

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Sinus membrane perforation is the most prevalent intraoperative complication encountered by clinicians during sinus floor augmentation via lateral access [12]. A recent systematic review demonstrated a mean prevalence of sinus membrane perforation of 15.7% [3]. As it has been reported to be highly associated with sinus infection, inadequate amounts of regenerated bone, and a lowered implant survival rate, many previous studies have argued for the necessity of repairing perforated sinus membranes and suggested appropriate repair protocols [45]. Resorbable collagen membrane (CM) has been documented for years as a candidate material for sealing perforated sinus membranes [67]. Clinical studies have investigated the implant survival rate in sinus floor augmentation when a perforated sinus membrane is covered with CM, and the outcomes have shown no significant difference from routine sinus floor augmentation [28].
Dehydrated human amnion/chorion membrane (dHACM) is a sterilized allograft derived from donated human placentae. Bi-layered amnion/chorion membrane surrounds the amniotic cavity and the fetus in the uteri of pregnant women, and it lines the inner surface of the placenta [9]. The amnion membrane within the bi-layered amnion/chorion membrane, including the epithelium, basement membrane, and avascular connective tissue, is in direct contact with the amniotic fluid and the fetus [10]. The chorion membrane is adjoined to the amnion membrane and contains only avascular connective tissue with multiple layers [10]. The human amnion/chorion membrane in its dried and sterilized form has been brought to market commercially as a surgical dressing material for soft tissue healing, and it has been used extensively in various medical contexts because it contains numerous biomolecules that promote wound healing and soft tissue regeneration [911]. In vitro tests have confirmed that dried amnion/chorion membrane grafts release regulatory proteins such as platelet-derived growth factor-AA and BB, transforming growth factor-α and β, angiogenin, and epidermal growth factor [1012], and amnion membrane grafts were found to have favorable biologic properties, including low immunogenicity, anti-inflammatory effects, and analgesic effects [1113]. In dental surgery, dried amnion membrane successfully induced healing processes in mucosal and bone defects caused by the surgical resection of cancerous or precancerous lesions [14]. In addition, the amnion/chorion membrane has been evaluated as a soft tissue barrier for periodontal regenerative therapy for furcation defects [15] and as a wound dressing for implant and vestibuloplasty surgery [1617]. The use of amnion membrane combined with a coronally advanced flap for root coverage treatment has been documented [18]. Thus, given its biologic healing potential and clinical usability, amnion/chorion membrane has the potential to be a useful option to prevent the loss of graft materials and to promote healing of perforated sinus membranes. The aim of this study, therefore, was to assess the effectiveness of dHACM grafts in a sinus floor augmentation model with sinus membrane perforations of a standardized size.
MATERIALS AND METHODS
Animals
Fourteen adult male New Zealand white rabbits (Koatech, Pyeongtaek, Korea) weighing from 2.8 to 3.0 kg were used in this study. The animals were kept in individual cages within a standard laboratory environment (temperature 23°C±3°C, humidity 55%±15%, and ventilation 10 to 20 times/hour). All animals were fed a standard laboratory pellet diet with free access to water. All procedures related to the animals were approved by the Institutional Animal Care and Use Committee at the Korean Animal Medical Science Institute (approval No. 16-KE-042; Guri, Korea). This animal study was designed and performed in compliance with the Animal Research: Reporting In Vivo Experiments (ARRIVE) guidelines [19]
dHACM
dHACM (BioXclude®, Snoasis Medical, Denver, CO, USA) grafts were manufactured from human placentae donated from cesarean sections. Before donation, donors were checked for underlying diseases to prevent the transmission of infectious diseases. Donated placentae were prepared following the manufacturer's protocol, described briefly as follows. Placental tissue was gently washed with sterile water several times and then dehydrated and stabilized into sheet form. After drying, the dHACM tissue was packed and processed by electron-beam irradiation for sterilization (Figure 1A).
