

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Contrast induced nephropathy (CIN) is an acute kidney injury after iodinated contrast media administration. CIN frequently occurs in ambulatory or hospitalized patients and is associated with a prolonged hospital stay and adverse clinical outcomes.12 It is known that CIN is induced by renal medullary hypoxia and direct tubular epithelial cell toxicity mediated by reactive oxygen species. Contrast media also induces intrarenal vasoconstriction mediated by many factors including vasopressin, adenosine, endothelin, and calcium.3
The single most important risk factor of CIN is underlying renal function impairment.4 Other risk factors of CIN include diabetes mellitus (DM), old age, hypovolemia, decreased effective circulating volumes, hemodynamic instability, use of concurrent nephrotoxic agent, and large volume of contrasts consumed and high osmolality of the contrast agents.45
There are a few prophylactic strategies including volume expansion with either saline or sodium bicarbonated solutions, N-acetylcysteine (NAC), theophylline, fenoldopam, and statins.67 Oral NAC along with either saline or sodium bicarbonate is the most widely accepted preventive method.18 However, despite many clinical trials, the benefit of NAC is not consistent. The current guideline does not recommend NAC anymore.910 It means that CIN prophylaxis is not enough and optimal strategy has not been fully established.
Sarpogrelate is a selective 5-hyoroxytryptamine receptor subtype 2A (5-HT2A) antagonist that inhibits responses to 5-HT medicated by 5-HT2A receptors.11 The 5-HT2A receptor is associated with vascular smooth muscle contraction, platelet aggregation, thrombus formation and coronary artery spasm.12 Several studies demonstrated that sarpogrelate have some roles in the treatment of cardiovascular diseases.1112 A porcine model study demonstrated that sarpogrelate inhibited serotonin induced coronary arterial spasm in dose dependent fashion.13 In DM patients, sarpogrelate reduced plasma and urinary thromboxane A2, and these effects reduced albuminuria.14 However, the CIN protective effect of sarpogrelate has not yet been investigated thus far. We hypothesized sarpogrelate can prevent CIN by relieving intrarenal vasoconstriction.
Thus, this study examined whether sarpogrelate reduces the incidence of CIN or subsequent renal impairment during four weeks after coronary angiography compared with a control group.
METHODS
Study design
The study design was previously published.15 The study was designed as a non-blinded, prospective, randomized controlled clinical trial in a single center to evaluate the efficacy and safety of sarpogrelate with respect to CIN in chronic kidney disease (CKD) patients undergoing diagnostic coronary angiography (CAG) or percutaneous coronary intervention (PCI). Participants were randomly allocated into either the treatment group (routine treatment with sarpogrelate) or the control group (routine treatment without sarpogrelate). Randomization was carried out using sealed envelopes. In this study, routine treatment was defined as saline hydration and NAC administration. All patients received 0.9% saline or 0.45% saline intravenously at 1.0–1.5 mL/kg/hr for at least 6 hours before and 6–24 hours after the exposure to the contrast agent. Standard antiplatelet agents such as aspirin, clopidogrel, ticagrelor, or prasugrel were prescribed for the patients receiving PCI regardless of sarpogrelate intake. Lipid-lowering agents, anti-hypertensives, and antianginal medication were prescribed based on the discretion of each physician. High dose statins were defined as a prescription of 40 to 80 mg of atorvastatin or 20 mg of rosuvastatin. This study is registered with ClinicalTrials.gov, number NCT01165567.15
Study population
All patients with CKD scheduled for CAG were eligible. CKD was defined as kidney damage or estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73m2 for 3 months or more, irrespective of cause. The method of creatinine (Cr) measurement was isotope dilution mass spectrometry (IDMS) traceable method. The modification of diet in renal disease (MDRD) formula is defined as the followings with the Cr concentration in mg/dL16:
The exclusion criteria were age less than 20 years or more than 85 years, liver cirrhosis greater than or equal to Child class B, decreased serum platelet level (< 100,000/uL), patients who were scheduled to receive concurrently percutaneous renal intervention and patients taking anticoagulant. Patients in shock, maintaining hemodialysis, hemofiltration or peritoneal dialysis were all excluded. Patients who were assigned to the sarpogrelate group started oral sarpogrelate 24 hours before exposure to the contrast agent. The daily dose of sarpogrelate was 200–300 mg, which was divided into 2 or 3 times a day. Sarpogrelate intake was administered for 4 weeks. CAG was performed using the non-ionic, iso-osmolar contrast media iodixanol (Visipaque®, GE Healthcare AS, Oslo, Norway).
Outcome
The primary outcome of the study was the incidence of CIN, defined as either a greater than 25% increase of serum Cr or an absolute increase in serum Cr of 0.5 mg/dL within 48 hours after exposure to the contrast agent. Clinical data were collected in-hospital and at the four-week visit. Serum Cr concentration was measured at admission, at 12 and 48 hours after contrast exposure and at four weeks. Secondary outcomes were the incidence of renal impairment, the beginning of hemodialysis or hemofiltration and bleeding complications and renal recovery rate at the four-week follow-up. Four-week renal impairment is defined as the same criteria as CIN at four weeks. The renal function recovery is defined as any improvement of renal function at 1 month compared to post PCI renal function.
Statistical analysis
All numeric data are expressed as the mean ± standard deviation for continuous variables and percentage for categorical variables. The differences in clinical characteristics and laboratory values between the two groups were compared using Student's t-test for continuous variable and the χ2 test for categorical variables. The renal function changes were examined with paired t-test within each study group. To determine predictors of renal function worsening, simple linear regression analysis was performed for each well-known risk factor of CIN as well as for sarpogrelate. To exclude the confounding effect of the univariable analysis, multiple logistic regression analysis was done regardless of the statistical relevance in the univariable analysis. Baseline eGFR, age, DM, contrast amount used, ejection fraction, sarpogrelate were included in multivariable analysis. A P value of < 0.05 was used to indicate statistical significance. However, the P value is dependent on the sample size.1718 Statistics experts strongly recommend that all the quantitative analyses suggest ‘effect size’ which is independent of the sample size.19 We calculated the effect size of the CIN events, differences in serum Cr level, and eGFR between or within groups. The effect size was ln odds ratio (OR) for categorical variables, and for any difference between two continuous variables, it was calculated by Equations 1 and 2.20
Equation 1: difference (d) as an effect size between independent two groups.

