

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The National Cancer Screening Program (NCSP) for gastric cancer and colorectal cancer (CRC) has been employed for Medical Aid recipients and National Health Insurance beneficiaries in the lower 50% income bracket in Korea.1234 In the NCSP, esophagogastroduodenoscopy (EGD) is conducted biennially for individuals aged ≥40 years,23 whereas annual fecal immunochemical test (FIT) and confirmatory colonoscopy are performed for those aged ≥50 years with positive FIT results.4
Since 2009, the quality indicators of EGD and colonoscopy have been measured through the National Endoscopy Quality Improvement Program (NEQIP) of the NCSP.567 The NEQIP includes indicators for the qualifications of endoscopists, quality improvement for instruments available at the endoscopy unit, endoscopic process, and measurement of outcomes for endoscopy screening.7 In Western countries, the quality indicators of EGD and colonoscopy have been recently revised on the basis of updated evidence.8910 The NEQIP was also revised; however, many quality indicators of the NEQIP were based mostly on expert opinion and variable levels of supporting evidence.11 Therefore, whether the revised NEQIP could represent relevant quality indicators and outcome measures of EGD and colonoscopy in the NCSP is questionable. Real-world evaluation of the revised NEQIP in clinical practice may be the first step towards successful widespread adoption of the NEQIP.
In this study, we evaluated the quality indicators of the revised NEQIP and outcome measures of EGD and colonoscopy performed at primary, secondary, and tertiary healthcare facilities participating in the NCSP.
Go to : 
MATERIALS AND METHODS
Study subjects
This study was conducted between March and August 2018 in primary, secondary, and tertiary healthcare facilities performing screening EGD and colonoscopy as part of the NCSP. Representative endoscopists, who were all directors of endoscopy units, were selected as potential respondents to complete a questionnaire for the revised NEQIP.11 In the NCSP, EGD is conducted biennially for individuals aged ≥40 years and confirmatory colonoscopy for those aged ≥50 years with a positive FIT result. FIT is performed as a quantitative test, and a cutoff value of 20 µg Hb/g feces (100 ng Hb/mL buffer) is used as the criterion for a positive FIT result. During the study period, there was no change in the quantitative FIT analyzer, examination methods, or cut-off values. All respondents voluntarily participated in this study and prospectively collected data on the outcome measures of EGD and colonoscopy monthly during the study period. This study was approved by the Institutional Review Board of Kyung Hee University Hospital at Gangdong (KHNMC 2017-02-025).
Quality indicators of the NEQIP
Before the online survey, the representative endoscopists were instructed to assess the quality indicators of the NEQIP using documents and over one off-line meeting. The respondents were surveyed for 34 quality indicators of the NEQIP,11 and those who did not complete the questionnaire were excluded from this study. The quality indicators of the NEQIP were classified into six domains: workforce, process, facility and equipment, outcomes, reprocessing, and sedation.11 The reported completion times of the survey ranged from 30 to 40 minutes. An e-mail survey was performed at 3 months after receiving instructions for the NEQIP. We sent a re-invitation e-mail to all potential respondents three times, conducted two phone calls, and sent three text messages to all non-respondents for the completion of the survey. In this study, the performance of the quality indicators was considered “optimal” when the performance level was ≥85% among the participants.
Outcome measures of endoscopy
In this study, all quality metrics focused on outcome measures, because outcome measures are the final target of quality improvement. The outcome measures of EGD included the number of EGDs performed per month, number of photo-documentations, total procedure time, proportion of sedative endoscopy, EGD with biopsy, precancerous/cancerous lesion (adenoma and carcinoma) detection, and EGDs with complications by month. The outcome measures of the FIT included the number of monthly FITs and proportion of positive FITs among all FITs by month. The outcome measures of colonoscopy conducted after obtaining a positive FIT result included total colonoscopy completion rate, number of monthly colonoscopies, waiting time to colonoscopy after notification of a positive FIT result, and the proportions of colonoscopies with biopsy, with advanced neoplasia (AN), which included advanced adenoma and carcinoma, and with adenoma alone. Colonoscopy completion rate was defined as the proportion of colonoscopies completed among those with a positive FIT. If the volume of colonoscopies conducted after obtaining a positive FIT result was not enough to measure the performance of colonoscopy, data on overall colonoscopies, including all diagnostic colonoscopies, were also collected. The outcome measures of the overall colonoscopies included the number of monthly overall colonoscopies, total procedure time, proportion of sedative colonoscopies, and colonoscopies with complications. In this study, complications associated with endoscopic procedures, as well as bowel preparation or sedation, were defined as any adverse events requiring endoscopic intervention or hospitalization. In this study, outcome measures of endoscopy were targeted for NEQIP of the NCSP; therefore, they were monitored at the facility level rather than the endoscopist level due to feasibility.