 | Figure 1(A) Commercial dHACM. (B) Bilateral surgical areas (7-mm diameter) were prepared on the nasal bone, and the sinus membrane was elevated and perforated (5-mm diameter). The perforated sinus membrane on the left was untreated, whereas the perforated sinus membrane on the right was covered with dHACM. (C) Deproteinized porcine bone mineral was subsequently grafted on both elevated sinuses. (D) A metal pin (as a reference point) was fixed on the midline suture, and then the periosteum was sutured. (E, F) Field emission scanning electron microscope images of dHACM.dHACM: dehydrated human amnion/chorion membrane.
|
The surface characteristics of the dHACM were analyzed using a field emission scanning electron microscope (FE-SEM; SUPRA40VP®, Carl Zeiss Co., Oberkochen, Germany). The dHACMs were sputter-coated with osmium for 12 seconds, and then images were taken under 2.0 kV. Figure 1E and F presents FE-SEM images of dHACM, with crater-like structures and an overall irregular and rough surface.
Experimental design
The number of experimental animals was calculated using G*Power version 3.1 freeware (Heinrich Heine Universität Düsseldorf, Düsseldorf, Germany; www.gpower.hhu.de) [20]. The probability of α error was set at 0.05, and the statistical power was set at 0.80. The effect size was determined based on previous research into sinus floor augmentation in rabbits [21]. The experimental groups were categorized according to the method used to repair the perforated sinus membrane during sinus floor augmentation: the dHACM group, in which the perforated sinus membrane was covered with dHACM followed by sinus grafting; the CM group, in which the perforated sinus membrane was covered with resorbable CM followed by sinus grafting; the negative control (NC) group, which underwent sinus grafting without repair of the perforated sinus membrane; and the positive control (PC) group, which underwent sinus grafting without perforation of the sinus membrane.
Bilateral sinus floor augmentation procedures were carried out on the nasal bone of each animal, for a total of 28 sinus augmentation procedures performed on the 14 animals. One investigator (Y.Y.C.) performed the random distribution of the experimental groups. Random allocation of the 4 experimental groups was conducted using the block randomization method [22], in which the 4 surgical sites in 2 animals were set as a single block. The 4 experimental groups were then randomly allocated among the 4 surgical sites within a block.
Surgical procedures
All surgical procedures were performed in a standard operating room under an aseptic field. Two experienced surgeons (S.H.K. and Y.Y.C.) performed the operations under general and local anesthesia. General anesthesia was induced by intravenous injection of tiletamine/zolazepam (Zoletil®, Virbac, Carros, France) and xylazine (Rumpun®, Bayer, Seoul, Korea). Each nasal bone was subsequently shaved and disinfected with povidone-iodine. Local anesthesia was administered with lidocaine (2% lidocaine HCl with 1:100,000 epinephrine, Kwang Myung Pharmaceutical, Seoul, Korea) on the nasal skin. The surgical site was determined by referring to a previous study that suggested using this maxillary sinus augmentation model in rabbits [232425]. An approximately 20-mm vertical incision was made along the midline suture of the nasal bone, and the full-thickness flap was bilaterally elevated to expose the surgical sites. For the perforated sinus membrane model, 2 circular areas with a diameter of 7.5 mm were determined bilaterally along the midline suture and marked with a surgical pencil. Point drilling using an implant twist drill with a diameter of 2.0 mm was done at the center of each indicated circular area. The drill perforated the sinus mucosa and penetrated into the sinus cavity, and then 2 circular areas were prepared with a commercially available instrument (MILAKit®, Megagen Co. Ltd., Gyeongsan, Korea) without sinus membrane tearing under saline irrigation. The circular windows were carefully removed. After confirming the point perforation at the center of each circular defect, the sinus membrane was gently elevated from the lateral border of the circular area. Thereafter, sequential twist drills with diameters ranging from 2.0 to 5.0 mm were manually placed into the perforated point of the sinus membrane without the use of a rotary drilling engine