Here, X1 and X2 are sample means; n1 and n2 are the sample size, and S1 and S2 are the standard deviation in each group.
Equation 2: difference (d) as an effect size between paired two groups.

Here, Y1 and Y2 are the sample means; Sdiff is the standard deviation of the difference between each paired data, and r is the correlation coefficient between Y1 and Y2 (e.g., the pretreatment-post-treatment correlation). This was done by online calculators at https://campbellcollaboration.org/research-resources/effect-size-calculator.html or https://effect-size-calculator.herokuapp.com/. All other statistical tests were performed with SPSS Version 23. (IBM SPSS Statistics, Chicago, IL, USA).
Ethics statement
The study was approved by the Institutional Review Board of Seoul Metropolitan Government-Seoul National University Boramae Medical Center (# 06-2009-123). The trial was undertaken in accordance with the Declaration of Helsinki. Written informed consent was given by all the subjects.
RESULTS
Originally, this study was designed to enroll 268 patients to get 80% statistical power. However, most of the eligible patients were reluctant to stay one extra day and declined to participate in this study. Finally, 74 eligible patients were randomized from April 2010 to March 2017. For one patient in the control group and two patients in the sarpogrelate group, the angiography was not performed because of the patients' refusal after enrollment. One patient in the sarpogrelate group expired during the CAG. One patient did not take sarpogrelate after assignment to the sarpogrelate group. One patient in the control group took sarpogrelate incorrectly after being assigned to the control group. One patient in the control group was excluded from the analysis because of a missed thrombocytopenia, and one patient was excluded due to follow-up loss (Fig. 1). Therefore, a total of 66 patients (89.2%) were included in the analysis. The baseline characteristics of the study subjects are listed in Table 1. The two groups were similar in baseline demographics, laboratory characteristics and procedure related factors including disease extent, presence of left main disease, multi-vessel disease or PCI and contrast amount used. The baseline ejection fraction of both groups was also similar.

