

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Periprocedural myocardial infarction (MI) increases the risk of major adverse cardiac events including mortality.1)2)3)4) An important cause of periprocedural MI is microvascular damage due to distal embolization during percutaneous coronary intervention (PCI).5)6) Periprocedural MI during PCI has been reported to range from 15–70% of cases, which depends on diagnostic modalities and definitions used.3)7) Plaque composition and morphology is closely related to distal embolization during PCI. Attenuated plaque on grayscale intravascular ultrasound (IVUS), thin-cap fibroatheroma (TCFA), necrotic core (NC) on virtual histology (VH)-IVUS and cap thickness on optical coherence tomography (OCT) are related to periprocedural MI.3)8)9)10)
The lipid core burden index (LCBI) measured using near-infrared spectroscopy (NIRS) can assess plaque vulnerability. Previous studies have demonstrated that pre-PCI LCBI was related with periprocedural MI indicated by cardiac enzyme elevation, and is related to poor clinical outcomes.11)12) However, there is no study on the relationship between LCBI measured with NIRS and microvascular dysfunction assessed using invasive coronary physiology. Microvascular dysfunction can be easily measured during PCI using a pressure wire. The index of microcirculatory resistance (IMR) is a pressure-derived index, which can assess microvascular dysfunction and has high reproducibility and reliability, independent of hemodynamic changes.13)
We aimed to evaluate the relationship between LCBI measured with NIRS and microvascular dysfunction during PCI invasively assessed using IMR.
METHODS
Study population
From February 2015 to July 2016, we enrolled 39 patients who underwent elective PCI with a drug-eluting stent (DES). This study is pilot retrospective study with an exploration study of observational finding. Inclusion criteria were silent ischemia, stable or unstable angina, and age 18–80 years. Exclusion criteria were a lesion in an infarct-related artery, left main disease, a restenosis lesion, graft vessel lesion, chronic total occlusion lesion, and a low ejection fraction (<40%). Cardiac enzyme elevation was defined as creatine kinase-MB (CK-MB) elevation ≥3 times of the upper reference limit, and cardiac troponin-I elevation was defined according to the Society for Cardiovascular Angiography and Interventions (SCAI) definition.14) The study protocol was approved by the Institutional Review Board (AJIRB-MED-MDB-17-235) and informed consent was obtained from the patients.
Quantitative coronary angiography
The Cardiovascular Angiography Analysis System II (Pie Medical, Maastricht, the Netherlands) was used for quantitative coronary angiography (QCA) analysis. Before and after PCI, the percentage diameter stenosis (DS), minimal luminal diameter (MLD), reference vessel diameter, and lesion length were measured and calculated.
Intravascular ultrasound and near-infrared spectroscopy
IVUS was performed after intracoronary administration of nitroglycerin, using a 3.2-Fr exchange catheter, which is a rotation and pullback device (Infrared, Burlington, Massachusetts). The catheter was advanced distally as far as possible in the target vessel followed by automatic pullback at 0.5 mm/sec. The NIRS system has been previously described.11) LCBI is calculated as a fraction of yellow pixels measured from the chemogram multiplied by 1,000. The maximum value of LCBI for any of the 4-mm segments at the culprit lesion (culprit LCBI4mm) is obtained and represents lipid core plaque. A previous study showed that LCBI4mm ≥500 before PCI was related to periprocedural MI indicated by cardiac enzyme elevation.11) Accordingly, we divided the patients into 2 groups using a cutoff value of culprit LCBI4mm ≥500, as high or low LCBI group. Off-line IVUS and NIRS analyses were performed by an independent physician blinded to the IMR value. All IVUS analyses were performed according to the American College of Cardiology clinical expert consensus document on standards for acquisition, measurement, and reporting of IVUS studies.15)
Coronary physiology measurement
Coronary pressure measurement was performed pre- and post-PCI using a 0.014-inch pressure wire (PressureWire, Radi Medical System; Abbott, Chicago, IL, USA). FFR was calculated by dividing the mean distal coronary pressure (Pd) by mean proximal arterial pressure, during maximal hyperemia. After successful DES implantation, IMR and coronary flow reserve (CFR) were measured simultaneously using a thermodilution technique as previously described.13)16) IMR was calculated as the Pd at maximal hyperemia divided by the inverse of hyperemic mean transit time (Tmn). CFR was calculated as resting Tmn divided by hyperemic Tmn. Microvascular dysfunction defined as a post-PCI IMR ≥25 U.17) Maximal hyperemia was induced with continuous intravenous adenosine infusion (140 μg/kg/min).