to widen the perforation (Figure 1B). The dHACM and CM (BioGide®, Geistlich Biomaterials, Wolhusen, Switzerland) used for the dHACM and CM experimental groups were cut into 8×8 mm2 squares and applied to the perforated membrane, followed by the placement of 0.15 g of particulated deproteinized porcine bone mineral (THE Graft®, 0.25–1.0 mm, Purgo Biologics, Sungnam, Korea) in the elevated sinus cavity (Figure 1C). In the NC group, no repair treatment was performed on the perforated sinus membrane; only the deproteinized porcine bone mineral was grafted. Then, a metal pin (Membrane Pin®, Dentium, Seoul, Korea) was placed on the midline suture as a reference point. The surgical areas were left uncovered, and a periosteum-releasing incision was made immediately. The periosteum and skin flap were sutured layer by layer with 5-0 polyglactin 910 absorbable material (Vicryl®, Ethicon, Johnson and Johnson, Cincinnati, OH, USA) (Figure 1D) and 4-0 glycolide synthetic absorbable monofilament (Monosyn®, B-Braun, Hessen, Germany). Antibiotics (enrofloxacin, 5 mg/kg, Baytril®, Bayer, Leverkusen, Germany) and non-steroidal anti-inflammatory drugs (ketorolac, 5 mg/kg, Keromin®, Han Pharm, Seoul, Korea) were administered to the animals for 7 days. In the PC group, the sinus membrane perforation procedure was not conducted, but preparation of the surgical area, elevation of the sinus membrane, and grafting of the bone biomaterials were carried out just as in the other groups. Six weeks postoperatively, the animals were euthanized by the administration of CO2 under general anesthesia. Block specimens including the surgical sites were obtained and fixed in 10% neutral-buffered formalin for 10 days.
Micro-computed tomography (micro-CT) analysis
The fixed block specimens were scanned using micro-CT (Viva CT 80®, Scanco Medical AG, Brüttisellen, Switzerland) at a resolution of 18 µm at 70 kVp and 114 µA. The scanned tomographic data were transformed into the Digital Imaging and Communications in Medicine format and reconstructed into 3-dimensional images using software (µCT Evaluation program V6.6, Scanco Medical AG, Brüttisellen, Switzerland). The augmented sinuses were color-coded 3-dimensionally, and the total augmented volume (mm3) of each augmented sinus was measured by an examiner (M.S.G.) masked to the experimental design.
Histologic process and histometric analysis
Following the micro-CT analysis, the fixed block specimens were decalcified in 5% formic acid for 14 days and then dehydrated and embedded in paraffin blocks using routine procedures. The central sections of the circular area around each reference micro-pin were coronally cut and processed at a thickness of 5 µm and then stained with Masson trichrome. The histologic slides were scanned using a digital panoramic scanner (Panoramic 250 Flash III, 3DHISTECH, Budapest, Hungary), and digital images of the histologic slides were used for histometric measurements. One experienced and blinded examiner (M.S.G.) performed the histometric measurements with a computer-assisted image-analysis system (Image-Pro Plus; Media Cybernetics, Rockville, MD, USA.) The total augmented area (TA, presented in mm2) referred to the entire tissue area demarcated by the antral native bone, overlying soft tissue, and inferior border of the lamina propria in the sinus membrane. The proportion of newly formed bone (NB) area, remaining biomaterial (RB) area, and fibrovascular tissue (FV) area within the TA were calculated individually and expressed as percentages. The percentages of the NB, RB, and FV areas in each group in the histometric analysis were determined as the primary outcome variable, and the total augmented volume in the micro-CT analysis was calculated as a secondary outcome variable.
Statistical analysis
Descriptive statistics are expressed as the mean and standard deviation, and as median and interquartile range for the micro-CT and histometric evaluations, respectively. The non-parametric Kruskal-Wallis test was carried out to determine the statistical significance of differences among the experimental groups. The presence of statistically significant differences between each pair of groups was confirmed by the Mann-Whitney U test. The level of significance was considered to be P<0.05. All statistical data were processed using a statistical analysis program (SPSS 22.0; IBM Corp., Armonk, NY, USA).