Table 1
Demographic and clinical characteristics of study subjects

Data are presented as mean ± standard deviation or number (%).
Cr = creatinine, eGFR = estimated glomerular filtration rate, NT-ProBNP = N-terminal pro-brain natriuretic peptide, PCI = percutaneous coronary intervention.
![]()
Primary and secondary outcome
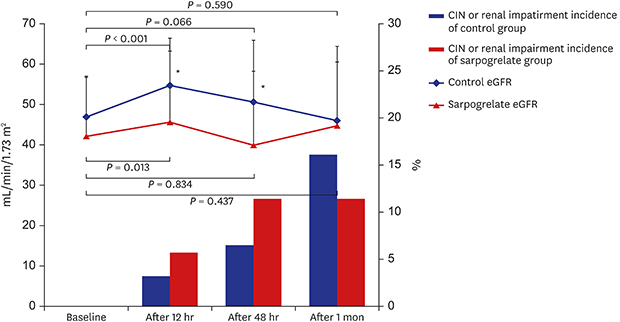
The cumulative incidence of CIN was 4.5%, 9.1% at 12, 48 hours and 13.6% for one month renal impairment, respectively, in the total population. CIN occurred numerically more at 48 hours in the sarpogrelate group and less at one month. However, the incidence showed no statistically significant difference between both groups at 12 and 48 hours and at one month (Table 2 and Fig. 2). The effect size, ln OR, was 0.63 at 48 hours and −0.40 at one month. There were no clinical or laboratory variables with statistical significance between the groups with or without CIN at 48 hours and at one month (data not shown). At four weeks, there were 5 patients in the control group and 4 patients in the sarpogrelate group who started hemodialysis. There was no significant difference in each group (P = 0.724). There was no bleeding complication in each group. Compared to control group, the sarpogrelate group showed significantly higher incidence of renal recovery rate at 1 month (53.6% vs. 24.0%; OR, 3.654; 95% confidence interval, 1.122–11.899; P = 0.028).
Table 2
The cumulative incidence of contrast induced nephropathy or renal impairment at each time interval and comparison between two groups

| Variables | Control | Sarpogrelate | P value | Effect size (ln OR) |
|---|---|---|---|---|
| After 12 hr | 1/31 (3.2) | 2/35 (5.7) | 1.000 | 0.60 |
| After 48 hr | 2/31 (6.5) | 4/35 (11.4) | 0.676 | 0.63 |
| After 1 mon | 5/31 (16.1) | 4/35 (11.4) | 0.724 | −0.40 |
![]()
 | Fig. 2Serial estimated GFR changes and cumulative incidence of CIN or renal impairment between two groups. Line graph shows serial eGFR and bar plot indicates the cumulative CIN incidence.eGFR = estimated glomerular filtration rate, CIN = contrast induced nephropathy.
*Between two groups, P value < 0.05.
|
Post hoc analysis
We compared renal function at each time interval between the two groups (Table 3 and Fig. 2). The baseline renal function was similar in both groups, but the eGFR was lower in the sarpogrelate group compared to the control group at 12 and 48 hours but not at one month. The effect size, d, was 0.49 and −0.60 at 12 hours and 0.38 and −0.63 at 48 hours, respectively, for the serum Cr and eGFR in the sarpogrelate group compared with the control group.
Table 3
Serial renal function changes

![]()
Serial renal function changes were demonstrated and compared with the baseline within each group (Table 4 and Fig. 2). In both groups, renal function improved significantly at 12 hours. eGFR improved from baseline to 12 hours by 3.6 ± 7.7 (effect size d was 0.21) in the sarpogrelate group and 7.6 ± 8.6 (effect size d was 0.68) in the control group, respectively (P value, paired t-test: 0.013 and < 0.001, respectively). However, this effect disappeared at 48 hours in both groups. This finding was attributable to renal function deterioration between 12 and 48 hours. eGFR decreased from 12 to 48 hours by 4.0 ± 6.4 in the sarpogrelate group (effect size d was −0.21) and 5.3 ± 7.9 in the control group (effect size d was −0.17), respectively (P value, paired t-test: 0.002 and 0.005, respectively) (Table 5). To summarize, in the sarpogrelate group, renal function was inferior during the first 48 hours and then comparable with the control group at one month. This was mainly contributed to the early larger improvement and late deterioration of the renal function in the control group.
Table 4
Serial renal function changes and comparison for matched pairs within each group

![]()
Table 5
Renal function comparisons between 12 hours and 48 hours for matched pairs within each group

![]()
In both the simple and multiple regression analysis models, the single most important predictor of eGFR at 48 hours was the baseline eGFR. Sarpogrelate was not an independent negative predictor of eGFR at 48 hours although the eGFR at 48 hours was lower in the sarpogrelate group (Table 6).
Table 6
The association of each risk factor with eGFR at 48 hours by simple and multiple linear regression analysis

