

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
To investigate the long-term follow-up results of arcuate keratotomy in femtosecond laser-assisted cataract surgery.
Methods
The medical records of 78 patients (99 eyes) with corneal astigmatism >0.5 diopters (D) who underwent arcuate keratotomy concurrent with femtosecond laser-assisted cataract surgery were retrospectively reviewed. Uncorrected and corrected visual acuities and keratometric and higher order aberration outcomes were compared preoperatively and 2 years postoperatively.
Results
The mean uncorrected visual acuities and corrected visual acuities changed from 0.55 ± 0.31 D and 0.33 ± 0.26 D, preoperatively to 0.13 ± 0.19 D and 0.07 ± 0.09 D, 2 years postoperatively. The mean preoperative corneal astigmatism was −1.15 ± 0.66 D. This was reduced to −0.79 ± 0.38 D at 1–2 days after surgery (p < 0.001), followed by no significant change for 2 years. The mean target-induced astigmatism was 1.15 ± 0.66 D preoperatively, and the mean surgically-induced astigmatism and difference vector were 0.69 ± 0.43 D and 0.83 ± 0.48 D, 2 years postoperatively. The mean correction index was 0.68 ± 0.45, 2 years postoperatively. There was no significant difference in higher order aberrations except 4 mm and 6 mm total higher order aberrations and 6 mm trefoil between preoperatively and 2 years postoperatively.
Figures and Tables
Figure 1
Preoperative and postoperative UCVA (logarithm of minimal angle of resolution, logMAR) and BCVA (logMAR) with standard deviation. Large improvement was shown at 1–2 days and maintained without significant change for 2 years. UCVA = uncorrected visual acuity; BCVA = best corrected visual acuity; Preop. = preoperative; mo = months; yr(s) = year(s).
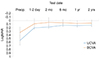
Figure 2
Preoperative and postoperative corneal astigmatism (diopter) with standard deviation. Significant improvement was shown at 1–2 days and maintained without significant change for 2 years. Wilcoxon signed rank test was used to examine statistical difference. Preop = preoperative; mo = month; yr = year; yrs = years; cyl = corneal astigmatism. *Significant difference between preoperation and postoperation 1-2 days.

Figure 3
Distribution of corneal astigmatism at preoperative and postoperative 2 years. Rate of patients below 1.0 diopter increased at 2 years after surgery. Preop. = preoperation; Postop. = postoperation; yrs = years; D = diopter.

Figure 4
Scatterplot of corneal astigmatism change. Scattered dots gathered within 1.0 diopter at 2 months after surgery. Preop. = preoperation; cyl = corneal astigmatism; mon = months; D = diopter.

Figure 5
Scatterplot of corneal astigmatism change. Similar distribution can be seen between 2 months and 2 years. mon = months; yr = years; cyl = corneal astigmatism; D = diopter.




Table 4
Vector analysis using Alphins method of keratometric astigmatic correction at 2 years after femtosecond-assisted combined phacoemulsification and arcuate keratotomy



References
1. Vickers LA, Gupta PK. Femtosecond laser-assited keratotomy. Curr Opin Ophthalmol. 2016; 27:277–284.
2. Park Y, Kim MS, Kim EC. Comparison of efficacies in treating astigmatism between toric intraocular lens implantation and limbal relaxing incision. J Korean Ophthalmol Soc. 2017; 58:1225–1233.