RESULTS
Clinical observations
All animals survived and did not show complications at any point during the healing period. As a result, 7 specimens per group were evaluated.
Micro-CT analysis
Cross-sectional images of the augmented sinuses and color-coded 3-dimensionally reconstructed images on the inner part of the augmented sinuses are shown in Figure 2. Generally, convex and antero-posteriorly elongated augmented areas were observed, with no specific morphological differences among the groups. In the cross-sectional micro-CT views, intact augmentation of the bone biomaterials and dislodgement of bone biomaterials could be observed in the NC group. All animals in the dHACM, CM, and PC groups showed relatively well-maintained biomaterial containment.
 | Figure 2Cross-sectional and 3-dimensional reconstructed micro-computed tomography images of sinus floor augmentation.NC: negative control, dHACM: dehydrated human amnion/chorion membrane, PC: positive control, CM: collagen membrane.
|
The total augmented volumes in the dHACM, CM, NC, and PC groups were 176.18±23.20 mm3, 171.95±40.46 mm3, 218.01±21.23 mm3, and 185.02±13.57 mm3, respectively (Table 1). No statistically significant differences were found among the experimental groups.
Table 1
Total augmented volume (mm3) in micro-CT analysis (n=7)

| Results | NC | dHACM | CM | PC |
|---|---|---|---|---|
| Mean±SD | 218.01±21.23 | 176.18±23.20 | 171.95±40.46 | 185.02±13.57 |
| Median (IQR) | 225.72 (200.93–234.42) | 187.12 (152.25–187.86) | 177.10 (157.77–196.45) | 179.15 (173.92–179.90) |
CT: computed tomography, NC: negative control, dHACM: dehydrated human amnion/chorion membrane, CM: collagen membrane, PC: positive control, SD: standard deviation, IQR: interquartile range.
![]()
Histologic analyses
NCs
The RBs were distributed throughout the augmented area, and NB was sparsely observed in the NC group (Figure 3A and B). The amount of NB varied depending on the specimen and was found mainly at the edge of the surgical window area and around the native septal bone region. The perforated sinus membrane could be observed, and the epithelial lining was discontinuous at the perforated site. Lamina propria infiltrated by inflammatory cells appeared to be directly exposed to the sinus cavity (Figure 3C). In the non-perforated area adjacent to the perforated site, the mucosal layer containing pseudostratified ciliated columnar epithelium and lamina propria was thickened, and inflammatory cells had infiltrated and congregated beneath the lining epithelium.
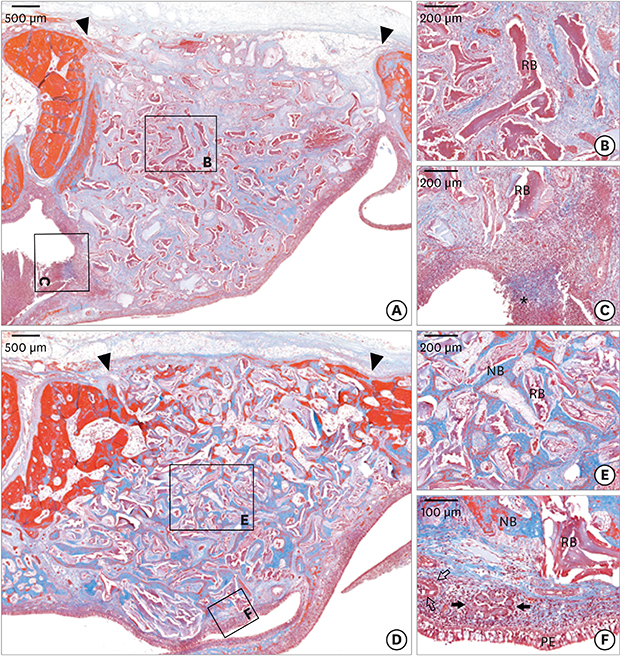
 | Figure 3Representative histologic views of the NC (A-C) and dHACM (D-F) groups 6 weeks after surgery. (A) Little NB was observed, and most RBs and fibrovascular tissue were in the augmented areas in the NC group. Discontinuous and perforated sinus membrane was observed. (B) Only RBs were deposited in the fibrovascular areas. (C) The lamina propria, containing a dense infiltration of inflammatory cells, was exposed to the sinus cavity. (D) Overall, the augmented areas in the dHACM group were embraced with the sinus membrane and densely packed with NB and RBs. (E) High-magnification view representing the center region of the augmented area. The NB was intimately connected to the RBs. (F) High-magnification view of the sinus membrane region. Pseudostratified ciliated columnar epithelium lined the augmented area, and a cluster of serous glands and small blood vessels were located in the lamina propria. An aggregation of inflammatory cells was also observed in the lamina propria (Masson's trichrome stain). Black arrow heads, asterisks, black arrows, empty black arrow are presented as the bony margin of the surgical window, perforated site, serous glands, and blood vessel, respectively.NC: negative control, dHACM: dehydrated human amnion/chorion membrane, NB: newly formed bone, RB: remaining biomaterial, PE: pseudostratified ciliated columnar epithelium.
