

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dental implants are a well-established option for replacing missing teeth [1]. Various implant treatment protocols have been introduced to meet a variety of needs, especially in terms of timing [2]. Depending on the post-extraction healing period, implant placement can be classified as immediate, early, or late. Additionally, alveolar ridge preservation is a popular method used for late placement [345]. In deciding the timing of implant placement, a dilemma often arises when selecting the type of approach used for prompt restoration of aesthetic appearance and chewing function (e.g., immediate and early implant placement) or other approaches that allow sufficient healing (e.g., late implant placement and alveolar ridge preservation). This dilemma has led to extensive research regarding changes in the ridge profile after tooth extraction and in conjunction with specific treatments [3678].
Of particular concern is the ridge profile of the anterior maxillary area [910111213]. Patients demand a short treatment period and favorable aesthetic outcomes. However, clinicians encounter difficulties when treating the anterior maxilla for the following reasons: i) the high remodeling tendency of labial bone, ii) the small labio-oral dimension of the alveolar ridge, and iii) facial concavity [1415]. Following tooth extraction, the tooth-dependent bundle bone starts to be resorbed, which may lead to a significant bone deficit. This resorption may necessitate primary bone augmentation in cases where the alveolar ridge has small dimensions. Moreover, the facial concavity should be properly managed, especially for prosthetically driven implant placement, depending on its extent.
The abovementioned issues indicate the necessity of assessing the ridge profile systematically. Moreover, physiological changes in the ridge profile are highly influenced by baseline status (i.e., alveolus with tooth embedment). Thus, irrespective of implant placement timing, adequate knowledge of this subject is of the utmost importance.
Hence, the present study aimed to i) analyze the ridge profile of the anterior maxilla using cone-beam computed tomography (CBCT) scans and ii) assess the clinical significance of the ridge profile by means of virtual implant placement.
MATERIALS AND METHODS
A cross-sectional observational study was conducted. Images obtained by CBCT from January 2010 and December 2016 at Kyung Hee University Dental Hospital were analyzed. The protocol of the present study was approved by the Institutional Review Board (IRB) of Kyung Hee University Dental Hospital (approval number: KHD IRB-1709-3).
CBCT images of i) adults aged 20–50 years; ii) patients who underwent CBCT scans of the maxillary central incisors, lateral incisors, and canine; and iii) patients who were periodontally healthy and assessed using radiography (radiographic bone level from cementoenamel junction ≤3 mm) were included. Inappropriate CBCT scans with low resolution, scattering, and distortion were excluded. In the included CBCT scans, individual teeth were examined and the following teeth were excluded: i) teeth with dental prostheses, ii) root canal-treated teeth, iii) teeth with pathologic changes around the roots (presence of radiolucency), iv) teeth with root anomalies, v) malaligned teeth, and vi) teeth showing altered passive eruption.
Radiographic evaluation
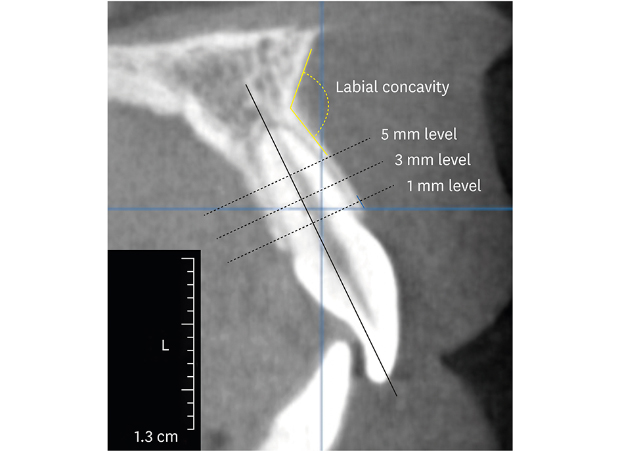
CBCT scans were performed using an Alphard VEGA (Asahi, Kyoto, Japan) at 80 kVp and 8 mA for 17 seconds. Images were obtained from volume data of the cone type with a field size of 51×51 mm (height×diameter). Image measurements were performed using Zetta PACS (Tae Young Soft, Anyang, Korea). The central cross-sectional images were identified in all included teeth. In these images, a vertical reference line was created along the longitudinal axis of the tooth, and three horizontal reference lines at 1-, 3-, and 5-mm levels below the labial bone crest were then drawn perpendicularly to the vertical reference line. Subsequently, the thickness of the total ridge (RT_1, RT_3, and RT_5), the labial bone plate (LT_1, LT_3, and LT_5), and the palatal bone plate (PT_1, PT_3, and PT_5) were measured at the 3 levels. Moreover, the angle of labial concavity was measured using 2 tangent lines along the labial bone plate (Figure 1).