Statistical analysis
Categorical variables were presented as percentage and continuous variables were presented as mean±standard deviations. To test normal distribution, we performed Kolmogorov-Smirnov test. Continuous variables were compared using the unpaired t-test or Mann-Whitney U test and categorical variables were compared using the χ2 test or Fisher exact test. The correlation between LCBI and physiologic parameters was assessed using Spearman correlation. All statistical analyses were performed using SPSS software (version 20.0; SPSS Inc., Chicago, IL, USA). A p value of <0.05 was considered statistically significant.
RESULTS
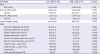
Baseline clinical characteristics are shown in Table 1. We enrolled 39 patients, and their mean age was 60±10 years. Patients with stable angina were 12 (31%), and those with unstable angina were 20 (51%). Diabetes was present in 9 (23%) patients. The most common target vessel was the left anterior descending artery (95%).
Table 1
Baseline clinical characteristics (n=39)

![]()
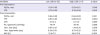
Baseline QCA and IVUS findings are summarized in Table 2. There were no differences in MLD and DS before and after PCI between the 2 groups. IVUS results showed that the low LCBI group had a larger proximal reference lumen area (12.5±4.6 vs. 9.7±1.7 mm2, p=0.012), and had a tendency for larger post-PCI minimal stent area (7.1±2.1 vs. 5.4±1.7 mm2, p=0.056). However, there was no difference in the IVUS area stenosis after PCI between 2 groups (32±13% vs. 37±17%, p=0.376). Mean value of culprit LCBI4mm was 333±196 before PCI and 119±137 after PCI. The delta LCBI defined as the difference between culprit LCBI4mm before and after PCI was higher in the high LCBI group (174±125 vs. 389±201, p=0.001).
Table 2
Coronary angiography and IVUS results (n =39)
Values are mean±standard deviation or number (%).
IVUS = intravascular ultrasound; QCA = quantitative coronary angiography; RVD = reference vessel diameter; DS = diameter stenosis; LA = lumen area; LCBI = lipid-core burden index; culprit LCBI4mm = maximum value of LCBI for any of the 4-mm segments at the culprit lesion; MLD = minimal luminal diameter; PCI = percutaneous coronary intervention; VA = vessel area; ΔLCBI = the difference of culprit LCBI4mm before and after PCI.
![]()
Coronary physiology study results are shown in Table 3. Pre-PCI FFR and post-PCI FFR (0.87±0.05 vs. 0.86±0.04, p=0.640) were not different between the 2 groups. The mean value of post-PCI IMR was 20±14 U. Post-PCI IMR was higher (15.6±7.3 vs. 42.6±17.6 U, p<0.001), and post-PCI CFR was lower in the high LCBI group (3.7±2.2 vs. 2.1±1.0, p=0.029) (Fig. 1). High LCBI group had longer mean hyperemic transit time (0.20±0.10 vs. 0.57±0.25 sec, p=0.001), but the Pd was not different between the 2 groups (79±14 vs. 79±18 mmHg, p=0.928) (Table 3). Pre-PCI culprit LCBI4mm had a negative correlation with post-PCI CFR (ρ=−0.494, p=0.001) and a positive correlation with post-PCI IMR (ρ=0.358, p=0.025) (Fig. 2).
Table 3
Coronary physiology study results
Values are mean±standard deviation.