|
dHACMs
NB in direct contact with the RBs was evident throughout the augmented area in the dHACM group (Figure 3D). In 2 specimens, the surgical window area was almost closed, with NB and RBs. The NB was not yet lamellated and was composed mainly of woven bone, containing numerous viable osteocytes and blood vessels (Figure 3E). In the non-perforated sinus membrane areas, the integrity of the augmented area was well maintained, with an intact sinus membrane. Pseudostratified ciliated columnar epithelium and lamina propria containing serous glands and small blood vessels were observed; however, the aggregation of inflammatory cells could also be observed (Figure 3F). In the healed sites that resulted from dHACM coverage in another specimen, the epithelial cell lining was mostly found to be non-ciliated and flat (Figure 4B). The lamina propria was replaced with cell-rich dense connective tissue and inflammatory infiltrates, and serous glands were seldom observed (Figure 4B). No dHACM fragment was discernible beneath the mucosal layer.
 | Figure 4Low- and high- magnification views of another specimen in the dHACM group. (A) NB had emerged from native bone and spread to the repaired sinus membrane regions. (B) Repaired sinus mucosa. The perforated, but repaired, sinus membrane adjacent to the ciliated columnar epithelium healed with non-ciliated, flat, and stratified epithelium. Inflammatory infiltration was also observed in the lamina propria, and serous glands were seldom observed (Masson's trichrome stain). Black arrow heads, black arrows, empty black arrow, and black dotted line are presented as the bony margin of the surgical window, pseudostratified ciliated columnar epithelium, healed and repaired non-ciliated stratified epithelium, and inferior border of lamina propria, respectively.RB: remaining biomaterial, dHACM: dehydrated human amnion/chorion membrane.
|
Resorbable CM
The overall histologic healing patterns in the CM group were similar to those in the dHACM group. New bone formation started from the wall of the native bone with surrounding biomaterials, and progressed to the center and sinus membrane regions (Figure 5A). Non-lamellated bone including multiple osteocytes constituted the NB (Figure 5B). At non-perforated sites, a lining of ciliated columnar epithelium and several clusters of serous glands were observed (Figure 5C), whereas at repaired and healed sites, flat and non-ciliated epithelial cells lined the augmented area and were connected to the native epithelium. The presence of CM could not be confirmed in the submucosal area.
 | Figure 5Representative histologic views of the CM (A-C) and PC (D-F) groups 6 weeks after surgery. (A) RBs were dispersed throughout the augmented areas, and the NB emerged from the native bone in the CM group. (B) High-magnification view showing new bone formation around native bone. (C) High-magnification view of the sinus membrane region. The lamina propria, including numerous serous glands and inflammatory cells, was relatively thick, similar to the dHACM group. (D, E) NB in direct contact with RBs was found at the bony margin of the surgical area and sinus membrane region in the PC group. (F) Ciliated columnar epithelium was well maintained, and abundant serous glands and small blood vessels were predominantly observed in the cell-rich lamina propria (Masson's trichrome stain). Black arrow heads, black arrows, and empty black arrows are presented as the bony margin of the surgical window, serous glands, and blood vessel, respectively.CM: collagen membrane, PC: positive control, dHACM: dehydrated human amnion/chorion membrane, NB: newly formed bone, RB: remaining biomaterial, PE: pseudostratified ciliated columnar epithelium.
