

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Diabetes is an endocrine disorder characterized by hyperglycemia.1 The prevalence of diabetes continues to increase in modern society.2 Diabetes is known to be closely related to food intake. Oral health status is an important factor in maintaining good nutrient intake. Even in the absence of oral diseases, such as periodontitis or dental caries, masticatory performance can be affected by the use of a dental prosthesis and may vary according to the type of prosthesis. Preferences for different food types may depend on the chewing difficulty involved.
Dental prostheses can be divided into fixed dental prostheses and removable dental prostheses. Fixed dental prostheses include tooth-supported fixed prostheses and implant-supported fixed prostheses, which are reported to exhibit masticatory forces similar to those exhibited by natural teeth. Removable dental prostheses can be readily inserted and removed by the patient.3 They are classified into removable partial dentures and removable complete dentures.3 Removable partial dentures are generally supported by the remaining natural teeth. Their masticatory performance varies depending on the number and position of natural teeth and the quality of the denture-bearing tissue. Removable complete dentures are generally fabricated when there are no teeth remaining in the jaw, and they are reported to be less stable and less efficient for mastication than any other type of dental prosthesis.45
Diabetes is frequently found in dental patients and is associated with oral health.6 Several studies have suggested that diabetes is positively associated with periodontitis7 and the number of missing teeth.8 Accordingly, a higher number of patients with diabetes may require dental prostheses to replace missing teeth. Therefore, the masticatory performance of the dental prosthesis may also affect the nutritional intake of patients with diabetes.
Although several studies have suggested a potential association between diabetes and oral health status, a limited number of studies have reported on the connection between diabetes and the use of a removable dental prosthesis.9 Therefore, this study aimed to investigate whether the use of removable dental prostheses affects diabetes and glycemic control using a representative sample of Korean adults.
METHODS
Survey and participants
Data from the Korean National Health and Nutrition Examination Survey (KNHANES) 2008–2010 were analyzed in this study. The KNHANES is a nationwide, cross-sectional survey conducted by the Korean Centers for Disease Control and Prevention and the Korean Ministry of Health and Welfare.10 This survey is conducted annually to monitor the health and nutritional status of the Korean population. All study procedures were conducted in accordance with the Declaration of Helsinki. Trained interviewers and examiners documented information about the study participants via a health interview, a health examination, and a nutrition survey.
Initially, 29,235 participants were included in the KNHANES. Because the use of a removable complete denture before the age of 50 years is reportedly rare,1112 the data of participants aged ≥ 50 years who participated in all 3 parts of the survey, including the dental examination (n = 10,238), were analyzed in this study. Participants who had not fasted for > 8 hours (n = 771) were excluded. Those who did not have data for fasting plasma glucose or serum insulin levels (n = 1,312) were also excluded. In total, 8,155 participants (3,525 men and 4,630 women) were ultimately included in this study (Fig. 1).

Use of dental prostheses and the classification of groups
Oral examinations were performed by trained public health dentists. The upper and lower jaws were scored separately with regard to the dental prosthesis as follows: score 0, natural teeth only without any dental prosthesis; score 1, one fixed dental prosthesis only; score 2, more than 1 fixed dental prosthesis; score 3, removable partial denture without a fixed dental prosthesis; score 4, removable partial denture with a fixed dental prosthesis; and score 5, removable complete denture.
According to the above scores, the participants were classified into 3 mutually exclusive groups as follows: Group NF did not use any type of removable dental prosthesis (natural teeth only or fixed dental prostheses including dental implants with fixed superstructures; scores of 0–2 on both jaws); Group RPD used removable partial dentures but not removable complete dentures (scores of 3 or 4 for at least 1 jaw, but no score of 5 for either jaw); and Group CD used at least 1 removable complete denture (score of 5 for at least 1 jaw).13
Diabetes and glycemic control
Trained examiners collected venous blood samples from participants who had fasted for > 8 hours. The samples were immediately centrifuged and refrigerated. Fasting plasma glucose, total cholesterol, high-density lipoprotein-cholesterol (HDL-C), and triglyceride (TG) levels were analyzed using a Hitachi Automatic Analyser 7600 (Hitachi, Tokyo, Japan) with an enzymatic method. Serum insulin levels were gauged using an immunoradiometric assay with a 1470 Wizard Gamma Counter (PerkinElmer, Turku, Finland).