Virtual implant placement
Virtual implant placement was performed using computer software with an implant library (Ondemand3D In2Guide; CyberMed Co., Seoul, Korea). Two types of dental implants, a standard implant (Straumann® Bone level; Straumann AG, Basel, Switzerland) and a tapered implant (Straumann® Bone level Tapered; Straumann AG), were placed in a prosthetically driven manner, with reference to the previous literature [161718]. Screw-retained restoration was planned for all implants. With regard to the platform diameter, 4.1 mm was selected for the central incisor and canine and 3.3 mm for the lateral incisor. The length of the implant was determined considering the requirement of sufficient primary stability in the palatal and apical areas of the socket. After completion of the implant placement, the proximity of the implant with respect to the labial bone plate in the apical area was categorized as follows: exposure outside of the bone plate, <1 mm between the implant and the labial plate, and ≥1 mm between the implant and the labial plate.
Examiner calibration
Image measurements were performed using Zetta PACS (Tae Young Soft) by 2 investigators (D.U.K. and H.P.). Prior to the measurement of all images, intra-examiner calibration was performed under the supervision of a senior investigator (H.C.L.). Ten random images were selected and measured. The inter-class correlation coefficient was 0.961, with a 95% confidence level of 0.940–0.974 (P<0.001).
Statistical analysis
The data were expressed as mean ± standard deviation. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Inc., Cary, NC, USA). A generalized linear mixed model (GLMM) was used to determine the statistical significance of differences in RT, LT, PT, and labial concavity between men and women. In addition, GLIMMIX (GLMM for categorical variables) was used to determine the statistical significance of differences in apical perforation according to implant type. In those analyses, the random variable for the mixed model was analyzed by setting the subjects as patient (ID), and the effect on the tooth number (FDI tooth numbering system) was corrected. The statistical significance level was set at P<0.05.
RESULTS
A total of 108 CBCT scans were initially obtained. After excluding inappropriate CBCT scans with low resolution, scattering, and distortion, 32 scans were analyzed. The study samples consisted of 13 men and 19 women, with a mean age of 30.4 years (range, 20–48 years). Subsequently, all teeth (from the left canine to right canine) were individually inspected to determine which teeth are eligible for analysis. Finally, 36 central incisors (tooth #11: n=16, tooth #21: n=20), 29 lateral incisors (tooth #12: n=14, tooth #22: n=15), and 19 canines (tooth #13: n=8, tooth #23: n=11) were included in the analysis. No teeth demonstrated bony dehiscence in the labial bone plate, but 14 teeth had labial fenestration between the middle and apical portion of the root (tooth #11: n=2, tooth #12: n=5, tooth #22: n=1, tooth #13: n=3, tooth #23: n=3).
