

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Patient outcome after major surgical procedures were superior in hospitals with experienced surgical teams with higher case volume compared to hospitals with lower case volume.1 Similar correlation has also been shown for solid organ transplantation performed with significantly higher one year mortality rates after liver transplantation and higher one year graft loss after kidney transplantation (KT) in centers with low volume compared to those with high volume.2
Since the first kidney transplantation in 1954, the number of KTs have significantly increased with more than 80,000 KTs performed worldwide in 2015. According to data from the Korean Network for Organ Sharing, KTs in Korea have more than doubled during the past 10 years from less than 1,000 in 2007 to more than 2,200 in 2016.3 Although the surgical procedure itself is rather straightforward in comparison with other solid organ transplantations, preoperative preparation and postoperative management can often be challenging. Multi-professional expertise is required for optimal patient outcome in preparation and cross-matching before surgery, maintenance of immunosuppressants, prevention and treatment of infection, and monitoring graft function.
KT has both medical and surgical aspects of care. Compared to surgical procedures, the effect of case-volume in medical conditions have not been studied extensively with sporadic reports of lower intensive care unit (ICU) mortality rates in institutions with higher volume of ICU patients4 and higher cure rate of pneumonia associated with physicians who have more experience.5 However, the impact of institutional case volume on graft survival after predominantly living donor KT remains relatively unclear.
We hypothesized that similar to complex surgical procedures and medical conditions, graft survival after KT would be superior in institutions with higher case volume. A national retrospective cohort study was performed to assess the case volume effect on graft survival after KT in Korea.
METHODS
Data source and study population
The National Healthcare Insurance Service (NHIS) database of Korea includes all claims/reimbursement data for the population contained by the government regulated National Healthcare Insurance (NHI) program and the Medical Aid program. The NHIS database was provided for analysis after de-identification of personal information.6
We identified adult patients (age ≥ 18 years) who received KT between 2007 and 2016 from the NHIS database by searching the NHI procedure code for KT (R3280) during hospitalization. After identification of adult KT recipients, underlying comorbidities such as coronary artery disease, diabetes mellitus, hypertension, and cardiovascular disease were obtained from the database using International Classification of Diseases (ICD)-10 codes. For adjustment of the disease severity, the Elixhauser comorbidity index, which is originated from thirty disease entities using ICD-10 codes7 and shown to associate with hospital mortality,8 was used as a covariate. The Elixhauser comorbidity index is frequently utilized in health service research to adjust for confounders or to represent patient population characteristics. The Elixhauser comorbidity system may be slightly superior to Charlson comorbidity system when adjusting for comorbidities.9 Because a single KT procedure code was used for both living donor KT and deceased donor KT, anesthesia codes for elective procedures and urgent/emergent procedures were used to classify KTs into elective KT and urgent KT.
Definition of case volume
The definition of case volume was defined as the average number of KT performed per year at each institution. Although each center is assigned a code so that case volume can be determined, the code is de-identified, making it impossible to identify a specific center. Centers were classified in accordance with case volume as follows; low-volume centers (< 24 KTs/year), medium-volume centers (24–60 KTs/year), and high-volume centers (> 60 KTs/year). The rationale was that centers performing 2 KTs or less per month could be considered as low-volume centers, whereas centers performing more than 1 KT per week could be considered as high-volume centers.
Outcomes
One year graft survival was the primary outcome, defined as no dialysis requirement or re-transplantation, at one year after KT. Long term graft survival, in-hospital mortality, and hospital length of stay were also collected. Because death certificates are automatically reported to the NHI, mortality was detected when healthcare coverage by the NHI was terminated.
Statistical analysis
Patient characteristics were compared according to case volume using the one-way analysis of variance for continuous variables and χ2 test or Fisher's exact test for categorical variables. Graft survival after KT according to case volume was assessed using logistic regression model after adjusting age, gender, transplantation period, and Elixhauser comorbidity index. The goodness-of fit for the logistic regression model was assessed using Hosmer-Lemeshow test. Graft survival after KT according to case volume was compared using Cox proportional hazard model after adjusting for age, gender, and Elixhauser comorbidity index.
The graft survival analysis was performed using the log-rank test according to case volume. The goodness-of fit for the Cox proportional hazard model was assessed using the likelihood ratio test and the proportional hazard assumption was explored using the log-minus-log plot. Mean and standard deviations for KT outcomes (hospital length of stay and overall cost) according to case volume were presented and compared using the one-way analysis of variance.
All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA). Results were considered statistically significant when P values were less than 0.05.