|
PCs
The augmented areas were convex and enveloped by intact sinus membrane in the PC group (Figure 5D). The new bone seemed to form from the bone edge of the surgical area; however, new bone was found intensively in the sinus membrane region of 2 specimens (Figure 5D). Overall, substantial new bone formation occurred in all specimens. The NB was intimately connected with the RBs, all in an immature form (Figure 5E). The space among the RBs not surrounded by NB was filled with fibrovascular tissue. In the sinus membrane region, continuous pseudostratified ciliated columnar epithelium was observed, and small blood vessels and abundant serous glands were evident in the lamina propria (Figure 5F).
Histometric analysis
The histometric results are shown in Table 2. The TAs were 19.12±5.16 mm2, 17.89±2.40 mm2, 22.34±4.19 mm2, and 18.22±2.12 mm2 in the dHACM, CM, NC, and PC groups, respectively. There were no significant differences among the experimental groups. The individual histometric parameters (the percentage of NB, RB, and FV areas) within the TA did not show statistically significant differences between the dHACM and CM groups. The percentage of NB area in the dHACM group was significantly higher than in the NC group (11.18%±12.78% vs. 1.79%±3.03%; P=0.04), whereas no significant difference was observed between the CM and NC groups. The percentage of NB area in the dHACM and CM groups did not differ significantly from that in the PC group. A statistically higher percentage of NB area was observed in the PC group than in the NC group (16.63%±10.09% vs. 1.79%±3.03%; P=0.009). The percentage of FV area in the PC group was lowest, with significant differences from the other groups (34.91%±8.88% in the PC group vs. 72.59%±17.59%, 49.45%±12.15%, 59.03%±16.00%; P=0.006, 0.047, and 0.018 in the NC, dHACM, and CM groups, respectively).
Table 2
Histometric data within the TAs (n=7)

TA: total augmented area, NC: negative control, dHACM: dehydrated human amnion/chorion membrane, CM: collagen membrane, PC: positive control, NB: newly formed bone, RB: remaining biomaterial, FV: fibrovascular tissue, SD: standard deviation, IQR: interquartile range.
a)Statistically significant difference compared to the NC group; b)Statistically significant difference compared to the PC group.
![]()
DISCUSSION
This study was devised to evaluate the healing of dHACM in sinus floor augmentation procedures in cases of a perforated membrane. For this study, a standardized defect model was required because most previous studies investigating treatments for the repair of perforated sinus membranes have been limited to uncontrolled and accidental clinical indications. In this study, sinus membranes were perforated with a consistent size by manipulating implant twist drills. This ensured equal-sized, standardized perforations. The standardization of sinus membrane perforation size is of vital importance because the extent of bone regeneration in sinus floor augmentation, as well as its prognosis, is intimately associated with the perforation size [2].
A recent clinical case series evaluated the use of amnion/chorion membrane to repair perforated sinus membranes during sinus floor augmentation, and the results demonstrated that it might be a useful alternative [26]. However, controlled preclinical studies were needed to confirm and compare the biologic effects of dHACM in a sinus floor augmentation model with perforated sinus membranes. In this context, the NC and PC groups in the present study were designed to enable reliable conclusions to be drawn, and a comparative evaluation with CM, which has been widely evaluated for sinus membrane repair, was also performed.