Linear measurements of the alveolar ridge
Total width of the alveolar ridge
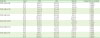
Canines had the greatest mean RT at all levels, followed by central incisors and lateral incisors. In all teeth, the mean RT increased from the 1-mm level to 5-mm level: central incisors, from 8.2±1.1 mm to 8.8±1.9 mm; lateral incisors, from 7.7±0.9 mm to 8.1± 1.3 mm; and canines, from 9.7±1.5 mm to 10.7±1.9 mm. Generally, men showed greater RT values than did women at all levels of all tooth types. Statistically significant differences were found in RT_1 (10.5±0.8 mm vs. 9.3±1.0 mm) of tooth #23, RT_3 of tooth #11 (9.2±2.0 mm vs. 7.2±1.6 mm) and tooth #21 (9.2±1.8 mm vs. 8.0±0.8 mm), RT_3 (11.6±1.2 mm vs. 9.5±1.4 mm) of tooth #23, and RT_5 (11.9±1.2 mm vs. 9.6±1.8 mm) of tooth #23 (P<0.05) (Table 1).
Table 1
RT at 1-, 3-, and 5-mm levels below the labial bone crest (in mm)
![]()
Width of the LT
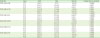
The mean LT of lateral incisors was generally smaller than that of the incisors and canines, especially at the levels of 3 and 5 mm. In central incisors, a relatively constant value of LT was measured from the 1-mm level to 5-mm level compared with other tooth types (between 0.9±0.3 mm for LT_5 and 1.1±0.4 mm for LT_3). In lateral incisors and canines, the mean LT gradually decreased, from 1.0±0.4 mm to 0.6±0.4 mm for lateral incisors and from 1.3±0.6 mm to 0.9±0.5 mm for canines. At all levels and for all tooth types, there were no statistically significant differences between males and females (P>0.05) (Table 2).
Table 2
LT at 1-, 3-, and 5-mm levels below the labial bone crest (in mm)

![]()
When LT was dichotomized into categories of ≥1 mm and <1 mm, 50%, 52.8%, and 61.1% of central incisors had less than 1 mm of LT at the 1-, 3-, and 5-mm levels, respectively. Meanwhile, 44.8% of lateral incisors had less than 1 mm of LT at the 1-mm level, 72.4% at the 3-mm level, and 86.2% at the 5-mm level. Lastly, 31.6% of canines had less than 1 mm of LT at the 1-mm level, 42.1% at the 3-mm level, and 68.4% at the 5-mm level (Figure 2).
 | Figure 2Proportions of the teeth according to the LT. LT_1, LT_3, and LT_5 are LT at 1-, 3-, and 5-mm levels below the labial bone crest.LT: thickness of the labial bone plate.
|
One central incisor, 1 lateral incisor, and 5 canines demonstrated more than 1.5 mm of LT. Only 2 teeth (1 lateral incisor and 1 canine) showed more than 2 mm of LT.
Width of the PT
Generally, the mean PT was greater than the mean LT, except at the 1-mm level of canines. Along the levels, PT increased in all tooth types (from 1.3±1.0 mm to 3.4±1.9 mm for central incisors, from 1.4±0.8 mm to 3.6±1.7 mm for lateral incisors, and from 1.2 ±1.0 mm to 4.0±1.8 mm for canines), and the difference between PT and LT was highest at the 5-mm level in all tooth types. Men demonstrated significantly greater PT_1 of tooth #13 (2.4±0.4 mm vs. 0.8±0.7 mm), PT_3 of tooth #13 (4.3±0.9 mm vs. 2.4±1.1 mm), and PT_5 of tooth #12 (3.8±1.2 mm vs. 2.7±0.9 mm) than did women (P<0.05) (Table 3).
Table 3
PT at 1-, 3-, and 5-mm levels below the labial bone crest (in mm)
PT: thickness of the palatal bone plate.
a)Statistically significant difference between men and women.
![]()
Labial concavity
The greatest mean value of labial concavity was observed for canines (14.9°±2.3º), followed by lateral incisors (12.4°±2.6°) and central incisors (11.8°±2.4°). Labial concavity was generally greater in women than in men, except for tooth #23. No significant difference was observed in labial concavity between men and women (P>0.05).