Statistical analysis
Descriptive statistics were used to summarize the quality indicators of the NEQIP and outcome measures of EGD and colonoscopy. Categorical data are expressed as numbers or percentages, whereas monthly continuous data are expressed as medians (ranges). One-way analysis of variance and Kruskal-Wallis test were used to compare differences in variables between three groups. All statistical tests were two-sided, and a p value of <0.05 was considered to indicate statistical significance. Statistical analyses were performed using the Statistical Package for the Social Sciences version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
We invited 17 representative endoscopists from 16 endoscopy units, and 15 of them responded for a participation rate of 88.2%. The complete overall response rate was 88.2% as there were no incomplete answers. Five (33.3%), seven (46.7%), and three (20.0%) of the respondents were working at primary clinics, secondary, and tertiary hospitals, respectively.
Quality indicators of the NEQIP
Table 1 shows the characteristics of the quality indicators of the NEQIP as assessed by the respondents participating in the NCSP. All respondents were gastroenterologists with fellow training of more than 1 year, had sufficient cumulative endoscopy volume, and continuous medical education (CME) for endoscopy. However, only 80% of them had optimal annual volume of EGDs (≥100 cases) and colonoscopies (≥50 cases). Further, only 53.3% of the endoscopy units had training for endoscopy quality improvement completed by ≥50% of their nursing staff. While most quality indicators were optimal, the quality indicators for colonoscopy reports, documentation of pathologic lesions (73.3% for both performance levels), the quality of reprocessing areas, and completion of endoscopy reprocessing education programs (53.3% for both performance levels) were suboptimal.
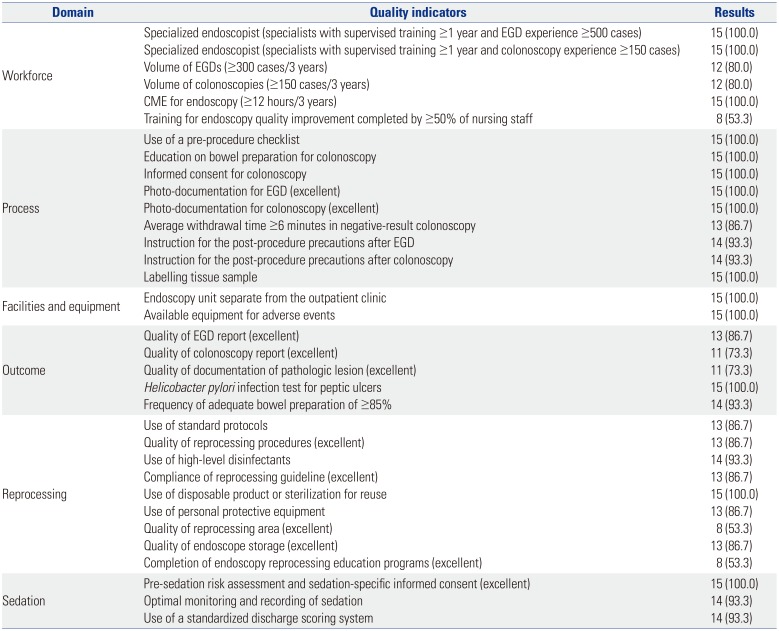
Table 1
Quality Indicators of the National Endoscopy Quality Improvement Program
![]()
Outcome measures of EGD
Table 2 shows the outcome measures of EGD performed in the facilities participating in the NCSP. The number of photo-documentations for EGD and total procedure time of EGD were higher at tertiary healthcare facilities than at other healthcare facilities (p<0.001 and p=0.023, respectively). The proportion of sedative EGDs, EGDs with biopsy, precancerous/cancerous lesion detection, and EGDs with complications were not different according to healthcare facility type [p=no significance (NS)].
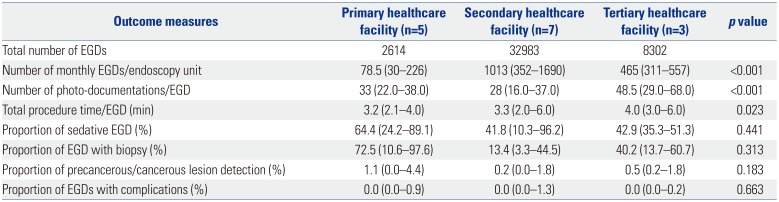
Table 2
Outcome Measures of EGD in the National Cancer Screening Program
![]()
Outcome measures of colonoscopy
Table 3 shows the outcome measures of colonoscopies performed in the facilities participating in the NCSP. The colonoscopy completion rate, number of monthly colonoscopies conducted after obtaining positive FIT results in the NCSP, and waiting time to colonoscopy were significantly higher at tertiary healthcare facilities (all p<0.001). The proportion of positive FITs, colonoscopies with biopsy, colonoscopies with AN, colonoscopies with adenoma, total procedure time of overall colonoscopies, and proportions of sedative colonoscopies and colonoscopies with complications were not different according to healthcare facility type (p=NS).