The healing process for the formation of new bone in the dHACM group was not only in agreement with that observed in the PC group (augmented sinuses without perforation), but also with that in a recent randomized clinical human study that investigated maxillary sinus floor augmentation using the same bone biomaterials used in this study [27]. In the sinus membrane region, 2 histologic patterns of healing were observed in the dHACM group. At non-perforated sites, pseudostratified ciliated columnar epithelium and serous glands were observed; however, inflammatory cells were also detected in the lamina propria. At the perforated but repaired sites, the sinus membrane was healed mainly with non-ciliated and flat epithelium. Inflammatory cells congregated in the lamina propria, and serous glands were absent in the lamina propria. These histologic observations were also found in the CM group and are in accordance with the findings of a previous study [28] that investigated sinus membrane regeneration after surgical membrane removal in rabbits. Those results are also confirmed by previous studies that showed the healing of perforated sinus membranes during sinus floor augmentation [2129].
The finding of a significantly higher percentage of NB area in the dHACM group than in the NC group suggests that dHACM repair of the perforated sinus membrane positively affected new bone formation compared with the absence of a repair treatment (NC group). Thus, it is necessary to repair a perforated sinus membrane with an adequate material such as dHACM because an untreated sinus membrane perforation is highly associated with inflammation around the perforation; furthermore, escaped bone biomaterials are closely related with sinus cavity inflammation [130], which has a negative impact on new bone formation in sinus floor augmentation, as confirmed in this study.
Recently, 2 preclinical studies with experimental goals similar to that of the present study were consecutively published. In one experiment performed in rabbits [31], a resorbable collagen membrane was used to cover the perforated sinus membrane in maxillary sinus floor augmentation. The percentage of NB area in the group repaired using the resorbable collagen was comparable to that shown in the dHACM group in this study. In the other experiment, which was conducted in sheep [32], new bone formation was evaluated in sinus floor augmentation in cases of a perforated sinus membrane. Test groups in which perforated sinus membranes were repaired using resorbable collagen were compared to a non-repair control group. The results showed that the proportion of NB area did not differ significantly between the test group and control group, which is inconsistent with our results. This discrepancy might have resulted from the major differences in the control groups of the 2 studies. The percentage of NB area in the NC group in this study was 1.79%±3.03%, whereas it was 12.3%±7.9% in the control group in that study. The percentage of NB area in the NC group in this study was therefore much lower than that in the control group in their study, possibly because of heterogeneity in the experimental animal species, graft materials, and coverage of surgical window.
In the PC group, the augmented areas were well enclosed, with sinus membrane containing ciliated columnar epithelium and lamina propria with abundant serous glands, whereas the repaired and healed sinus membrane in the dHACM group presented different histologic observations (as described above). Previous research reported that healed and regenerated sinus membrane exhibited decreased mucociliary activity and function [3334]. However, other research revealed that the mucociliary function of regenerated sinus membrane could improve during long healing periods [3536]. The percentage of NB area in the dHACM group did not differ significantly from that in the PC group. In this respect, it could be suggested that implant placement in sinus floor augmentation healed by dHACM is clinically acceptable. A previous retrospective study revealed a high implant survival rate in sinus floor augmentations with a perforated but repaired sinus membrane [437]. Furthermore, the sinus membrane repaired using the dHACM could be expected to show better mucosal healing upon long-term observation because of the numerous biomolecules derived from the dHACM. Hence, a longer observational period is needed to obtain a better understanding of the healing of dHACM.
In this study, the surgical window area was not covered by resorbable CM. Covering the surgical area with a resorbable CM is based on the principle of guided bone regeneration; therefore, new bone formation initiated from the edge of the native bone area might be enhanced in some situations by secluding the overlying soft tissue with a barrier membrane. Because this effect could positively influence new bone formation and mask the statistical results, the surgical area was not covered in this study.
This study had a low level of statistical power due to its small sample size, even though a comparative experimental design with NC and PC groups was adopted. Further studies with larger sample sizes should be conducted to increase the reliability of the conclusions.
Within the limitations of this study, the results suggest that the stable and secure repair of perforated sinus membranes increases new bone formation. dHACM demonstrated comparable outcomes to those obtained using conventional resorbable CM for the repair of perforated sinus membranes. Therefore, dHACM could be a feasible solution for repairing sinus membrane perforations that occur during sinus floor augmentation.
 XML Download
XML Download