

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Revascularization for intermediate coronary stenosis (defined as 50% to 70% stenosis by quantitative coronary angiography) has been still under debate due to the limitations of coronary angiography itself. Coronary angiography, which evaluates lesions based on projection images, often under- and overestimates a lesion's severity because of contrast-dependent coronary dilation, high interobserver variability and poor ability to analyze plaque characteristics, especially in intermediate lesion.1)2)3) Current guidelines recommend the use of fractional flow reserve (FFR) and intravascular ultrasound (IVUS) to guide and optimize revascularization in intermediate coronary lesion.1)4)5)
FFR measurement is generally used as index for the functional severity of coronary artery stenosis, and well known as modality to decide whether to proceed with percutaneous coronary intervention (PCI) or defer in stable coronary disease.6)7) On the other hand, IVUS has been widely used to optimize for PCI and assess accurate stenotic lesion and stent implantation.8) The use of FFR and IVUS has been associated with improved clinical and procedural outcomes.9)10) In Korea, FFR measurement has been covered by the national insurance system under some limited cases like an intermediate lesion. However, it was not well known about contemporary patterns of FFR and IVUS among patients undergoing PCI in Korea. We aimed to investigate the current status of intervention using FFR and IVUS for intermediate stenotic lesions from Korean percutaneous coronary intervention (K-PCI) registry.
METHODS
We analyzed the K-PCI registry, as a retrospective multicenter registry, that collected a standardized database for PCI case analysis of the participating 92 hospitals throughout the country from January 1, 2014, through December 31, 2014. Two reports of the K-PCI registry have already been published in the Korean Circulation Journal.11)12) We excluded 17,295 patients with acute myocardial infarction from the original registry data (44,967 patients), and analyzed 27,672 patients who underwent PCI under angiography-only, FFR-, or IVUS-guidance. Demographic characteristics, medical history, procedural data and PCI related complications in hospital were collected retrospectively using case report forms (CRFs). All variables corresponded with written definitions in the CRF dictionary to standardize the data, as detailed in the previous article (K-PCI registry 2014 CRF, Supplementary Table 1 in the online-only data Supplement).11)
The local Institutional Review Board (IRB) at each participating center approved this study. The informed consent document was waived at all center, considering retrospective enrollment of the study, without clinical follow-up. Data were collected using a web-based reporting system.
We classified enrolled patients to 3 groups according to intervention approach, such as angiography-only, IVUS and FFR. When both IVUS and FFR were used, those cases were considered to be FFR groups. The centers that were equipped with FFR device accounted for about 77.1% among the K-PCI registry. We divided enrolled patients according to the severity of diameter stenosis (<50%, 50–69%, and ≥70%), the use of devices (IVUS and FFR). Intermediate coronary stenosis was defined as 50% to 70% narrowing of coronary artery in this registry, considering stenotic severity range (50–70%) for reimbursements by National Health Insurance (NHI) about FFR measurement. The reimbursement in our country only would cover as follows: 1) to evaluate the need of PCI in case which intermediate coronary stenosis of 50–70% by quantitative coronary angiography (QCA) was confirmed in patients who have multivessel disease or more than two lesions in the same artery, 2) to evaluate the need of additional PCI for the side branch after the stent insertion at the main branch. We investigated the rates of coronary intervention and the use of FFR device according to the target vessels, lesion severity, and the presence or absence of FFR device. In-hospital clinical outcomes before discharge were also analyzed.
Continuous variables are presented as mean±standard deviation and compared using Student's t-tests or analysis of variance (ANOVA). Categorical variables are summarized as counts and percentages and compared using the chi-square test or Fisher's exact test, as appropriate. All statistical analyses were conducted with R version 3.3.2 (R foundation for Statistical Computing, Vienna, Austria). A 2-sided p-value of <0.05 was considered statistically significant.
