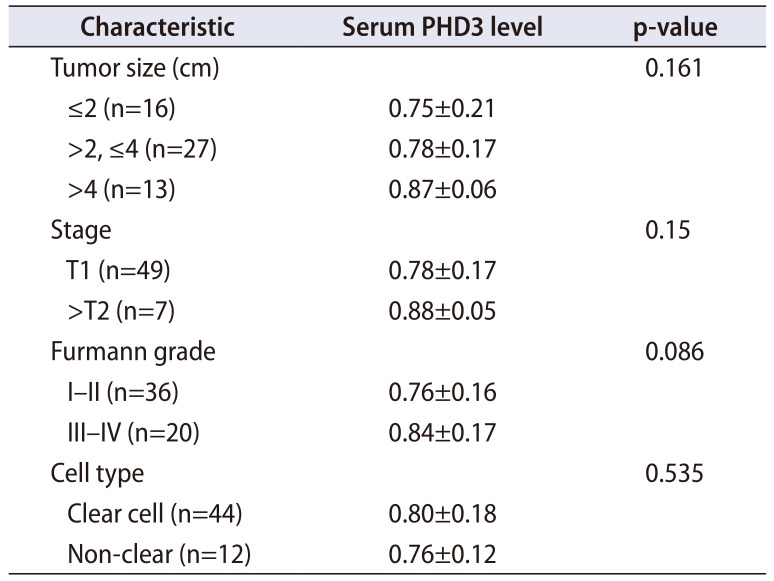
Table 1
Clinical and pathological characteristics of the study cohort
![]()
Table 2
Serum PHD3 level according to tumor characteristics in patients with renal cell carcinoma
![]()
2. Diagnostic performance of PHD3
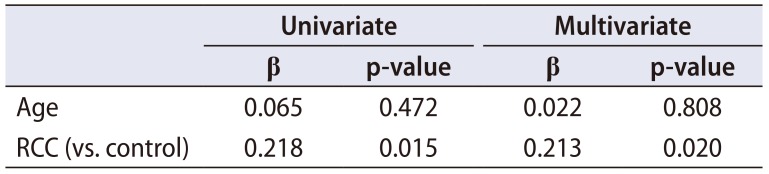
RCC patients had higher serum PHD3 levels than the controls (0.79±0.17 ng/mL vs. 0.73±0.09 ng/mL; p=0.023) (Fig. 1A). In the multivariate linear regression analysis, presence of RCC significantly affected the PHD3 serum level regardless of age (Table 3). Analyses of ROC curves for all cases (n=56) versus all controls (n=69) revealed an AUC for PHD3 of 0.668 (95% CI, 0.565–0.769) (Fig. 1B). Using a cutoff value of 0.761 ng/mL, as calculated according to the Youden index, the sensitivity, specificity, positive predictive value, and negative predictive value were 66.1%, 68.1%, 28.8%, and 37.3%, respectively. ROC curve analyses were also performed for subgroups of RCC cases. The PHD3 AUCs for patients with tumor size >2 cm (n=40) and patients with clear-cell histology (n=44) were 0.709 and 0.688, respectively.
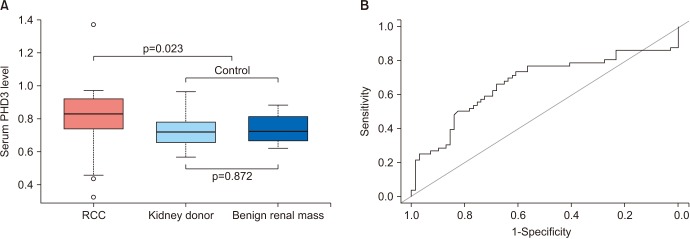 | Fig. 1(A) Difference in serum prolyl hydroxylase-3 (PHD3) levels between renal cell carcinoma (RCC) patients and controls. The control group included both healthy kidney donors and patients with benign renal masses. (B) Receiver operating characteristic curve for PHD3 comparing RCC patients (n=56) and controls (n=69). The AUC for PHD3 was 0.668 (95% confidence interval, 0.565–0.769).