The definition of diabetic patients was taken from the KNHANES of the Korea Centers for Disease Control and Prevention.10 Diabetic patients were defined as those with fasting plasma glucose ≥ 126 mg/dL, taking insulin or anti-diabetic medication, or diagnosed with diabetes mellitus by a physician.14
Glycated hemoglobin (HbA1c) levels ranging between 6.5% and 7.0% (48–53 mmol/mol) have been targeted in recent recommendations for strict glycemic control for patients with diabetes.115 In addition, the KNHANES and the Korean Diabetes Association define uncontrolled blood glucose as an HbA1c level ≥ 6.5%.1016 Based on these results, we used an HbA1c level of 6.5% as a cut-off value for uncontrolled diabetes.
Evaluation of the association between diabetes and the use of dental prostheses
The prevalence of diabetic patients in three groups, NF, RPD, and CD, classified according to the type of dental prosthesis used, was compared. The proportion of patients with controlled diabetes in each dental prosthesis group was also compared. In addition, after the potential confounders were analyzed, the relationship between diabetes and the type of dental prosthesis was analyzed after adjusting for potential confounders.
Potential confounders
All participants were asked to complete a self-reported questionnaire that contained data about sociodemographic and lifestyle characteristics, including age, place of residence (urban or rural), marital status, smoking habits, alcohol consumption, and physical activity. According to their answers in the questionnaires, the participants were categorized as non-smokers, ex-smokers, or current smokers. Based on the average quantity of alcohol consumed per day during the month prior to the interview, the participants were classified into the following 3 groups: non-consumer, mild consumer (1–30 g/day), and heavy consumer (> 30 g/day).17 To assess the degree of physical activity of each subject, the International Physical Activity Questionnaire was used.18 Regular physical exercisers were defined as those who exercised moderately for > 30 min/session, more than 5 times/per week, or who exercised vigorously for > 20 min/session, more than 3 times per week.
Trained examiners measured the participants' weights, heights, and waist circumferences to the nearest 0.1 kg, 0.1 cm, and 0.1 cm, respectively. Weight was measured with an electronic scale, and height was measured with a portable stadiometer. Waist circumference was measured with a measuring tape at the narrowest point between the costal margin and the iliac crest at the end of a normal expiration. By dividing the weight in kg by the height in m2 (kg/m2), the body mass index (BMI) was obtained. Systolic and diastolic blood pressure was measured with a mercury sphygmomanometer (Baumanometer; Baum, Copiague, NY, USA). These were measured 3 times, and the mean of the last 2 values was calculated and used.
The frequency of daily tooth brushing was represented by the number of times the subject brushed their teeth daily. Secondary oral products included dental floss, interdental toothbrushes, electric toothbrushes, and gargling solutions.
Statistical analysis
Statistical analysis of the KNHANES data was performed using SAS version 9.3 for Windows (SAS Institute, Inc., Cary, NC, USA) due to the complex sampling design and the sampling weights in the KNHANES data. The χ2 test for categorical variables or the independent t-test for continuous variables was performed to assess the differences in characteristics among the groups categorized according to dental prosthesis used.
Multivariable logistic regression analyses were performed to examine the association between the risk of diabetes and the use of dental prostheses. Statistical calculations were also performed after adjusting for age, BMI, smoking habits, alcohol consumption, physical activity level, household income, educational level, and frequency of daily tooth brushing (Models 1 and 2). P < 0.05 was considered to indicate a statistically significant difference.
Ethics statement
The survey protocol was reviewed and approved by the Institutional Review Board of the Korean Centers for Disease Control and Prevention (approval No. 2008-04EXP-01-C, 2009-01CON-03-2C, and 2010-02CON-21-C). Informed consent was submitted by all participants when they were enrolled.
RESULTS
Tables 1 and 2 list the characteristics of the study participants categorized by gender and prosthodontic treatment. Table 1 shows the general and clinical features of the participants. Table 2 shows the relationship between their oral health status and the study group to which they belong. The demographics of the target population were as follows: the mean age was 61.1 years, and the percentage of men was 47.3%. The percentage of participants using removable dental prostheses increased with increasing age (P < 0.001) (Fig. 2).
Table 1
General characteristics of participants according to gender and type of dental prosthesis used

Data are presented as the mean ± standard error or % (standard error).
NF = no removable dental prosthesis, RPD = removable partial denture but not removable complete denture, CD = at least 1 removable complete denture, BMI = body mass index, FPG = fasting plasma glucose, HbA1c = glycated hemoglobin, HDL-C = high-density lipoprotein-cholesterol, LDL-C = low-density lipoprotein-cholesterol, WBC = white blood cell count.
aData are obtained only from diabetic patients; bdata are presented as geometric mean (95% confidence interval).
