

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Tuberculosis is a major health problem, with 10.0 million cases and 1.3 million deaths worldwide in 2017.1 There are two types of tuberculosis infection status, active tuberculosis and latent tuberculosis.2 Latent tuberculosis infection is the presence of an immune response to Mycobacterium tuberculosis antigens without clinical manifestations of active tuberculosis.3 About 10%–15% of individuals with latent tuberculosis infection develop active tuberculosis. The majority of cases of active tuberculosis develop within five years of infection.4 Almost one quarter of the world population have latent tuberculosis infection.5 Individuals with latent tuberculosis infection are the major reservoir of M. tuberculosis.6 Indonesia is a high-tuberculosis-burden country, and had the third highest number of people with latent tuberculosis infections (120 million) after China and India in 2016.5
Various bacterial, host, and environmental factors, contribute to reactivation of latent tuberculosis infection.6 Tuberculosis-human immunodeficiency virus (HIV) co-infection is a major risk factor for the reactivation of latent tuberculosis infection.7 In HIV-infected individuals, the lower the CD4+ T lymphocytes (CD4+ count), the higher the risk of tuberculosis, other opportunistic infections, and tuberculosis-related mortality.89 In addition, the management of both HIV and tuberculosis are significantly more complex in individuals with tuberculosis-HIV coinfection, compared to individuals with either infection alone.8 The management of tuberculosis-HIV coinfection is a major challenge, especially in countries with a high burden of tuberculosis.10
It is estimated that HIV prevalence in Indonesia among the population over the age of 15 years was 0.33% in 2015 and it is expected decrease slightly to 0.32% in 2020.11 Due to the high prevalence of tuberculosis infection in Indonesia, individuals with HIV infection have a high risk of developing active tuberculosis due to reactivation of latent tuberculosis infection.
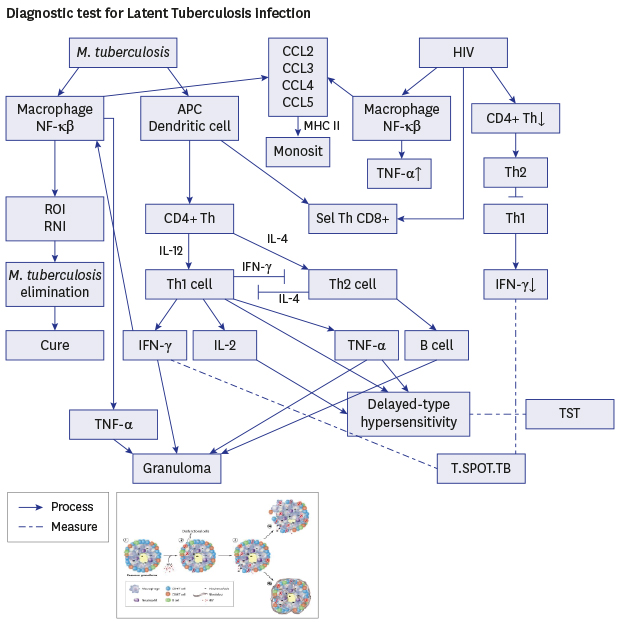
Currently, there is no gold standard test for the diagnosis of latent tuberculosis infection. Individuals with latent tuberculosis infection have a low level of M. tuberculosis bacteria and, therefore, diagnosis of latent tuberculosis infection relies on testing of the individual immune response to M. tuberculosis antigen.712 There are two methods for detection of latent tuberculosis infection recommended by World Health Organization, the tuberculin skin test (TST) and interferon-gamma release assays (IGRAs).7 Both methods have low sensitivity, especially in individuals with severe immunodeficiency.1314 The TST is based on the delayed-type hypersensitivity reaction that occurs when those infected with M. tuberculosis are exposed to certain antigenic components, and the IGRA is based on the immune response to specific M. tuberculosis antigens which are not present in BCG or certain nontuberculous mycobacteria.15
Studies to compare IGRA and TST for the detection of latent tuberculosis infection in countries with varying burdens of tuberculosis have been conducted previously,141617181920 but it is still unclear which test performs better in high tuberculosis-prevalence settings. There is also a very limited number of studies that have evaluated the performance of these tests in HIV-infected individuals in countries where most people receive BCG vaccination.