3. Steinert RF. Cataract surgery: Technique, complication and management. 2nd ed. Philadelphia: WB Saunders;2004. p. 253–266.
4. Mohammad-Rabei H, Mohammad-Rabei E, Espandar G, et al. Three methods for correction of astigmatism during phacoemulsification. J Ophthalmic Vis Res. 2016; 11:162–167.
5. Bahar I, Levinger E, Kaiserman I, et al. IntraLase-enabled astigmatic keratotomy for postkeratoplasty astigmatism. Am J Ophthalmol. 2008; 146:897–904.e1.
6. Hoffart L, Proust H, Matonti F, et al. Correction of postkeratoplasty astigmatism by femtosecond laser compared with mechanized astigmatic keratotomy. Am J Ophthalmol. 2009; 147:779–787.
7. Takács AI, Kovács I, Miháltz K, et al. Central corneal volume and endothelial cell count following femtosecond laser-assisted refractive cataract surgery compared to conventional phacoemulsification. J Refract Surg. 2012; 28:387–391.
8. Conrad-Hengerer I, Al Juburi M, Schultz T, et al. Corneal endothelial cell loss and corneal thickness in conventional compared with femtosecond laser-assisted cataract surgery: three-month follow-up. J Cataract Refract Surg. 2013; 39:1307–1313.
9. Abbey A, Ide T, Kymionis GD, Yoo SH. Femtosecond laser-assisted astigmatic keratotomy in naturally occurring high astigmatism. Br J Ophthalmol. 2009; 93:1566–1569.
10. Chan TC, Cheng GP, Wang Z, et al. Vector analysis of corneal astigmatism after combined femtosecond-assisted phacoemulsification and arcuate keratotomy. Am J Ophthlamol. 2015; 160:250–255.e2.
11. Day AC, Lau NM, Stevens JD. Nonpenetrating femtosecond laser intrastromal astigmatic keratotomy in eyes having cataract surgery. J Cataract Refract Surg. 2016; 42:102–109.
12. Baharozian CJ, Song C, Hatch KM, Talamo JH. A novel nomogram for the treatment of astigmatism with femtosecond-laser arcuate incisions at the time of cataract surgery. Clin Ophthalmol. 2017; 11:1841–1848.
13. Day AC, Stevens JD. Predictors of femtosecond laser intrastromal astigmatic keratotomy efficacy for astigmatism management in cataract surgery. J Cataract Refract Surg. 2016; 42:251–257.
14. Khan MI, Muhtaseb M. Prevalence of corneal astigmatism in patients having routine cataract surgery at a teaching hospital in the united Kingdom. J Cataract Refract Surg. 2011; 37:1751–1755.
15. Mayer WJ, Klaproth OK, Hengerer FH, et al. In vitro immunohistochemical and morphological observations of penetrating corneal incisions created by a femtosecond laser used for assisted intraocular lens surgery. J Cataract Refract Surg. 2014; 40:632–638.
16. Richard J, Hoffart L, Chavane F, et al. Corneal endothelial cell loss after cataract extraction by using ultrasound phacoemulsification versus a fluid-based system. Cornea. 2008; 27:17–21.
17. Tejedor J, Murube J. Choosing the location of corneal incision based on preexisting astigmatism in phacoemulsification. Am J Ophthalmol. 2005; 139:767–776.
18. Khokhar S, Lohiya P, Murugiesan V, Panda A. Corneal astigmatism correction with opposite clear corneal incisions or single clear corneal incision: comparative analysis. J Cataract Refract Surg. 2006; 32:1432–1437.
19. Barequet IS, Yu E, Vitale S, et al. Astigmatism outcomes of horizontal temporal versus nasal clear corneal incision cataract surgery. J Cataract Refract Surg. 2004; 30:418–423.
20. Amesbury EC, Miller KM. Correction of astigmatism at the time of cataract surgery. Curr Opin Ophthalmol. 2009; 20:19–24.
21. Hayashi K, Hayashi H, Nakao F, Hayashi F. Risk factors for corneal endothelial injury during pahcoemulsification. J Cataract Refract Surg. 1996; 22:1079–1084.
22. Juhasz T, Loesel FH, Kurtz RM, et al. Corneal refractive surgery with femtosecond laser. IEEE J Sel Top Quantum Electron. 1999; 5:902–910.
23. Roverts TV, Lawless M, Bali SJ, et al. Surgical outcomes and safety of femtosecond laser cataract surgery: a prospective study of 1,500 consecutive cases. Ophthalmology. 2013; 120:227–233.
24. Diakonis VF, Yesilirmak N, Cabot F, et al. Comparison of surgically induced astigmatism between femtosecond laser and maual clear corneal incisions for cataract surgery. J Cataract Refract Surg. 2015; 41:2075–2080.
25. Ahn DS, Han SY, Lee KH. Comparison of effective phacoemulsification time between femtosecond laser-assisted cataract surgery and conventional cataract surgery. J Korean Ophthalmol Soc. 2016; 57:236–242.
26. Chan TC, Ng AL, Cheng GP, et al. Corneal astigmatism and aberrations after combined femtosecond-assisted phacoemulsification and arcuated keratotomy: two-year results. Am J Ophthalmol. 2016; 170:83–90.
27. Eliwa TF, Abdellatif MK, Hamza II. Effect of limbal relaxing incisions on corneal aberrations. J Refract Surg. 2016; 32:156–162.
 XML Download
XML Download