Influence of sex on ridge dimension and labial concavity following adjustment for tooth number and individual subjects
Due to the inclusion of multiple teeth from 1 individual and inclusion/exclusion of the same tooth type from different locations, tooth number and subjects were adjusted. The RT values at all levels were significantly greater in men than in women (P<0.05). The estimated difference between men and women was 0.87 mm, 1.47 mm, and 1.62 mm for RT_1, RT_3, and RT_5, respectively. The LT values were not significantly different between men and women (P>0.05), but PT_3 and PT_5 were significantly greater in men than in women (P<0.05). The estimated differences at PT_3 and PT_5 were 0.91 mm and 1.28 mm, respectively. Labial concavity was not significantly different between men and women (P>0.05).
Virtual implant placement
The tapered implants led to less apical fenestration than the standard implants (12 of 84 vs. 20 of 84) (Figure 3). Moreover, a greater number of the tapered implants had ≥1 mm of space between the implant and the labial plate (59 of 84 vs. 34 of 84). When apical status was dichotomized as fenestration and no fenestration, tapered implants demonstrated statistically significantly less fenestration (P<0.05). The extent of fenestration ranged from 1 to 3 mm in both length and width.

DISCUSSION
The present study investigating the ridge profile of the anterior maxilla demonstrated that i) the maxillary anterior teeth was located labially, based on the total, labial, and palatal thickness (RT, LT, and PT) of the ridge; ii) a large number of teeth had LT of less than 1 mm between the 1-mm level and 5-mm level below the crest; iii) the LT of lateral incisors was narrower compared with other tooth types; iv) men had greater RT than did women (significantly different at the 1-mm level), but men and women had comparable LT; v) labial concavity appeared similar irrespective of tooth type and sex; and vi) less apical fenestration occurred when tapered implants were used.
To achieve better aesthetic outcomes after dental implant therapy, a certain critical thickness of the facial bone has been suggested. Based on retrospective studies, 2 mm of facial bone is warranted in the facial area with respect to the implant [1920]. Maintenance of this critical thickness may be greatly influenced by the dimensional change in the alveolar bone following extraction, indicating the necessity of evaluating the profile of the alveolar ridge. Moreover, for accurate implant placement in a 3-dimensionally correct position, knowledge regarding the ridge profile is of the utmost importance. Currently, CBCT technology and the related software allow easy evaluation of the ridge profile, including the total, facial, and palatal thickness of the ridge and the concavity of the facial bone plate.
In the samples included in the present study, the teeth (central and lateral incisors and canines) were located labially. The proportion of LT in relation to RT along the ridge was smaller than that of PT in relation to RT. Although the total thickness of the ridge increased, this increase was related to the palatal bone plate. Previously, the location of these teeth in the alveolus was investigated using CBCT [2122], and approximately 81% and 79% of anterior teeth, respectively, were positioned toward the labial bone plate. Those results are in line with the results of the present study.
The abovementioned labial location of the teeth led to a thin labial bone plate. The mean LT_1 of all tooth types (1.0±0.3 mm for central incisors, 1.1±0.9 mm for lateral incisors, and 1.3±0.6 mm for canines) and LT_3 of central incisors (1.1±0.4 mm) and canines (1.2±0.7 mm) were ≥1.0 mm, but the LT values were less than 1 mm for the rest. Some previous studies demonstrated more or less similar results regarding labio-coronal bone thickness (between 0.90 and 1.09 mm [12], between 1.01 and 1.23 mm [23], and between 0.89 and 1.29 mm [24]), while others demonstrated a relatively smaller labial bone thickness (between 0.6 and 0.7 mm [1125]; between 0.45 and 0.54 mm [9]). In particular, a study conducted in the Korean population exhibited smaller labial bone thickness for central incisors (0.68±0.29 mm, measured at 3 mm below the cementoenamel junction) [26]. These differences may be due to the characteristics of the included patients and sample size.