The aim of this study was to evaluate the level of agreement between the T-SPOT.TB test and TST in the diagnosis of latent tuberculosis infection in HIV-infected patients in Indonesia, a country with a high burden of tuberculosis.
METHODS
Study population and study design
This study was a cross-sectional study which was conducted in Moewardi Hospital, a teaching hospital in Surakarta, Indonesia from November 2016 to January 2017. The participants were outpatients attending clinic that provided HIV testing. Participants were selected by a consecutive sampling based on clinical symptoms, HIV rapid test results, and age ≥ 18 years. Baseline characteristics were determined by interviewing the participants taking a history of their HIV treatment. Their age, gender, HIV stage, time on antiretroviral therapy (ART), BCG vaccination, BCG scar, previous tuberculosis infection, history of taking antituberculous drugs, and a history of close contact with someone with active tuberculosis were documented. A close contact history was defined as a history of living with a person with tuberculosis, or having frequent contact with people with active tuberculosis. To rule out the presence of active tuberculosis infection, participants had a chest X-ray and were clinically examined by a pulmonologist. BCG vaccination status was determined by asking about the history of BCG vaccination and checking for a BCG scar. Participants were required to be HIV-positive, ≥ 18 years old, and to provide voluntary, informed consent. HIV patients with clinical symptoms of active tuberculosis infection, an abnormal chest X-ray, a history of active tuberculosis, or who were taking antituberculous drugs, were excluded.
Determination of HIV stage
The HIV stage was determined by measuring the level of CD4+ cells using a flow cytometer (BD FACSCount, Becton Dickenson, San Jose, CA, USA) according to the manufacturer's instructions.
Determination of Latent Tuberculosis Infection using Tuberculin Skin Test (TST) and Interferon-gamma release assay (T-SPOT.TB)
The IGRA (T-SPOT.TB) and TST were done concurrently. Each participant provided a blood sample for the T-SPOT.TB test; following this, TST was performed by intradermal injection of Tuberculin PPD RT23, 2 TU (Statens Serum Institute, Copenhagen, Denmark). The reading of skin induration was done in an outpatient clinic, 48 to 72 hours after PPD injection. A positive result was defined as the presence of skin induration at the injection site, with diameter more than 5 mm. T-SPOT.TB test was conducted with the tuberculosis-specific antigens early secretory antigenic target 6-kDa protein (ESAT-6) and culture filtrate protein 10 (CFP 10) with an enzyme-linked immunosorbent spot assay. The interpretation of T-SPOT.TB result was done according to the manufacturer’s instructions.
Participants’ tuberculosis status (i.e., exclusion of active tuberculosis) was determined by sputum smear examination and sputum testing using GeneXpert MTB/RIF (Cepheid, Sunnyvale, CA, USA). Sputum was collected for microscopic examination using Ziehl-Neelsen staining. GeneXpert MTB/RIF was done according to the manufacturer's instructions.
Data analysis
Frequency and descriptive statistics analyses were used to describe baseline characteristics. The level of agreement between TST and T-SPOT.TB was determined using Cohen's κ coefficient, which was interpreted as follows: < 0.2, poor agreement; 0.2–0.39, fair agreement; 0.4–0.59, moderate agreement; 0.6–0.79, good agreement, and 0.8–1.0, very good agreement. We used SPSS Version 21 (IBM Co., Armonk, NY, USA) for all the analyses. A P value < 0.05 was considered statistically significant.