RESULTS
The mean age was 65.8±10.7 years and 68.0% were male in this study, as shown in Table 1. Hypertension was the most common concomitant medial history (66.0%), followed by dyslipidemia (44.5%) and diabetes mellitus (38.0%). Unstable angina (57.8%) was more common than stable angina (36.6%) as clinical indication for PCI. FFR was used in 1,419 cases (5.1%) and IVUS was used in 8,206 cases (29.6%) among all coronary lesions in K-PCI registry.
Table 1
Baseline patient and clinical characteristics

Values are presented as number (%), or mean±SD.
CABG = coronary artery bypass graft; CAD = coronary artery disease; CKD = chronic kidney disease; CT = computed tomography; CVD = cerebrovascular disease; ESRD = end-stage renal disease; FFR = fractional flow reserve; FHx = family history; GFR = glomerular filtration rate; IVUS = intravascular ultrasound; KTP = kidney transplant patients; MI = myocardial infarction; MR = magnetic resonance; PAD = peripheral arterial disease; PCI = percutaneous coronary intervention; SD = standard deviation.
*GFR ≤60mL/min/1.73m2.
Most of procedure were conducted in elective cases (89.8%). Left anterior descending artery (LAD, 40.6%) was the most commonly detected coronary vessel, followed by right coronary artery (RCA, 34.3%) and left circumflex artery (LCX, 28.2%). Mean number of stents implanted was 1.3±0.8, and trans-radial approach (65.5%) was performed more frequently than trans-femoral approach (36.2%) (Table 2).
Table 2
Baseline angiographic and procedural characteristics

Values are presented as number (%), or mean±SD.
DES = drug-eluting stent; FFR = fractional flow reserve; IVUS = intravascular ultrasound; LAD = left anterior descending artery; LCX = left circumflex artery; p-LAD = proximal left anterior descending artery; PCI = percutaneous coronary intervention; RCA = right coronary artery; SD = standard deviation.
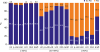
The rates of PCI for intermediate lesions in left main artery (LM) (32.3%) and LAD (18.1%) were relatively higher than RCA (8.2%) and LCX (7.5%), as shown in Figure 1 (detailed in Supplementary Table 1). On the other hand, the incidence of deferring PCI for significant lesion with stenosis >70% was highest in LCX (32.5%), followed by RCA (23.4%), LM (20.2%), LAD (21.1%), except graft. Especially, the rates of PCI for proximal LAD was relatively higher than other coronary vessel of all stenotic severity.
Figure 1
Comparison of PCI rates for coronary vessels according to stenotic severity.
LAD = left anterior descending artery; LCX = left circumflex artery; LM = left main artery; p-LAD = proximal left anterior descending artery; PCI = percutaneous coronary intervention; RCA = right coronary artery.
The rate of FFR and IVUS measurement in intermediate lesion performed PCI was respectively 11.5% and 32.6%. The rates of using FFR in intermediate lesion was low in the hospitals with FFR device (16.8% for LAD, 13.2% for RCA, 12.2% for LM, and 9.8% for LCX) (Figure 2, detailed in Supplementary Table 2). The rates of using IVUS in intermediate lesions, even in FFR-present group, was higher than the rate of using FFR in all coronary vessels (52.1% vs. 12.2% for LM, 27.4% vs. 16.8% for LAD, 32.1% vs. 9.8% for LCX, and 33.9% vs. 13.2% for RCA). And also, the rate of PCI in intermediate lesion was higher in the FFR-present group than in the FFR-absent group, especially in LM (40.9% vs. 5.9%) and LAD (20.8% vs. 6.0%) (Figure 3, detailed in Supplementary Table 3).
Figure 2
Use of adjunctive PCI tools according to the availability of FFR.
FFR = fractional flow reserve; FFR(+) = Hospitals that were equipped with FFR device; FFR(−) = Hospitals that were not equipped with FFR device; IVUS = intravascular ultrasound; LAD = left anterior descending artery; LCX = left circumflex artery; LM = left main artery; p-LAD = proximal left anterior descending artery; PCI = percutaneous coronary intervention; RCA = right coronary artery.