|
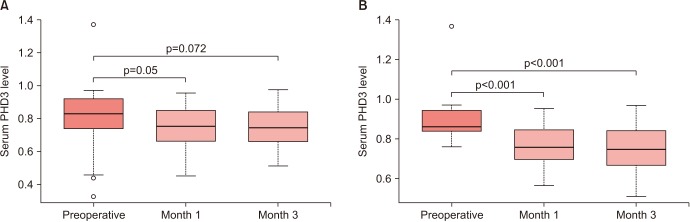
3. Serial changes in serum PHD3 level after surgery in RCC patients
The mean PHD3 level in the RCC patients at postoperative months 1 and 3 had decreased from the preoperative level (Fig. 2A). For the 37 patients with PHD3 levels greater than the cutoff value of 0.761 ng/mL, the level was decreased in 33 patients (89.2%) at postoperative month 1, and in 31 patients (83.8%) at postoperative month 3 (Fig. 2B). Paired t-test analyses revealed that the PHD3 levels at postoperative months 1 and 3 were significantly lower than the preoperative PHD3 levels (both p<0.001).
Go to :
DISCUSSION
The results of the present study revealed that PHD3 levels are significantly higher in RCC patients than in healthy, cancer-free individuals. PHD3 levels did not differ by age, sex, or presence/absence of benign renal masses. In addition, although not statistically significant, correlations of PHD3 level with tumor size, stage, and grade were observed, indicating that this marker can potentially reflect tumor burden and/or aggressiveness. The diagnostic performance of PHD3 was improved when considering only those patients with tumor size >2 cm. An active surveillance cohort study reported no association between a tumor size <2 cm and delayed intervention [12]. We suggest that measurement of the PHD3 level will yield superior diagnostic accuracy in significant RCC.
Multiple potential RCC biomarkers have been investigated for diagnostic or monitoring purposes [13141516]. The HIF pathway plays an important role in the development of RCC, and recent studies have demonstrated that downstream molecules of HIF such as carbonic anhydrase IX or angiopoietin-like 4 could be utilized as biomarkers of RCC [13]. PHDs are also closely related to HIF signaling, which is critical in the hypoxic conditions of the tumor microenvironment. Under normoxic conditions, PHDs inactivate HIFs via hydroxylation of a specific domain, resulting in the binding of VHL to HIF and subsequent proteasomal degradation [517]. In contrast, PHD activity decreases under hypoxic conditions, and subsequent HIF accumulation leads to the expression of HIF target genes, enabling tumor cells to survive under hypoxic conditions.
The role of PHD3 has been examined in multiple human cancers such as pancreatic, gastric, breast, and colorectal cancer [781819]. In most studies, PHD3 plays a tumor-suppressive role by promoting apoptosis of tumor cells [78181920]. The level of PHD3 expression is also associated with favorable oncologic outcomes in RCC [21]. Another study involving lung cancer, however, suggested a tumor-promoting function of PHD3 [22]. The mechanism underlying the effect of PHD3 on tumor progression has yet to be fully elucidated. PHD3 may enhance cell cycle progression and the survival of cancer cells by decreasing the stability of cyclin-dependent kinase inhibitor p27 or through involvement in glucose metabolism [781819]. A recent study suggested that PHD3 plays a role in the maintenance of the high glycolytic rate, as well as lactate production, in clear-cell RCC, thus contributing to tumor progression [23].
A previous transcriptional study showed that PHD3 expression is highly up-regulated in RCC tissues compared with that in normal kidney tissues [11]. Sato et al. [10] reported that PHD3 is a potent immunogenic antigen in RCC. In a subsequent study, researchers d discovered that the serum anti-PHD3 antibody levels in RCC patients are significantly higher than those in healthy controls. These results were similar to those of our study. Nevertheless, our study has several advantages over prior studies. First, our study included patients with benign renal masses in the control group, and we demonstrated that PHD3 could be utilized for differentiation between malignant and benign renal masses. Second, the current study included more than twice the number of participants in the study by Tanaka et al. [9]. We also investigated the association between PHD3 and age, sex, and tumor characteristics such as mass size, stage, and histology.
