

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Chronic infection with hepatitis C virus (HCV) is a leading cause of liver disease in over 170 million infected individuals worldwide.1 Persistent HCV infection leads to the development of chronic liver disease, liver cirrhosis (LC), and hepatocellular carcinoma (HCC).2 Therefore, the primary goal of antiviral treatment for chronic hepatitis C (CHC) is to prevent HCV-related morbidity and mortality, including complications of liver fibrosis or cirrhosis and the development of HCC.3 HCV infection can be cured by achieving a sustained virological response (SVR) defined as undetectable HCV RNA at 12 weeks (SVR12) or 24 weeks (SVR24) after treatment completion. In the past, treatments with pegylated interferon (PEG-IFN) plus ribavirin were standard therapy for chronic HCV infection, however, SVR rate was relatively low and patients frequently discontinued the treatment due to various adverse events. Nevertheless, it has been reported that SVR after PEG-IFN plus ribavirin administration maintains the durability of SVR, inhibits hepatic inflammation and fibrosis, and has good clinical outcomes.45
In these days, many oral antiviral drugs called direct-acting antivirals (DAAs) with low adverse effects and high SVR rates have been developed. The combination of oral daclatasvir (DCV), a non-structural 5A (NS5A) inhibitor, and asunaprevir (ASV), a second generation NS3 protease inhibitor, is the first drug combination approved in Korea for the treatment of HCV genotype 1b (GT1b)-infected patients. In a previous clinical trial, DCV/ASV treatment provided favorable SVR rates (82%–90%) and low adverse events.6 Because the presence of NS5A resistance-associated substitution (RAS) is known to cause the failure of DCV/ASV treatment, it is recommended that the administration of DCV/ASV treatment should be done on patients without NS5A RAS.
However, treatment failure can sometimes occur in patients without NS5A RAS, and the risk factors for treatment failure remain unclear. Additionally, due to limited clinical data, it remains unclear whether the SVR is maintained and fibrosis is improved after the achievement of SVR.
In this study, we aimed to assess the efficacy of DCV/ASV treatment in patients without NS5A RAS, and to evaluate the durability of SVR after achievement of SVR12, the cause of treatment failure, and the change of liver function and non-invasive fibrosis markers after DCV/ASV treatment.
METHODS
Patients
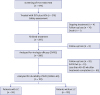
A total of 474 patients with HCV GT1b infection who were examined in NS5A RAS testing between September 2015 and March 2017 at five hospitals were enrolled in this retrospective study. Patients with decompensated cirrhosis, HCC-requiring treatment, a history of liver transplantation, or coinfection of other HCV genotypes were excluded. Of the 366 patients without NS5A RAS, 316 patients were treated with DCV/ASV treatment and 297 patients finished the treatment. Except for follow-up loss, 288 patients who had confirmed HCV RNA testing at 12 weeks after treatment completion were finally included for the evaluation of efficacy. Of these patients, durability of SVR was analyzed in 191 patients who underwent HCV RNA testing after achievement of SVR12 (Fig. 1). In addition, changes of non-invasive fibrosis markers between baseline and 48–60 weeks after treatment completion were evaluated in patients who showed durable SVR.
Diagnostic criteria of cirrhosis
LC was diagnosed by liver biopsy or clinical findings such as an irregular liver surface or splenomegaly on radiologic images, varices on endoscopy, and thrombocytopenia (< 150 × 103/μL). Patients that met at least two of these clinical findings (a cirrhotic liver image, splenomegaly, varices, and thrombocytopenia) were diagnosed as having liver cirrhosis, as previously described.7
Treatment regimen
DCV and ASV were administered orally at doses of a 60-mg capsule once daily and a 100-mg tablet twice daily for 24 weeks, according to the manufacturer's prescribing information.
Assessment of resistance-associated substitutions
HCV NS5A RASs at Y93 and L31 were detected by commercial direct sequencing assays using a Veriti® 96-Well Thermal Cycler and a genetic analyzer (Applied Biosystems, Carlsbad, CA, USA) with the upper limit of quantification set at 5,000 IU/mL. The result was recorded as “positive” or “negative” according to the presence of NS5A RAS sites L31 or Y93. If result was “not detected,” reexamination of the HCV genotype was done to exclude the other genotype. NS5A RAS was reaffirmed in some patients without SVR after treatment completion.