Figure 3
Comparison of PCI rates according to availability of FFR.
FFR = fractional flow reserve; FFR(+) = Hospitals that were equipped with FFR device; FFR(−) = Hospitals that were not equipped with FFR device; IVUS = intravascular ultrasound; LAD = left anterior descending artery; LCX = left circumflex artery; LM = left main artery; p-LAD = proximal left anterior descending artery; PCI = percutaneous coronary intervention; RCA = right coronary artery.

There was no significant difference in composite in-hospital clinical outcomes among three groups, as shown in Table 3. However, non-fatal myocardial infarction (MI) was more frequently occurred in the FFR group than other groups (0.3% vs. 1.0% vs. 1.6%, p<0.001). And also, the rates of death and transfusion were significantly different between 3 groups.
Table 3
In-hospital outcomes

DISCUSSION
The major findings of our study are as follows: 1) the rate of FFR measurement among non-acute MI patients who performed PCI was relatively low (5.1%); 2) PCI was more frequently performed using IVUS than using FFR in intermediate lesion (32.6% vs 11.5%); 3) regardless of whether FFR is used or not, PCI for intermediate lesion was more frequently performed in the hospitals with available FFR device than without it; and 4) there were no significant differences in in-hospital clinical outcomes such as cardiac death, stent thrombosis, and stroke among angiographic-guided vs IVUS-guided vs. FFR-guided PCI groups.
The rate of FFR measurement in intermediate lesions among PCI cases in our K-PCI registry, even though it did not have deferred-PCI cases, was quite low (11.5%). Despite a significant increase in the use of FFR and IVUS according to the national database13) and data from the registry,14) FFR was only performed in 3.7% of patients (2.5% in ACS patients, 7.2% in non-ACS patients) according to the original report of the 2014 K-PCI registry.11) Prolonged procedure time due to catheter reinsertion, the use of drug like adenosine, high cost of catheter, and poor reimbursement could be considered as factors that can be considered as causes for the low rates of FFR use.15) The low rates of FFR use was similarly observed in other country, 6.1% in US (among 61,874 attempted PCI for intermediate lesion between April 2009 and September 2010) and 8.2% in Japan.15)16) There might have been more obstacles in using the FFR for intermediate coronary lesions due to strict national insurance coverage than in Japan, where application for national insurance coverage is relatively easy. Interestingly, we also found that PCI for intermediate lesion was more frequently performed in all coronary lesions in the hospitals equipped with FFR device with or without FFR guidance, compared with the hospitals without FFR device. As the most important factor of this result, the difference in cardiovascular center size (high- vs. low-volume centers) could be considered. Previous study using K-PCI registry reported that the low-volume centers had fewer patients with stable coronary disease, and performed less elective PCI and more frequently urgent/emergency PCI for patients with ACS than high-volume centers.11) The differences in centers volume, clinical indication for PCI, and composition of patients may have caused the difference in the rates of PCI for intermediate lesions. However, this analysis is not powered to draw definitive conclusion, and additional research would be needed to elucidate the factors responsible for differences between high- vs. low-volume centers.