Most studies on the relationship between HIF and PHD3 have been performed on clear-cell RCC. Although increasing evidence supports a role of HIF in other types of RCC, PHD3 expression in non-clear-cell RCC is not widely reported [24]. In our study, the PHD3 level was higher in patients with non-clear-cell RCC than in the healthy controls. Overexpression of PHD3 in papillary RCC was demonstrated in a previous study, using immunohistochemistry, indicating that the expression of PHD3 might be independent of mutations in the VHL gene [10]. Although no statistically significant relationship was observed due to the small number of patients with non-clear-cell RCC, the results suggest that PHD3 might be informative in the diagnosis of this RCC type. This theory should be explored in further research involving more patients with non-clear-cell RCC than that in the current study.
Our study is not devoid of limitations. First, the control group had few benign renal masses and did not include patients with other malignancies. Although upregulation of PHD3 expression in other malignancies has been reported, data from the cBioPortal (http://www.cbioportal.org) [25] showed that PHD3 expression is extremely high in RCC (Fig. 3). We believe that PHD3 might be a more specific marker of RCC. Second, we observed patients with RCC who had PHD3 levels comparable to those of healthy controls, which might reflect low tumor burden or inter-individual differences in PHD3 expression. Additional VHL and HIF genetic profiling data could help identify factors associated with the expression of PHD3. Third, we did not investigate the association between the PHD3 level and prognosis. During follow-up, which had a median duration of 27 months, only 2 patients experienced recurrence, which was an insufficient number for statistical analysis. A prolonged follow-up study in patients with more advanced stages of RCC is required to evaluate the prognostic value of PHD3. Fourth, there was significant difference in age between the RCC and control groups, as the control group mainly consisted of healthy kidney donors. However, the PHD3 level did not differ according to age in the control group and age did not affect the level of PHD3 in multivariate analysis (Table 3). The last limitation of our study protocol is that it did not include postoperative blood sampling in the control group. Thus, we cannot exclude the effect of renal volume reduction on the postoperative decrease in serum PHD3 level in the RCC group.
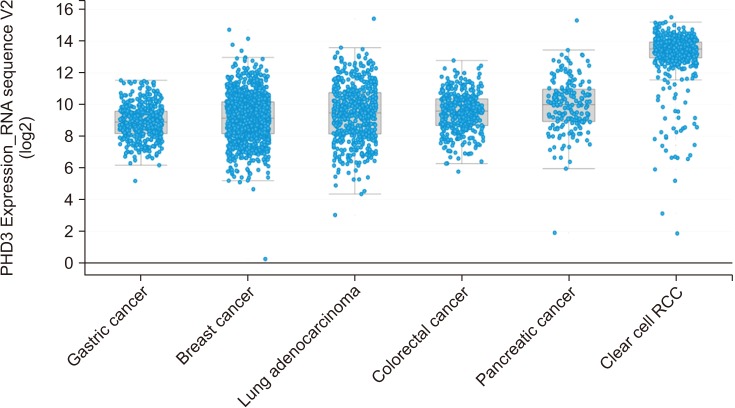 | Fig. 3Data for prolyl hydroxylase-3 (PHD3) expression level from cBioPortal (http://www.cbioportal.org). Cancer types associated with upregulated PHD3 expression were included in the analysis. The median level of PHD3 expression was higher in clear-cell renal cell carcinoma (RCC) than in other types of malignancy.
|
Go to :
CONCLUSIONS
Serum PHD3 can serve as a novel biomarker of RCC diagnosis and postsurgical monitoring, and shows acceptable diagnostic performance. It can also help differentiate RCC from benign renal masses. Although our findings should be validated in a larger cohort, serum PHD3 appears to be suitable for clinical application in diagnosing and monitoring patients with RCC.
Go to :
 XML Download
XML Download