![]()
Table 2
Dental characteristics of participants according to gender and type of dental prosthesis used

Data are presented as % (standard error).
NF = no removable dental prosthesis, RPD = removable partial denture but not removable complete denture, CD = at least 1 removable complete denture.
![]()
 | Fig. 2Distribution of groups according to age in men (P < 0.001) and women (P < 0.001).NF = no removable dental prosthesis, RPD = removable partial denture but not removable complete denture, CD = at least 1 removable complete denture.
|
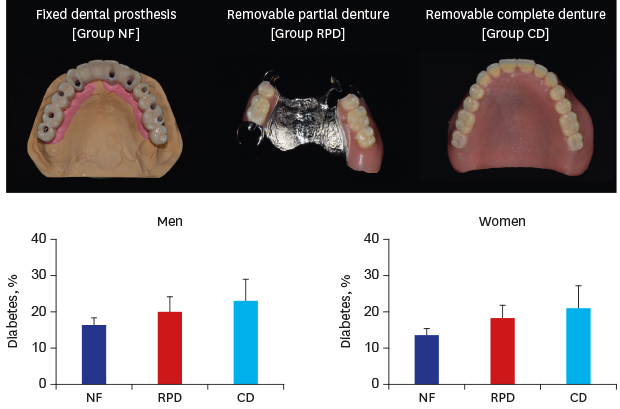
The prevalence of diabetes was lowest in the NF group, higher in the RPD group, and highest in the CD group for both genders (P = 0.009 and < 0.001 for men and women). In addition, fasting plasma glucose levels in the participants followed a similar trend, being lower in the NF and RPD groups than in the CD group (P = 0.166 and 0.07 for men and women) (Fig. 3).
 | Fig. 3Prevalence of diabetes according to groups in men and women. The prevalence of diabetes increased across the dental prosthesis groups (P < 0.01). The error bars represent the upper 95% confidence interval.NF = no removable dental prosthesis, RPD = removable partial denture but not removable complete denture, CD = at least 1 removable complete denture.
|
The associations between diabetes and the dental prosthesis groups in the multivariable logistic regression models are presented in Table 3. Removable complete denture wearers (group CD) had a 1.49-fold higher risk of having diabetes than the group NF participants among men after adjusting for age, BMI, smoking habits, alcohol consumption, exercise, household income, education level, and the number of times they brushed their teeth per day (adjusted odds ratio [OR], 1.491; 95% confidence interval [CI], 1.034–2.151). In addition, the adjusted ORs for diabetes were significantly increased in the order group NF, group RPD, and group CD in the men population. In the women population, after adjusting for age and/or other variables, the adjusted ORs for diabetes were slightly increased in the ascending order in group NF, group RPD, and group CD. However, no statistically significant association was found between diabetes and the use of dental prostheses in the women participants (Models 1 and 2).
Table 3
Adjusted ORs of diabetes and glycemic control according to the type of dental prosthesis

Data are presented as odds ratio (95% confidence interval).
NF = no removable dental prosthesis, RPD = removable partial denture but not removable complete denture, CD = at least 1 removable complete denture.
aAdjusted for age; badjusted for age, body mass index, smoking status, alcohol consumption, exercise, household income, education level, and number of times teeth brushed per day; cdefined as glycated hemoglobin < 6.5%.
![]()
The results relating to blood glucose control (defined as HbA1c < 6.5%) are also shown in Table 3. Similar to the association between the prevalence of diabetes and the use of dental prostheses, glycemic control was also significantly associated with the use of dental prostheses in men participants (P = 0.021). Men participants who wore complete dentures (group CD) exhibited poorer glycemic control (defined as HbA1c ≥ 6.5%) compared with men participants who did not use any type of removable dental prostheses (group NF) after adjustment for variables (OR, 0.232; 95% CI, 0.091–0.591).
DISCUSSION
The present study statistically evaluated the association between diabetes and the use of removable dental prostheses based on a nationwide survey. Among Korean adults aged ≥ 50 years who participated in the KNHANES, the prevalence of diabetes and glycemic control were significantly associated with the use of removable dental prostheses in men participants after adjusting for several potentially confounding variables.