Assessment of efficacy and safety
Efficacy was assessed by measuring the virologic response after treatment. End treatment response (ETR) was defined as undetectable HCV RNA at the end of 24 weeks of treatment and SVR12 was defined as undetectable HCV RNA at 12 weeks after treatment completion. Durability of SVR after achievement of SVR12 was defined as undetectable HCV RNA at 48–60 weeks after treatment completion. Safety was assessed by measuring the rate of occurrence and severity of adverse events. Adverse events were identified by a review of medical records.
Laboratory data
Biochemical markers including serum aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin, total bilirubin, creatinine levels, and prothrombin time were measured using standard laboratory procedures. HCV RNA was measured by a real-time PCR assay using the m2000SP/m2000RT (Abbott Molecular, Des Plaines, IL, USA; lower detection limit 12 IU/mL) or Cobas AmpliPrep/Cobas TaqMan (Roche Molecular Systems, Pleasanton, CA, USA; lower detection limit 15 IU/mL). Virologic breakthrough was defined as an increase of HCV RNA > 1 log10 from nadir or HCV RNA ≥ lower limit of quantification (LLOQ) after a measurement below LLOQ.
Non-invasive fibrosis markers
In order to assess the degree of liver fibrosis, non-invasive fibrosis markers such as AST to platelet ratio index (APRI), FIB-4 index, and fibrosis index (FI) were used. These markers were calculated using the following formulae: APRI = [(AST/upper limit of nor-mal)/platelet count (109/L)]×100; FIB-4 index = age (years) × AST [U/L]/(platelet count (109/L) × (ALT [U/L])1/2); FI = 8.0–0.01 × platelet count (109/L) - serum albumin (g/dL) at baseline, and 48-60 weeks after treatment completion. In some patients who underwent transient elastography (TE) (Fibroscan, Echosens SA, Paris, France), liver stiffness measurements were evaluated at baseline and 48-60 weeks after treatment completion.
Statistical analyses
Continuous variables are presented as means ± standard deviations (SD) or median (range). Categorical variables were presented as numbers of patients (%). The Student's t-test was used to analyze the continuous variables. The χ2 test was used to compare categorical variables.
Multivariate analysis was conducted for the risk factors of SVR12 failure using logistic regression analysis. Variables that showed a P value < 0.2 in the univariate analysis were included in the multivariate analysis. Paired t-test and Wilcoxon signed-rank test were used to compare continuous variables between baseline and 48–60 weeks after treatment completion. Statistical significance was accepted for P values of < 0.05. The analyses were performed using SPSS version 19.0 (SPSS, Chicago, IL, USA).
RESULTS
Prevalence of NS5A RAS
A total of 474 patients (men: 227; women: 247) were tested for NS5A RAS. Sixty-seven patients (14.1%) had baseline NS5A RAS (Y93 or L31). The proportion of NS5A RAS at positions Y93 and L31 was as follows: Y93H (56/67, 83.6%), L31M (3/67, 4.5%), L31F (3/67, 4.5%), Y93H with L31M/F/Y (2/67, 2.9%), Y93H with L31Y (1/67, 1.5%), Y93H with L31M (1/67, 1.5%), and Y93F (1/67, 1.5%). The most frequent NS5A RAS was Y93H (Fig. 2).

Baseline characteristics of the patients
The baseline characteristics of 288 patients who had confirmed HCV RNA testing at 12 weeks after treatment completion are shown in Table 1. Mean age of the patients was 55 ± 12 years, and 143 (49.7%) were men. Seventy-nine (27.4%) patients had liver cirrhosis and 218 (75.7%) patients were treatment-naïve (Table 1).
Table 1
Baseline characteristics

Data are expressed as mean ± standard deviation or number (%).
SVR = sustained virologic response, HCV = hepatitis C virus, ALT = alanine aminotransferase, AST = aspartate aminotransferase, APRI = aspartate transaminase to platelet ratio index, FI = fibrosis index, LSM = liver stiffness measurement, TE = transient elastography, HIV = human immunodeficiency virus.
