

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cavernous hemangioma of the gallbladder is an extremely rare benign tumor (1). Hemangioma occurs in several organs, including the liver, brain, lungs and skeletal muscle. It is the most common benign tumor in the liver, in which cavernous hemangioma represents the majority of tumors (23). Gallbladder hemangioma has only been reported in nine cases in literature, and the pathophysiology is unclear.
In previous literature, ultrasound, endoscopic ultrasonography, contrast-enhanced computed tomography (CT) and angiography were reported to be useful for the diagnosis of hemangioma. However, the differentiation of hemangioma from cancer of the gallbladder was challenging. Moreover, there are no reports of gallbladder hemangioma focusing on the findings of MRI.
This study reports the radiological findings focusing on MRI and literature review of an extremely rare case of cavernous hemangioma of the gallbladder.
CASE REPORT
A 53-year-old male patient was referred to our hospital for further evaluation of incidental finding of a nodular lesion abutting the gallbladder on screening chest CT. The patient had no associated medical history and was asymptomatic. There was no tenderness or rebound tenderness observed over the right upper abdomen on physical examination, and the patient was afebrile. The laboratory data were within normal limits: leukocyte count of 4.9 × 103/µl; C-reactive protein (CRP) 0.25 mg/dL; total bilirubin 0.8 mg/dL; and cancer antigen 19-9 (CA19-9) 3.36 U/mL (reference value: 0–37).
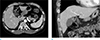
The chest CT showed a 1.8 cm, well-defined, mild enhancing nodular lesion with peripheral nodular enhancement abutting to the body of the gallbladder (Fig. 1a, b). Transabdominal and endoscopic ultra-sonographies demonstrated an oval isoechoic nodular lesion with a slightly hyperechoic rim (Fig. 2a, b). The color Doppler examination did not reveal blood flow in the mass (Fig. 2c). On MRI (Achieva 3T, Philips Healthcare, Best, the Netherlands), the gallbladder lesion showed a homogeneous high signal intensity on the T2-weighted images (Fig. 3a). The lesion had a high signal intensity on a diffusion weighted image (DWI) with a high b-value (500 s/mm2) and slightly lower value on the apparent diffusion coefficient (ADC) map (Fig. 3b, c). The contrast enhanced dynamic images, using Gd-EOB-DTPA (Primovist, Bayer Schering Pharma AG, Berlin, Germany), showed a small nodular lesion with peripheral nodular and centripetal progressive enhancement (Fig. 3d–g). No significant wall thickening was observed in the body of the gallbladder abutting the nodular lesion. Gallstone or enlarged lymph nodes were not identified. The possibility of a sub-epithelial tumor of the gallbladder, gallbladder duplication with chronic inflammation, and metastatic lymphadenopathy were considered.
A laparoscopic cholecystectomy was performed because of the high possibility of a malignant tumor or metastatic lymphadenopathy. Intraoperatively, a dark reddish nodular lesion protruding from the body of the gallbladder was observed, which appeared to be completely covered with connective tissues (Fig. 4a). The gross specimen showed a 2.0 × 0.8 cm, well-defined tumor located at the sub-serosal perimuscular connective tissue layer of the gallbladder (Fig. 4b). There was no direct connection between the tumor and adjacent liver on examination of the operative and gross specimens. The cut surface showed a typical spongiform pattern of cavernous hemangioma. The histopathological findings showed blood within enlarged blood vessels, which were lined by endothelium without atypia (Fig. 4c). The gallbladder nodular lesion was then diagnosed as cavernous hemangioma.
DISCUSSION
Cholesterol polyps, adenoma and adenomyoma are the most common benign tumors of the gallbladder (4). Hemangioma is the most common tumor in the liver. However, it rarely occurs in the gallbladder. Only nine cases have been reported in past literature (123).
The pathological types of hemangiomas are cavernous, capillary, venous and arteriovenous (1). In past literature, nine cases of gallbladder hemangioma have been reported. Among these, seven cases were diagnosed as cavernous hemangioma, one as venous, and another as a case of arteriovenous hemangioma (125). Similar to those of the liver, majority of the hemangiomas of the gallbladder are also cavernous hemangiomas (3). The present case of gallbladder tumor was also a cavernous hemangioma. The pathophysiology of gallbladder hemangiomas is unclear. However, two hypotheses have been proposed. One hypothesis suggests hamartomatous proliferation of the connective tissue elements normally present in the gallbladder wall. On the other hand, the other proposes a congenital origin of the lesion, arising from the proliferation of embryonic mesodermal tissue elements sequestrated in the sub-serosal layer of the gallbladder wall (15).
Symptoms reported in the previous studies ranged from asymptomatic to mild or severe abdominal pain, and mostly occurred in adult males (12). The location of the hemangioma is variable. However, the most commonly reported site is the fundus of the gallbladder (1). Identifying the organ of origin is challenging through preoperative imaging studies. This is particularly true of gallbladder lesions on the hepatic surface, which can be misdiagnosed as hepatic tumor (15).
Imaging features of hepatic hemangioma are well known in various imaging modalities. On contrast-enhanced dynamic CT and MRI images, the hepatic hemangiomas typically show peripheral nodular enhancement with centripetal progression. T2-weighted MRI show marked high signal intensity (3). To the best of our knowledge, there are no reports of MRI findings of cavernous hemangioma of the gallbladder. In this study, CT and MRI showed similar images that were characteristic features of hepatic hemangioma.
Hemangioma is a benign disease and it is important to distinguish the lesion from malignant tumors of the gallbladder. The most common malignant tumor is the gallbladder carcinoma. Gallbladder cancer is a tumor originating from the mucosal epithelium. It appears as a thickening of the mucosal layer or protruding polyp into lumen on imaging studies. The presence of irregular thickening of the mucosa may be helpful in differentiating carcinoma of the gallbladder from hemangioma (67). The second most common malignancy is the metastatic tumor that originates from malignant melanoma, gastric, renal and lung cancers. Metastatic cancer of the gallbladder usually shows infiltrative and persistently enhancing thickening of the wall or an early strong enhancing nodule on CT or MRI. The presence of primary carcinoma and pattern of enhancement can aid in distinguishing metastatic tumor from hemangioma (8). Focal adenomyomatosis of the gallbladder can be seen as a well-defined mass in the fundus. The finding of the intramural foci of high signal intensity on the T2-weighted MRI, known as “string of beads” sign, is highly specific in the diagnosis of gallbladder adenomyomatosis (7). The majority of the sub-epithelial tumors originating from the mesenchymal tissue of the gallbladder are sarcoma. Therefore, benign tumors of the gallbladder sub-epithelial tumor are very rare. Among the benign tumors of the gallbladder, the granulosa cell tumors are the most common ones. A few cases of leiomyoma and gastrointestinal stromal tumor (GIST) have been reported (9). In the case of a duplicated gallbladder, magnetic resonance cholangiopancreatography can be distinguished from a hemangioma (10).
In conclusion, the possibility of gallbladder hemangioma, although rare, must be considered if a well-defined subepithelial tumor of the gallbladder shows peripheral nodular enhancement with centripetal progression on delayed contrast-enhanced study and homogeneous high signal intensity on the T2-weighted image of MRI.



 XML Download
XML Download