RESULTS
From 2007 to 2016, a total of 13,872 cases of KT were performed in 74 centers in Korea. Characteristics of the patient and the center are described in Table 1. The number of KTs significantly increased over time.
Table 1
Patient and center characteristics
All values for continuous variables are means ± SD and for categorical variables are percentages.
KT = kidney transplantation.
![]()
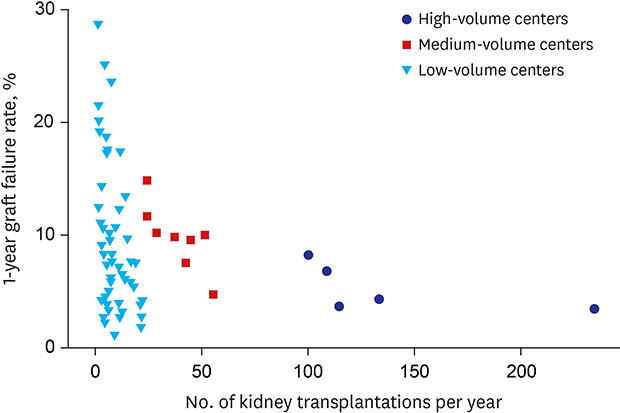
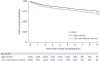
The overall one year graft failure rate was 7.0% (811/11,666). One year graft failure rate was significantly lower in the high-volume centers (5.1%) compared to medium-volume (9.7%; P < 0.001) or low-volume centers (8.2%; P < 0.001) (Table 2 and Fig. 1). Independent risk factors for one year graft failure were KT performed at medium-volume and low-volume centers (adjusted odds ratio [aOR], 1.87; 95% confidence interval [CI], 1.57–2.23; P < 0.001 and aOR, 1.50; 95% CI, 1.26–1.78; P < 0.001, respectively), urgent KT (aOR, 1.93; 95% CI, 1.66–2.25; P < 0.001), and Elixhauser comorbidity index (aOR, 1.01; 95% CI, 1.00–1.02; P = 0.015). However, 3- and 5-year graft failure rate was significantly higher only in medium-volume centers (aOR, 1.41; 95% CI, 1.21–1.65; P < 0.001 and aOR, 1.23; 95% CI, 1.03–1.47; P = 0.024, respectively) compared to high-volume centers. Long term graft survival analysis of up to 9 years showed superior results in high-volume centers compared to medium- and low-volume centers as shown in Fig. 2.
Table 2
One year graft failure after kidney transplantation

![]()
In-hospital mortality after KT was higher in old age, urgent KT, and higher Elixhauser comorbidity index (Table 3). After adjustment, low-volume centers had significantly higher mortality compared to high-volume centers (aOR, 1.75; 95% CI, 1.15–2.66; P = 0.010). Medium-volume centers did not show significant difference. The overall mortality rate after KT was 4.7% (655/13,872) and adjusted risk factors were urgent KT (aOR, 2.01; 95% CI, 1.72–2.36; P < 0.001), KT at medium-volume and low-volume centers (aOR, 1.27; 95% CI, 1.04–1.55; P = 0.02 and aOR, 1.38; 95% CI, 1.16–1.65; P < 0.001, respectively), and older age (19–49 vs. 50-59. vs. 60 and above, 2.7% vs. 5.8% vs. 10.5%, aOR, 2.35; 95% CI, 1.95–2.83; P < 0.001 and aOR, 4.62; 95% CI, 3.78–5.65; P < 0.001, respectively).
Table 3
In-hospital mortality after kidney transplantation

![]()
The overall hospital length of stay was 28.1 ± 17.7 days. High-volume centers showed a significantly shorter hospital length of stay (27.3 ± 18.5 days) compared to medium- (29.3 ± 16.8 days) or low- (28.7 ± 17.0 days) volume centers (P < 0.001).
DISCUSSION
Our study showed that higher center volume was associated with lower graft failure rate after KT. High-volume centers (> 60 KTs per year), had lower one year graft failure rate after KT compared to low-volume centers (< 24 KTs per year). High-volume centers also showed lower mortality than low-volume centers.