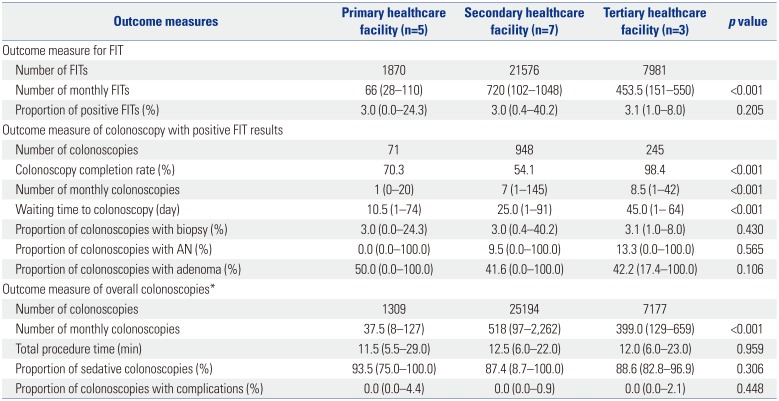
Table 3
Outcome Measures of Colonoscopy in the National Cancer Screening Program
![]()
Go to :
DISCUSSION
This is the first study to investigate quality indicators of the NEQIP and outcome measures of endoscopy in the NCSP according to healthcare facility type in Korea. Among the quality indicators of the NEQIP, most were close to optimal; however, the quality indicators for annual volume of EGD and colonoscopy, training for endoscopy quality improvement by endoscopy nursing staff, colonoscopy reports, documentation of pathologic lesions, quality of endoscopy reprocessing areas, and completion of endoscopy reprocessing education programs were not adequate.
In the NEQIP, the recommended annual volume of EGD and colonoscopy cases are 100 and 50, respectively.11 No consensus is reported on the minimum number of annual EGDs, whereas 150–200 annual colonoscopies are recommended in guidelines.1012 The European Society of Gastrointestinal Endoscopy (ESGE) recommends a minimum number of annual colonoscopies to be performed.10 The National Health Service Bowel Cancer Screening Programme of the United Kingdom and the Spanish Society of Gastrointestinal Endoscopy recommend at least 150 and 200 annual colonoscopies for their respective National CRC Screening Programs.10 Harewood13 reported an annual volume of at least 200 colonoscopies are required to maintain adequate competence among junior endoscopists. Considering suboptimal levels in the annual volumes of endoscopies in the present study, quality improvement programs may be advised to focus on low-volume endoscopists and endoscopy units. The US guidelines have suggested CME to maintain proficiency for endoscopists and endoscopy nursing staff,1415 however, education for the latter was not adequate in the NEQIP. Therefore, CME should be emphasized for the endoscopy nursing staff in the NCSP.
As the quality of endoscopy is closely associated with the quality of the endoscopy report, accurate endoscopy reporting is one of the main goals of the NEQIP.1116 The endoscopy report helps to exchange information on endoscopic findings, treatments, clinical recommendations, and adverse effects.1718 Suboptimal performance for colonoscopy reports and documentation of pathologic lesions in the NEQIP may be associated with a lack of awareness of the importance of accurate endoscopy reports and high endoscopy workloads in daily clinical practice. However, it is not easy to demonstrate a negative association between high endoscopy workloads and poor reports/documentations of colonoscopy because their objective measurement is difficult. In the reprocessing domain, the endoscopy examination area should be separated from the reprocessing area, because completely sterilized endoscopes may be re-contaminated during storage.1920 In the NEQIP, over 50% of endoscopists and reprocessing personnel are required to complete endoscopy reprocessing education programs.11 The suboptimal performance level for the quality of reprocessing areas and completion of endoscopy reprocessing education programs in the NEQIP may be associated with a lack of training in infection control and poor infrastructure for primary clinics.