The results of the present study can be interpreted in several ways. First, inadequate nutritional intake by individuals wearing removable dentures may be associated with diabetes. Removable denture wearers usually prefer softer foods over harder or foods that are difficult to chew.19 This is due to the maximum biting force of complete denture wearers being 1/7 to 1/4 of the force of the average person with intact dentition.45 Therefore, for complete denture wearers, the quantity of foods that are difficult to chew, such as vegetables, consumed is reduced due to their reduced chewing ability.2021 These changes in food consumption may lead to nutritional deficiencies, and may be associated with the development of metabolic syndrome and poor glycemic control.52223 From this point of view, fixed partial dentures and implant-supported fixed dental prostheses may be a better choice of treatment than removable dentures to enhance the health of patients with diabetes.21 In Table 3, for women, the significance of the results disappeared after adjusting for the confounding factors. This may be due to gender differences in interests or patterns of food intake in older people.242526 Further research will be needed to identify these gender differences.
A second possible explanation for the findings of the present study is that diabetes is associated with several dental problems that necessitate the use of removable dental prostheses. First, diabetes increases the risk of periodontitis.727 Diabetes increases oxidative stress and the production of glycation end-products. Therefore, immune function is altered, and periodontitis is induced.28 The development of dental caries is also associated with diabetes. The prevalence of dental caries is higher in the diabetic population than in the nondiabetic population.2930 According to a study by Murrah,31 decreased salivary flow and an increased level of glucose in the parotid saliva may result in an increased incidence of caries in individuals with diabetes. In addition, individuals with type 2 diabetes have higher rates of apical periodontitis than nondiabetic patients.32 Patients with uncontrolled diabetes have a higher incidence of several types of oral infection, including dental pulp infection.33 Therefore, individuals with diabetes may have more missing teeth compared without diabetes due to the higher incidence rates of dental caries, apical periodontitis, and periodontal disease.3234 Additionally, according to Lee et al.,8 the number of missing teeth is positively associated with fasting plasma glucose levels in the rural elderly population.
To restore missing teeth, some patients with diabetes are advised to obtain removable dental prostheses rather than fixed dental prostheses, such as implant-supported prostheses. This is because achieving implant osseointegration is more difficult in patients with poorly controlled diabetes.35 A patient’s blood HbA1c level has also been reported to be 1 of the most important factors affecting the implant complication rate.36 In addition, type 2 diabetes is more prevalent in lower socio-economic groups.37 It may be difficult for those with a lower socio-economic status to receive high-cost fixed dental prostheses, such as implant-supported prostheses, for their edentulous area. For these reasons, patients with diabetes are more likely to receive a removable dental prosthesis than an implant-supported fixed dental prosthesis.
The present study had a number of limitations, predominantly due to its cross-sectional design. As exposure and outcome were assessed simultaneously, causality was not clear.38 Another limitation was that all the participants were Asians, and the dietary habits of Asians may differ from those of other cultures. The type and combination of medications that are administered is important for the control of diabetes; however, these could not be analyzed, which represents a limitation of this study. In addition, the duration of diabetes is a significant confounding factor affecting glycemic control. However, due to the limitation of the KNHANES data, the duration of diabetes could not be adjusted in the present study. Furthermore, in elderly diabetic patients, the recommended HbA1c level is approximately 7% or over 7% or less than 7.5%–8%, especially in those who have experienced hypoglycemic events.394041 The HbA1c cut-off level < 6.5% used in the present study could be too low for those patients. Therefore, in interpreting the results of this study, the limitations related to these factors should be considered.
Despite these limitations, the present study had several strengths. First, the oral condition of the participants was professionally classified into 3 mutually exclusive groups according to their use of removable dental prostheses. Based on this grouping scheme, a detailed analysis was performed. In addition, data in the present study were collected by specialists, whereas previous studies used self-reported data.9 The present study also used blood samples to evaluate glucose levels in participants. Furthermore, the majority of previous studies evaluated small numbers of participants and did not consider possible confounding variables.
Previous studies linked the number of natural teeth to the incidence of systemic diseases.4243444546 Even if participants have the same number of residual natural teeth, there are large differences in masticatory force between edentulous sites restored with a fixed dental prosthesis, including dental implants, and those restored with a removable dental prosthesis. Thus, it is also important to analyze the health status of patients according to their type of dental prosthesis, as in the present study.
In conclusion, the present study showed that men who use removable dental prostheses, particularly removable complete dentures, were more likely to have diabetes. The prevalence of uncontrolled diabetes was higher in those who wore removable complete dentures than in those who wore other types of dental prostheses. Therefore, it might be necessary for endocrinologists and dentists to consider the potential risk of uncontrolled diabetes when examining patients with removable dental prostheses. Further prospective cohort studies are required to obtain a better understanding of the underlying mechanisms.
 XML Download
XML Download