Virologic response
The overall ETR rate was 98.3% (292/297) and a SVR12 rate of 96.5% (278/288) was achieved in patients who had confirmed HCV RNA testing 12 weeks after treatment completion. SVR12 failure comprised of 5 breakthrough and 5 relapsed patients. There was no difference in SVR12 rate between treatment-naïve patients and treatment-experienced patients (97.2% [212/218] vs. 94.3% [66/70], P = 0.239). There was no difference in SVR12 rate between patients without LC and patients with LC (97.6% [204/209] vs. 93.7% [74/79], P = 0.103) (Fig. 3).
Fig. 3
Virologic response at 12 weeks after treatment completion (SVR12).
SVR = sustained virologic response, Tx = treatment, LC = liver cirrhosis.

Characteristics of the patients who failed SVR12 are summarized in Table 2. Of the 10 patients who failed SVR12, 7 (70%) patients were women, 3 (30%) patients were over 70 years, 5 (50%) patients had liver cirrhosis and 6 (60%) patients were treatment-naïve. Six patients who were checked by NS5A RAS testing after treatment failure exhibited the presence of NS5A RAS, although baseline NS5A RAS was absent. Two patients were identified as dual NS5A RAS at L31 plus Y93 and 4 patients were identified as single NS5A RAS at L31 (n = 2) or Y93 (n = 2). There were no differences in baseline clinical and laboratory characteristics between patients with and without SVR12 (Table 1). Multivariate analysis were performed to determine the risk factor for SVR12 failure. However, there was no significant risk factor for SVR failure.
Table 2
Characteristics of patients who failed SVR12

Durability of SVR
Durability of SVR after achievement of SVR12 was analyzed in 191 patients who underwent HCV RNA testing at 48–60 weeks after treatment completion. Among them, only one patient showed no durability of SVR. Overall, 99.5% (190/191) of patients had durability of SVR. The patient who did not show durability of SVR was a treatment naïve 57-year-old man with baseline HCV RNA 7,360,113 IU/mL and non-LC. The patient underwent tattooing after achieving SVR12. The patient was not able to reconfirm the genotype after showing failure of durable SVR due to follow-up loss.
Improvement of liver function and fibrosis after achievement of SVR12 in patients who had durable SVR
In total patients (n = 190), there were significant improvements in total bilirubin level (0.9 ± 0.6 to 0.8 ± 0.4 mg/dL, P = 0.004), albumin level (4.1 ± 0.6 to 4.3 ± 0.4 g/dL, P < 0.001), and platelet count (169 ± 82 to 182 ± 72 × 103/mm3, P = 0.001) between baseline and 48–60 weeks after treatment completion. In addition, there were significant improvements in APRI score (1.4 ± 1.9 to 0.5 ± 0.5, P < 0.001), FIB-4 index (4.3 ± 4.9 to 2.4 ± 1.9, P < 0.001), and FI (2.4 ± 1.2 to 2.1 ± 1.2, P < 0.001). Although data of LSM on TE were available in only 41 patients, LSM (14.0 ± 10.0 to 9.6 ± 6.7 kPa, P = 0.001) was also improved between baseline and 48–60 weeks after treatment completion.
In patients with LC (n = 59), there were also improvements in total bilirubin level (0.9 [0.3–5.8] to 0.7 [0.2–2.7] mg/dL, P = 0.068), albumin level (3.8 [2.2–4.7] to 4.3 [2.4–4.9] g/dL, P < 0.001), and platelet count (99 [40–329] to 118 [40–399] × 103/mm3, P < 0.001) between baseline and 48–60 weeks after treatment completion. In addition, there were significant improvements in APRI score (1.8 [0.1–14.8] to 0.6 [0.1–4.8], P < 0.001), FIB-4 index (5.5 [0.6–32.8] to 3.3 [0.4–12.2], P < 0.001), and FI (3.2 [0.3–5.3] to 2.6 [0.2–4.9], P < 0.001). Although data of LSM on TE were available in only 16 patients with LC, LSM (17.2 [5.3–48.0] to 11.2 [3.7–28.1] kPa, P = 0.001) was also improved between baseline and 48–60 weeks after treatment completion (Fig. 4).
Fig. 4
Improvements in liver function and non-invasive fibrosis markers after 48–60 weeks of daclatasvir and asunaprevir treatment completion in patients with liver cirrhosis. Changes in liver function: (A) total bilirubin, (B) albumin, (C) platelet count, and non-invasive fibrosis markers: (D) APRI, (E) FIB-4 index, (F) FI, (G) LSM on TE. Data are presented as box plots, where horizontal line represents median value and box edges represent 25th and 75th percentiles.