For the outcome measures of EGD, the number of photo-documentations and total procedure times of EGD were significantly higher at tertiary healthcare facilities. The recommended minimum numbers of photo-documentations for EGD are 10 according to an ESGE quality improvement initiative17 and 8 according to the NEQIP, respectively.11 In this regard, the number of photo-documentations for EGD was excellent regardless of healthcare facility type in the current study. The total procedure time of EGD was also suggested as a potential quality indicator of EGD.17 It could be a outcome measure of EGD, which is comparable to the withdrawal time of colonoscopy; however, it is based only on limited evidence, and the cutoff procedure time varied from 3 to 7 minutes for EGD.212223 Biopsy rate could be considered as a quality indicator of EGD, as it has been shown to be associated with efficacy in gastric premalignant conditions, as well as with the rate of missed gastric cancers.24 However, it was not different among the different healthcare facility types. Precancerous/cancerous lesion detection rates in EGD could also be an important performance measure. However, no agreement has been reached on a specific cutoff for the detection of precancerous/cancerous lesions in the NEQIP because of inconsistency in supporting evidence.11 Furthermore, the proportions of EGDs with precancerous/cancerous lesions did not differ according to healthcare facility type. As the number of cases of precancerous/cancerous lesion was to small to analyze associations with total procedure time, biopsy, or photo-documentation, further larger studies are needed.
Regarding the outcome measures of colonoscopy, the colonoscopy completion rate and waiting time to colonoscopy were significantly higher at tertiary healthcare facilities. In US guidelines,25 the colonoscopy completion rate for those with a positive FIT should be more than 80%. In this regard, colonoscopy completion rate was only optimal at tertiary healthcare facilities in the current study. However, our results should cautiously be interpreted because colonoscopy could be performed at the cost of oneself (i.e., outside of NCSP) at primary and secondary healthcare facilities when participants had a positive FIT. Colonoscopy registry with a tracking system may be able to increase colonoscopy completion rates for those with a positive FIT. The waiting time to colonoscopy after obtaining a positive FIT result was 39.7 days in our previous study.26 A Spanish working group recommends an optimal waiting time to colonoscopy of less than 42 days.12 In a microsimulation model,27 12 months of waiting time to colonoscopy after obtaining a positive FIT result can yield proportional losses of screening benefits, according to a study in the US. In addition, longer waiting time for colonoscopy after obtaining a positive FIT result has been shown to be associated with an increased risk of neoplasia.28 However, waiting time for colonoscopy after a positive FIT is not an important issue in Korea, because median waiting times to colonoscopy are less than 45 days (1.5 months) regardless of healthcare facility type. The most important measure of FIT-based screening may be the AN detection rate; however, it was not suggested as a quality indicator in US guidelines owing to the low likelihood of those findings and the progressive reduction in those findings with subsequent series of FITs.25 The US guidelines suggested a 35–45% adenoma detection by colonoscopy as an outcome measure.25 In this regard, the outcome measure of the current study may be optimal, as the median proportions of colonoscopies with adenoma ranged from 41.6–50.0% regardless of healthcare facility type. The positive rate of FIT results was also suggested as a potential quality metrics for FIT,29 however, the proportion of positive FITs did not significantly differ according to healthcare facility type in this study.
Our study results need to be interpreted with caution in the context of potential limitations. The generalizability of the study results may be limited, owing to selection bias of the survey respondents, as they were all gastroenterologists and completed gastrointestinal fellowship training. In addition, our results may not be generalizable to other endoscopists who do not perform endoscopy in the NCSP. A larger survey from variable endoscopy settings may be warranted to overcome this limitation. Furthermore, the sample size was small. It was very difficult to enroll a large enough number of physicians who are willing to provide endoscopy quality data for the NCSP. Our respondents were representative endoscopists of each endoscopy units and presented actual clinical setting data in the NCSP. Previous studies based on the NCSP were limited by retrospective data collection, which is inaccurate, biased, and not representative of daily clinical practice. However, our data collection has minimal bias as the participating respondents fully agreed with the aim and the design of our study and collected data. Therefore, our findings reflect important NCSP data, despite the small sample size. The performance level of outcome measures was considered as “optimal” when the performance level was ≥85% among the participants in this study. However, there is no standard threshold of an optimal performance, which makes our definition arbitrary. Furthermore, outcome measures were monitored at the facility level rather than at the endoscopist level in this study. Considering the feasibility and reliability of quality metrics in the NCSP, since many endoscopists do not have adequate numbers of quality events to support reliable quality measurement, measurement at the facility level should be considered.30
In conclusion, outcome measures of endoscopy should be included as quality indicators of NCSP. However, universal outcome measures for all types of healthcare facilities should be established because performance levels of some outcome measures were different in each healthcare facility type.
Go to :
 XML Download
XML Download