CFR = coronary flow reserve; IMR = index of microcirculatory resistance; FFR = fractional flow reserve; LCBI = lipid-core burden index; Pa = proximal arterial pressure; Pd = distal coronary pressure; Tmn = mean transit time.
![]()
 | Figure 1Comparison of physiologic parameters. The mean value of post-PCI IMR was higher (15.6±7.3 vs. 42.6±17.6 U, p<0.001) and post-PCI CFR was lower in high LCBI group (3.7±2.2 vs. 2.1±1.0, p=0.029).CFR = coronary flow reserve; IMR = index of microcirculatory resistance; LCBI = culprit lipid-core burden index; PCI = percutaneous coronary intervention.
|
 | Figure 2Correlation between pre-intervention LCBI and physiologic parameters.CFR = coronary flow reserve; IMR = index of microcirculatory resistance; LCBI = culprit lipid-core burden index; PCI = percutaneous coronary intervention.
|
The incidence of microvascular dysfunction was more common in the high LCBI group (9.4% vs. 85.7%, p<0.001). However, there were no significant differences in the incidence of CK-MB elevation (9.4% vs. 14.3%, p=0.563) and troponin-I elevation (12.5% vs. 14.3%, p=1.000) based on the SCAI procedural MI definition.
DISCUSSION
This study showed that a high lipid-rich plaque as assessed using NIRS is related to post-PCI microvascular dysfunction, and has a fair correlation with post-PCI IMR and CFR, as assessed using a pressure wire.
Periprocedural MI increases the risk of major adverse cardiac events.1)2)3)4) Distal embolization of the plaque and/or thrombus is an important cause for the development of periprocedural MI, and it leads to impairment of microvascular perfusion at the tissue level.2)3)5) Since plaque dissection or redistribution occurs during PCI, the vulnerable plaque is more easily redistributed and embolized to the distal vessel or to a side branch.18) Hence, plaque composition and morphology are closely related to distal embolization of plaque debris during PCI.
Previous studies evaluated the relationship between plaque characteristics and periprocedural MI using different invasive imaging modalities. In grayscale IVUS, an attenuated plaque was related to deterioration in the coronary blood flow after PCI.8) Using VH-IVUS, TCFA and high NC, increased the risk of periprocedural MI.3)19) The OCT study showed that the presence of OCT-defined TCFA could predict periprocedural MI.10)
NIRS is a novel imaging technique that illuminates the tissue with near-infrared light. Since the absorbance spectrum reflects the chemical makeup of the imaged tissue, it is a very effective method to detect a lipid-rich plaque.3)20)21) The LCBI measured with NIRS can assess plaque vulnerability, and a recent study has demonstrated that higher LCBI increases the risk of major adverse cardiac events. Every 100 units increase in culprit LCBI4mm was associated with a 19% increase in death, non-fatal acute coronary syndrome, or unplanned revascularization during 4 years of follow-up.12) Goldstein et al.11) reported that periprocedural MI identified by cardiac enzyme elevation is more frequent in a patient with a large lipid plaque using a cutoff value of culprit LCBI4mm ≥500 in NIRS. We divided the patients using this cutoff value as a reference. In addition, the receiver operating characteristic curve analysis using our study population showed a similar result. The best cutoff value for culprit LCBI4mm to predict microvascular dysfunction (IMR >25 U) was >488 with a sensitivity of 67%, specificity of 97%, and accuracy of 87%. Using a cutoff value of culprit LCBI4mm ≥500, the incidence of microvascular dysfunction after PCI is more frequent in high LCBI group. Besides the absolute value of culprit LCBI4mm before PCI, the delta LCBI was higher in high LCBI group, which might reflect more plaque redistribution and embolization during PCI in this group.