There are a few reports in the literature that evaluated the case volume effect in KTs. The most recent retrospective study evaluated outcomes for adult deceased donor KT over a 15-year study period.10 Of the 206,179 deceased donor KTs analyzed, high-volume centers showed a significantly lower observed-to-expected rates of one year graft loss and one year mortality compared to low-volume centers, which is consistent with our study. In another study of 1,060 KTs performed in Taiwan, high volume centers that have performed more than 72 KTs showed lower mortality and higher 1 to 3 year graft and patient survival rates compared to low volume centers.11 Discrepancies when compared to our study include the use of 72 cumulative cases over 8 years as cutoff between high and low volume centers as opposed to annual case volume of KT and the smaller number of KTs included (1,060 vs. 13,872). In another study regarding case volume effect in pediatric KTs using data from North American Pediatric Transplant Cooperative Study database, high volume centers (>100 KTs) showed lower incidence of graft thrombosis and acute tubular necrosis, and therefore, lower graft failure rates.12 Our study is the largest adult KT study to evaluate the case volume effect in more than 13,000 patients over 10 years and demonstrated improved short-term and long-term graft survival rate in high-volume centers compared to low- or medium-volume centers.
Graft failure after KT impacts the patient's quality of life and long-term survival,13 but studies concerning risk factors of graft failure after KT is limited to specific subpopulations. A prospective study in deceased donor KT population identified KT from circulatory death donors, expanded criteria donors, and elderly donors, and vascular thrombosis as independent risk factors graft loss within 30 days of KT requiring graft nephrectomy or dialysis.14 Although our study did show a higher graft failure rate after urgent KT compared to elective KT, the significance of our study lies in the impact of case volume on both short term and long term graft failure rate and in-hospital mortality. Another study evaluated elderly KT recipients (> 60 years) and showed ABO incompatibility, delayed graft function, cytomegalovirus infection, and hepatitis B virus infection as independent risk factors of graft failure.15
Of note, our study showed a tendency towards increased risk of one year graft failure in women compared to men (6.6% vs. 7.4%, adjusted P = 0.066). Previous reports are conflicting with some showing better graft survival in women16 and others showing better graft survival in men.17 Our results seem to be in accord with the more recent report.17
Other studies regarding the association of physician case volume and in-hospital mortality include children diagnosed with pneumonia. Physicians with more experience in treating children with pneumonia were able to provide better respiratory care, reducing hospital length of stay, in-hospital mortality, and medical costs.18 Patient mortality and risk of graft failure may be dependent on surgical and medical experience of the hospital due to complexity of the surgery and postoperative care. A multicenter retrospective study on noninvasive ventilation use during acute exacerbations of chronic obstructive pulmonary disease suggested that accumulated experience is associated with higher probability of using noninvasive ventilation, which is associated with decreased mortality.19 KT also requires comprehensive post-transplant care and patient follow-up, which may be provided more optimally in high-volume centers where care is more likely to be protocolled and specialized. Most reported cause of patient mortality after KT include infection, cardiovascular complications, hepatic failure, and malignancy.2021 In a study of 19,103 KTs performed between 2001 and 2012, reported risk factors of one year mortality were old age, deceased-donor KT, and pre-transplant comorbidities.22 Similarly, risk factors for in-hospital mortality in our study included old age and urgent KT. Deceased donor KT is a well-known risk factor of poor outcome after KT compared to living donor KT.23 Living and deceased donor KT could not be differentiated because the procedure code for living donor KT and deceased donor KT was identical. We attempted to distinguish between living and deceased donor KT by using the elective and urgent/emergent anesthesia codes based on the assumption that deceased donor KTs would carry urgent/emergent anesthesia codes. However, sample hospital based data obtained to verify the assumption showed significant discrepancy between the proportion of deceased donor KTs and KTs with the urgent/emergent anesthesia codes, implying that many deceased donor KTs were performed during routine hours. However, the center case volume effect on graft failure rate and patient mortality was significant even after adjusting for the urgency of KT in our study.
Because solid organs for transplantation are an extremely valuable resource, developing standards or regulations for identifying qualified transplant centers is reasonable. In the United States, all transplant centers are required to meet quantitative and qualitative standards in order to maintain the status as a transplant center of each solid organ.24 Korea lacks such regulations and solid organ transplantations may be performed with no requirements or performance standards to meet. The one year graft failure rate of up to 30% and high in-hospital mortality in a number of low volume centers may serve as a starting point for discussions regarding quality control for transplanting scarce solid organs.
There are some limitations to consider in our study. First, the study used administrative data with limited clinical information. However, the completeness of the data, which includes all KT data performed in Korea for 10 years and no selection bias, and the concrete outcomes evaluated, is likely to suffice in supporting the conclusion. Second, due to lack of previous studies to use as reference, the number of KTs for defining low-, medium-, high-volume center was arbitrary. Centers were classified as high-volume centers when more than one KT was performed per week and as low-volume centers when less than one KT was performed per month.
In conclusion, high-volume centers, performing more than 60 KTs per year, were associated with lower postoperative graft failure rate and lower mortality.
 XML Download
XML Download