APRI = aspartate transaminase to platelet ratio index, FI = fibrosis index, LSM = liver stiffness measurement, TE = transient elastography.

Safety assessment
The safety was assessed by a retrospective review of the medical records of 316 patients treated with DCV/ASV (Fig. 1). ALT elevations were observed in 5 patients during treatment. One of them had ALT elevation greater than 10 times the upper limit of normal. However, ALT elevation was improved after discontinuation of DCV/ASV combination therapy. Bilirubin elevations were observed in 2 patients and those were spontaneously normalized during treatment. Skin rashes were observed in 3 patients, of which one patient had grade 3 or higher and discontinued DCV/ASV combination therapy. Five patients showed symptoms of fatigue and 3 patients had headaches, however the degree of symptoms was mild (Table 3). Three patients developed HCC after achievement of SVR12, but no patients underwent liver transplantation. Two patients died after achieving SVR12, but mortality was not associated with HCV infection.
DISCUSSION
In this study, we observed that the combination treatment of DCV/ASV in patients with NS5A RAS negative resulted in a high virologic response and good durability. Treatment failure in patients with baseline RAS-negative may be associated with treatment-emergent RAS. In patients with liver cirrhosis who achieved SVR, improvements of liver function and non-invasive fibrosis markers at 48–60 weeks after treatment completion were observed.
Recently, multiple interferon-free, oral DAA regimens have become available for the treatment of chronic HCV infection. When selecting DAA regimens for HCV infection, viral genotype and subtype, presence of cirrhosis, and HCV treatment history should be considered. Furthermore, the presence of NA5A RAS is a well-known risk factor for DCV/ASV treatment failure in HCV GT1b-infected patients, compared with recently developed DAAs which are known to be effective regardless of RAS. In a previous clinical study of DCV/ASV treatment for HCV GT1b-infected patients, NS5A RAS positive was an important risk factor in SVR12 failure; NS5A RAS was confirmed in 12.6% of enrolled patients and SVR12 was obtained in 39% of NS5A RAS positive patients, whereas SVR12 was obtained in 92% of NS5A RAS negative patients.6 The prevalence of pre-treatment NS5A RASs has been reported as 6-16% using population sequencing (cut-off 15%–25%) or deep sequencing (cut-off 1%), and regional differences have been suggested.8 In a previous study, NS5A RAS at Y93H and/or L31M/V was detected in 11.8% of Asian patients and 4.8% of non-Asian patients.9 In recent Korean real-world data, 15.5% at Y93 and 5.6% at L31 were positive.10 In our study, 14.1% of patients (12.0% at Y93, 1.3% at L31, and 0.8% at Y93 and L31) were positive.
Because there is no insurance coverage for DCV/ASV treatment for HCV GT1b-infected patients with baseline NS5A RAS positive in Korea, virologic response for only RAS negative patients was confirmed in our study. Our results showed a higher SVR12 of 96.5% in patients with baseline NAS5A RAS negative than results from a global clinical trial (92%) or a Japanese real-life study (93.7%).611 Although there was no statistical difference, the virologic response was slightly lower in LC patients than non-LC patients, and was also lower in treatment-experienced patients than treatment-naïve patients. In addition to NS5A RAS, high baseline HCV RNA level, old age, and severe fibrosis were suggested as risk factors of DCV/ASV treatment failure.61213 However, our study did not show any significant association between these factors and treatment failure. Interestingly, NS5A RAS was detected in 6 patients who checked NS5A RAS testing after treatment failure among 10 treatment failure patients with baseline NAS5A RAS negative. The other 4 patients could not confirm whether the NS5A RAS appeared because they were lost during follow-up or did not consent to the test. From these results, the only cause of treatment failure may be the selection of NS5A RAS during treatment. A previous study also demonstrated that the RAS was confirmed by direct sequencing after treatment failure of DCV/ASV in patients with baseline RAS negative.1415 These results suggest that the virus with RAS, which was present in a minor portion within the range that could not be detected by commercial methods before treatment, was incompletely inhibited by DAA and the virus could remain selected.