The rate of IVUS use was higher than that of FFR in coronary intervention for intermediate lesion (32.6% vs. 11.5%) in K-PCI registry, similar to data from National Cardiovascular Data Registry in US (20.3% vs. 6.1%).15) Optimization of PCI using IVUS has been well known to improve clinical outcomes compared to angiography-only guided PCI.10)17)18) However, IVUS guided PCI may not help to decide whether to proceed PCI, but for optimization of PCI. IVUS-derived minimal lumen area (MLA), which can be used as an indicator of functionally significant stenosis, had a relatively low positive predictive value, and use of IVUS-derived MLA to guide PCI may result in unnecessary or inappropriate PCI.19)20) And, mean MLA cut-off value was different by ethnicity between Asians and Westerners, maybe due to lower body mass index and smaller myocardial masses in Asian people.21)22)
Unlike angiography- or IVUS-guided anatomical approach, physiologic approach using FFR measurement in intermediate lesions could be used as an accurate indicator to guide and proceed PCI. FFR-guided PCI improved clinical outcome when compared with angiography-guided PCI or medical therapy alone, during long-term follow-up.9)23)24)25) Furthermore, use of FFR could reduce unnecessary or inappropriate PCI without any disadvantages, and ensure economic efficiency by reducing medical cost related to PCI.16)26)27) Previous study related to PCI for intermediate coronary lesion reported that clinical outcomes were not different between FFR-guided vs. IVUS-guided PCI and FFR-guided PCI reduced the need for revascularization (FFR vs. IVUS; relative risk, 0.02).28) In our study, we could observe relatively higher use of FFR in LAD compared with other vessels (16.8% for LAD, 13.2% for RCA, and 9.8% for LCX). Physicians might have concerned about a higher association of LAD stenosis with heart failure and poor prognosis as previously reported.22)25) Based on clinical importance and lots of clinical data for FFR-guided physiologic approach PCI, current guidelines recommended FFR measurements before PCI in patients with stable coronary artery disease.5)29)
Composite in-hospital clinical outcome in our K-PCI registry was not significantly different among angiographic-guided vs IVUS-guided vs. FFR-guided PCI groups. Even though the rate of clinical outcomes such as death, nonfatal MI, and transfusion had significant difference; we think this might be explained by extremely large disparity in the number of cases between the 3 groups (angiographic-guided group: 18,047, IVUS-guided group: 8,206, and FFR-guided group: 1,419). Originally, this study is retrospective, cross-sectional study, and was not designed for randomized comparison of FFR-vs. image-guided PCI of intermediate lesions. Furthermore, data on specific causes and timing for death and transfusion at each 92 hospitals could not be uniformly verified in this registry. Nevertheless, our study is the first analysis about real-world pattern of PCI with the use of FFR and IVUS for intermediate coronary lesion from the nationwide standardized database by K-PCI registry. Although results of our study did not show improvement in the clinical outcomes or reduction of complication, we think our study might suggest what to supplement and what to do for improvement of clinical outcomes, by presenting current status of PCI and obstacles to use FFR device. Meanwhile, nonfatal MI was higher in IVUS-guided and FFR-guided group than angiographic-guided group. Possible mechanism for this difference could be explained by transient increase of cardiac marker that was caused by manipulation of adjunctive device, or prolonged procedure time.
There are several limitations to be addressed in our study that should be considered when interpreting the results. First, even though the K-PCI registry is the largest PCI registry in Korea, these results represent only those patients treated in 92 high volume hospitals, not all patients who underwent PCI in Korea. Also, the rate of FFR or imaging studies might be underreported due to the absence of data for the patients who underwent only diagnostic angiography with those studies. Second, this registry had only in-hospital clinical outcomes before hospital discharge. It was limited to evaluate long-term clinical effect according to use of IVUS or FFR in intermediate lesion. Further long-term follow-up study would be needed to evaluate the effect of adjunctive device such as FFR and IVUS. Third, because this study used a multicenter retrospective registry, procedural features may have influenced by uncontrolled variable factors in terms of diversity of operator in different region or different hospitals. Fourth, because this K-PCI registry is a database for PCI case which was performed on 92 hospitals, the FFR-guided deferred cases are not included in this study. Finally, there are no data regarding exact timing of IVUS examination in the IVUS-guided group.
In conclusion, these data may provide the current PCI practice pattern with the use of FFR and IVUS in intermediate lesion. To reduce unnecessary PCI and help to decide whether to proceed PCI, more common use of FFR for intermediate lesion should be encouraged.
 XML Download
XML Download