The most important finding of this study is that the majority of teeth showed less than 1 mm of LT at least at one measurement level (77.8% for central incisors, 89.7% for lateral incisors, and 73.7% for canines). Following tooth extraction, a tooth-dependent bundle bone undergoes resorption [14]. The dimensions of this structure were found to be 0.1–0.4 mm [27] and 0.2–0.5 mm [28] in histological and radiological analyses, respectively. Thus, the resorption of the bundle bone concomitantly with the trauma from tooth extraction is likely to jeopardize the integrity of the labial bone plate. However, the clinical significance of the resultant ridge profile after extraction might differ depending on the level of the thinnest bone before extraction.
Clinically, the labial location of the anterior teeth with thin labial plates influenced all types of implant placement timing. Especially for immediate implant placement, such anatomical aspects may yield detrimental aesthetic outcomes when not properly managed (i.e., mid-facial gingival recession over time) [2930]. In cases of early implant placement, the space for a thin labial bone plate is replaced with soft tissue, which is known as spontaneous soft tissue thickening [31]. This thickened soft tissue limits the need for additional soft tissue grafting. For delayed implant placement, an alveolus with a thin labial plate is likely to require major bone augmentation; this tendency may be even higher in lateral incisors because the total thickness of the alveolar bone in this area is smaller than that for other teeth. Lastly, for alveolar ridge preservation, resorption of the thin labial plate may still require bone augmentation at the time of implant placement.
Interestingly, men and women had comparable LT values, even though the RT values were greater in men than in women. The PT of central (teeth #11 and #21) and lateral incisors (teeth #12 and #22) in men was similar to that of women, except for PT_5 of tooth #12. For canines, PT_1 and PT_3 were significantly greater in men at tooth #13 than in women. This, in turn, indicates that the difference in RT was influenced by the size of the central and lateral incisors, which concurs with the findings of a previous study demonstrating no statistically significant differences from the crest to 2 mm below the crest for the central and lateral incisors between men and women [25].
In the present study, the labial concavity between the central incisor and canine had a tendency to increase. This is due to the presence of the canine fossa. Compared with other previous studies, the amount of concavity was not pronounced. However, the influence of this concavity should be evaluated in conjunction with its location: depending on the thickness of the ridge at the level of concavity and occlusion, the position of a prospective implant may cause fenestration of the labial bone plate.
The virtual implant placement of the present study demonstrated the risk for apical fenestration in the anterior maxilla, even though most of the implants placed in a prosthetically driven manner did not harm the integrity of the labial bone plate. This apical fenestration may be prevented using tapered implants. Virtually placed tapered implants (n=12) caused significantly less apical fenestration than standard implants (n=20). However, in the present study, the diameter for each tooth type was pre-set; thus, if a smaller diameter is chosen, the possibility of fenestration may be reduced. Moreover, it should be taken into account that the extent of the fenestration was minor in the present study, indicating that augmentation procedures to compensate for fenestration may not be difficult.
There are some limitations of the present study. First, discrepancies between the present study and others may have been due to the small sample size. Of particular note are the different findings between the present study (32 patients) and another study (20 patients) conducted in the Korean population [26]. Second, the present study included only Koreans; therefore, some of the findings might not be generalizable to other ethnic groups. Different dento-skeletal relationships between ethnic groups may play a role in the ridge profile of the anterior maxilla [12]. Third, virtual implant placement did not consider occlusion, and thus some correction of the implant position might be required in real patients.
Taken together, the present study demonstrated that most of the teeth in the anterior maxilla have thin labial bone plates due to their location. A large number of teeth had area(s) with less than 1-mm thickness of labial bone between the 1- and 5-mm level below the crest. No statistically significant differences were found in the thickness of the labial bone plate between men and women. The placement of a tapered implant may reduce the risk of apical fenestration in the anterior maxilla.
 XML Download
XML Download