In a meta-analysis of patients who had acquired SVR by IFN therapy, high SVR durability was reported.16 However, few studies have confirmed the long-term SVR durability in DAA treatment, due to the short history of DAA market. In our study, the treatment of DCV/ASV provided good SVR durability for 1 year after achievement of SVR12. HCV RNA at 1 year after achievement of SVR12 was detected in only one of the patients with SVR12. The cause of late relapse or reinfection in this patient was not clear, but it was confirmed that he got a tattoo after achievement of SVR12.
Liver fibrosis results from chronic liver injury and is characterized by excessive accumulation of extracellular matrix proteins.17 Its staging is critical for the clinical outcome of CHC patients.1819 Previous studies have demonstrated that the pre-treatment stage of fibrosis was an important risk factor for HCC development and mortality.20 Thus, a recent guideline recommends that HCC surveillance after achievement of SVR should be considered in patients with advanced fibrosis and cirrhosis.21 However, previous studies also suggested that liver fibrosis after achievement of SVR could be improved in patients who received IFN,52223 and the majority of patients with improved fibrosis after IFN treatment showed good clinical outcomes.5 On the other hand, there are few studies on the long-term changes of fibrosis after achievement of SVR in DAA treatment. Although liver biopsy has been widely regarded as the gold standard for the staging of liver fibrosis, the procedure has several limitations, including intra- and interobserver variability in histopathological interpretation, sampling errors and complications (i.e., bleeding). There have been various studies on the non-invasive evaluation of hepatic fibrosis in CHC patients, and the simple non-invasive fibrosis indices such as APRI, FIB-4, and FI, and LSM on TE were suggested as useful non-invasive markers for evaluation of hepatic fibrosis.2425 In a meta-analysis, the area under the receiver operating characteristic (ROC) curve (AUROC) of the APRI for the diagnosis of significant fibrosis (≥ F2 according to METAVIR), severe fibrosis (≥ F3), and cirrhosis in patients with CHC was 0.77, 0.80, and 0.83, respectively.26 In a previous study, the AUROC of FIB-4 for the diagnosis of severe fibrosis and cirrhosis was 0.85 and 0.91, respectively.27 The AUROC of FI for the diagnosis of significant fibrosis, severe fibrosis, and cirrhosis was 0.74, 0.72, and 0.91, respectively.25 The AUROC of LSM on TE for the diagnosis of significant fibrosis, severe fibrosis, and cirrhosis was 0.83, 0.90, and 0.95, respectively.28 Additionally, Vergniol et al.24 suggested that fibrosis stages measured by non-invasive fibrosis markers were related to clinical outcomes in patients with CHC. In our study, patients with LC showed a significant improvement of APRI, FIB-4 index, FI and LSM on TE one year after achievement of SVR12 compared with pre-treatment, and the albumin level was also significantly improved. Although the long-term clinical outcomes of the treatment with DCV/ASV could not be evaluated due to the short-term follow-up period in real-world, these results suggest that the achievement of SVR after treatment with DCV/ASV might predict a good prognosis in CHC patients.
There are several limitations in this study. First, as a retrospective study, there is a possibility of selection bias and difficulties in reviewing safety profiles. Second, liver fibrosis status could not be compared with the histologic results. There is still some debate over whether the changes of non-invasive fibrosis markers after antiviral treatment can reflect histological changes of liver fibrosis.29 In addition, non-invasive fibrosis markers may be also overestimated by abnormal serum levels of aminotransferases.30313233 To overcome this limitation, we evaluated the changes of various non-invasive fibrosis markers and confirmed that all non-invasive fibrosis markers were improved after DCV/ASV treatment. Third, deep sequencing was not performed in the RAS test. If deep sequencing for RAS test was performed before treatment, RAS, which was confirmed after treatment failure, might have been detected before treatment. Finally, this study used relatively old DAA (DCV/ASV) compared to new highly effective DAAs that do not need RAS test. However, the durability of SVR and fibrosis improvement in DCV/ASV treatment can be generalized to the effect of other new DAAs.
In conclusion, the treatment with DCV and ASV can be expected to have a high efficacy and improve liver fibrosis if administered only to patients with RAS negative. However, RAS, which was not detected in pre-treatment, may appear during treatment and lead to treatment failure.
 XML Download
XML Download