![]()
DISCUSSION
This study was the first to investigate if sarpogrelate has a prophylactic effect on CIN. Although both groups showed improved renal function at 12 hours, it reversed to baseline at 48 hours. During the short period of treatment, there was no difference in the cumulative incidence of CIN between the control and sarpogrelate group. It means that sarpogrelate has no protective effect for CIN.
The main peripheral sources of 5-HT are platelets and pulmonary neuroepithelial cells. Several studies have demonstrated that 5-HT works on the cardiovascular system. In the porcine model, sarpogrelate, a selective 5-HT2A serotonin receptor antagonist, showed an inhibitory effect on coronary spasm and the possibility of an alteration of the serotonin receptors.13 Sarpogrelate was originally developed to inhibit platelet function, but it appeared to be beneficial for renal function as well. In DM patients, the effects of the 5-HT2 receptor antagonist sarpogrelate on microalbuminuria were examined. When comparing the sarpogrelate treated group and control group, the sarpogrelate treated group showed significantly reduced microalbuminuria and both decreased plasma and urinary thromboxane B2 (TXB2) levels. The blocking effect of 5-HT2 receptors appears to be effective in patients with nephropathy.14
Many studies have shown that sarpogrelate improved DM nephropathy by reduced urinary albumin excretion. Serotonin activates the Janus kinase/signal transducer and activators of transcription (JAK2/STAT-1) pathway mediated by the 5-HT2A receptor, resulting in the activation of monocyte chemoattractant protein-1 (MCP-1). MCP-1 has an important role in macrophage accumulation. Sarpogrelate not only increases the plasma adiponectin levels but also decreases the albumin to Cr ratio and the plasma and urinary MCP-1.21 In nephritis rate models, serotonin was shown to contribute to glomerular injury and crescent formation by macrophages induced by T cell activation.22
We did this study expecting the serotonin antagonist sarpogrelate to be effective by its vasodilation and anti-inflammatory actions. Disappointingly, sarpogrelate was not beneficial for CIN prophylaxis in the present study. It is presumed that serotonin does not have a key role although sarpogrelate has reno-protective effects. In our knowledge, the present study is the first study to evaluate the reno-protective effect of sarpogrelate.
This study has some limitations. First, the study population was too small to demonstrate a positive effect of sarpogrelate. We had to close the study prematurely because the enrollment rate was too slow. Because this study is underpowered, which means we might miss the true preventive effect of sarpogrelate for CIN, we need to pay attention to a few effect sizes suggested in this study. According to Dr. Cohen's rule of thumb, a d of 0.2, 0.5 or 0.8 and an OR of 1.5, 2 and 3 have a small, moderate and large effect size, respectively.1720 The OR of sarpogrelate was 0.67 for the incidence of renal impairment at one month which was converted from the ln OR of −0.40. This is compatible with the reciprocal of the small effect size with an OR of 1.49. Based on this statistical finding, it is anticipated a large sized study may reveal the renoprotective effect of sarpogrelate. Although eGFR was statistically significantly improved during the first 48 hours in both groups, even showing a larger improvement in the control group, the effect size was only small to moderate despite the extremely low P value. It is regarded as the effect from saline hydration. It is notable that this early preventive effect did not exist anymore at one month. Second, the cumulative incidence of renal impairment was numerically higher in the control group at one month. This suggests more CIN events might occur, and sarpogrelate was possibly effective after discharge. It might be inappropriate to measure the eGFR at 48 hours to detect the real benefit from sarpogrelate. Third, we could not explain why renal function was inferior to the control group during the first 48 hours. Even, we cannot deny sarpogrelate might have nephrotoxic effect during initial two days after taking. Forth, we did not know what medication patients were taking prior to and after CAG in detail and the difference between two groups. We cannot exclude the possibility the medicine can affect study results at last. Finally, although the sarpogrelate has possibility to have beneficial effect for CIN prevention through blocking vasoconstriction, there are very limited data supporting this hypothesis. Further studies should be followed including animal studies demonstrating its possible mechanism.
In conclusion, this study demonstrated that sarpogrelate has no renoprotective effect. The results obtained in our study indicate that different strategies that target any pathophysiology other than serotonin induced inflammation or vasospasm should be considered.
 XML Download
XML Download