The strength of our study is the use of IMR to assess microvascular dysfunction. Usually, periprocedural MI is evaluated using cardiac enzyme elevation after PCI. However, the reported incidence has a wide range, several different definitions, and measured cardiac enzyme at different time points. Moreover, cardiac enzyme elevation cannot specifically identify the origin, as to whether it is related with a target lesion or other vessels or a patient level.4)14)22) In contrast, the IMR is a reliable method for assessing coronary microvasculature at the target vessel territory. It has a significantly good correlation with true microvascular resistance, good reproducibility and lesser dependence on hemodynamic parameters including heart rate, contractility, and blood pressure.13)23)
A previous study reported the usefulness of IMR in evaluating periprocedural MI. Cuisset et al.24) reported that a patient treated with direct stenting had significantly lower IMR compared to conventional stenting. A VH-IVUS study showed that the IMR significantly increased after PCI in patients with TCFA compared with non-TCFA.9) In the current study as well, besides the incidence of microvascular dysfunction, the mean value of IMR was higher in high LCBI group. The difference in IMR between the high and low LCBI group results from the difference in hyperemic Tmn. There was no difference in coronary distal pressure between the 2 groups; however, hyperemic Tmn was significantly longer in the high LCBI group indicating increased microvascular resistance in this group. Moreover, the mean value of post-PCI CFR, which is another parameter reflecting microvascular dysfunction, was lower and the incidence of CFR ≤2 was numerically higher (57% vs. 22%, p=0.08) in the high LCBI group. Although CFR has limitations in that it is not specific for microvascular function and has a high variability with hemodynamic changes compared to IMR, our CFR result indicates that a high lipid-rich plaque was related to post-PCI microvascular dysfunction.
Although our study showed no differences in the incidence of cardiac enzyme elevation including CK-MB and cardiac troponin-I between 2 groups, the IMR was a more accurate and sensitive for evaluating target vessel microvascular dysfunction. Several reasons can explain these discrepancies. First, IMR can increase without troponin elevation, and indicate a microvascular injury after PCI even in the absence of detectable myonecrosis.24) Second, since the time of cardiac enzyme measurement after PCI was different in each study, the peak value of cardiac enzyme could not reflect true myocardial damage always. Finally, our sample size was too small to be powerful enough to detect the difference. Accordingly, IMR might be a more sensitive method to detect microvascular dysfunction compared to cardiac enzyme after PCI.
Despite vulnerable plaques assessed using various imaging modalities being correlated to periprocedural MI, there was limited and debatable data for the prevention of periprocedural MI. Brilakis et al.25) have reported that embolic material was retrieved in 89% of the cases with lipid-rich plaques assessed with NIRS using filter devices; however, the Coronary Assessment by Near-infrared of Atherosclerotic Rupture-prone Yellow trial failed to demonstrate the efficacy of distal protection to prevent periprocedural MI in patients with lipid-rich plaques.26) The culprit LCBI4mm was higher in patients with periprocedural MI, however, the use of a distal protection device did not prevent periprocedural MI (35.7% vs. 23.5%, p=0.69).26) On the other hands, another study demonstrated that pre-PCI high dose statin therapy reduced post-PCI microvascular dysfunction as assessed using IMR.27) Moreover, early statin therapy within 48 hours after admission in statin-naïve patients with acute MI reduced long-term clinical outcomes compared with statin initiation later.28) The use of high dose statin before PCI and selected use of distal protection device are helpful to prevent periprocedural MI.
There were several limitations in this study. First, the major limitation is too small number of patients, patients of high LCBI group were only 7. This is a pilot observational retrospective study, and it is a limitation to draw meaningful statistical difference. To obtain statistical significance, statistically designed prospective study is necessary. Second, we did not measure CFR and IMR before PCI. However, in cases with significant epicardial stenosis at the target vessel, the IMR cannot reflect microvascular function accurately because of the effect of epicardial resistance. Third we did not conduct IVUS volumetric analysis. Volumetric analysis is helpful to understand the mechanism of plaque redistribution and embolization.
In conclusion, a large lipid-core plaque at the ‘culprit’ lesion is observed higher incidence of post-PCI microvascular dysfunction after PCI. Prospective study with adequate subject numbers will be needed.
 XML Download
XML Download