RESULTS
Characteristics of the study participants
Participant characteristics are shown in Table 1. A total of 115 participants were enrolled in the study. However, three participants were later excluded, leaving 112 participants in the study. The reasons for exclusion were active tuberculosis infection (n = 1), and blood sample lysis (n = 2). All except two of the 112 participants were on antiretroviral therapy. Participants' HIV stage according to the CD4+ count is shown in Table 2.
Table 1
Baseline characteristics of human immunodeficiency virus positive individuals involved in this study (n = 112)

Agreement between the TST and T-SPOT.TB test results
Of the 112 participants, 20 showed positive results by T-SPOT.TB test and 21 positive results by TST (Table 3). The two tests had good agreement (κ = 0.648; P < 0.001). Overall, 101 out of 112 (90%) had concordant TST and T-SPOT.TB test results, with 15 (13%) having concordant positive results, and 86 (77%) having concordant negative results. However, among the 36 participants with CD4+ counts < 200 cells/mm3, 4 (12.5%) had a positive T-SPOT.TB test and a negative TST, while none had a positive TST and a negative T-SPOT.TB test.
Table 3
The agreement between TST and T-SPOT.TB for the detection of latent tuberculosis infection in human immunodeficiency virus infected individuals (n = 112)

| Variables | T-SPOT.TB test | Participants (n = 112) | ||
|---|---|---|---|---|
| Positive results | Negative results | |||
| TST | ||||
| Positive result | 15 | 6 | 21 | |
| Negative result | 5 | 86 | 91 | |
| Total | 20 | 92 | 112 | |
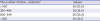
Performance TST and T-SPOT.TB according to the CD4+ count
The performance of the TST and T-SPOT.TB tests was evaluated according to the level of CD4+ (Table 4), and the proportion of participants with positive results according to CD4+ count is shown in Fig. 1. There was a statistically significant difference in the sensitivity of the TST and T.SPOT-TB tests in the detection of latent tuberculosis in participants with CD4+ < 200 cells/mm3 (P < 0.001).
Table 4
Performance of TST and T.SPOT.TB based on the number of CD4+ (cells/mm3)
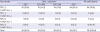
Fig. 1
Percentage of latent tuberculosis positive based on CD4+ level measured by TST and T.SPOT-TB. Among participants with a CD4+ level < 200 cells/mm3 the number with a positive T.SPOT-TB was greater than the number with a positive TST (P < 0.001).
TST = tuberculin skin test, CD4 = cluster of differentiation 4.
DISCUSSION
Our study evaluated the performance of TST and T-SPOT.TB for diagnosis of latent tuberculosis infection in HIV patients living in a high tuberculosis prevalence setting with universal BCG vaccination. None of the participants reported having had close contact with someone with active tuberculosis, but it can be assumed that the majority had been exposed to tuberculosis because of the high prevalence of tuberculosis in the region.
In this study, TST and T-SPOT.TB detected latent tuberculosis infection in 19% and 18% of the participants, respectively. A study of latent tuberculosis among drug-users with HIV infection in Indonesia revealed a prevalence of 29% using QuantiFERON Gold In-Tube assay, another type of IGRA.21 This prevalence is higher than that found in our study using T-SPOT.TB. The higher prevalence could be attributable to the different type of IGRA that was used, the higher proportion of participants who had household exposure to tuberculosis (10%–30%), and the high proportion of participants who had previously been treated for tuberculosis (approximately 40%).21
It has been reported that the positive predictive value of TST for detecting latent tuberculosis infection may be reduced due to BCG vaccination and a high prevalence of non-tuberculous mycobacterial infections.22 The high level of agreement between the TST and T-SPOT.TB results in this study indicates that BCG vaccination did not affect the TST results. Most of the people in countries with a high burden of tuberculosis receive BCG vaccination in early infancy and this is unlikely to affect TST results later in life.4
Almost one third of participants in this study had a CD4+ level < 200 cells/mm3. There were a high number of participants with negative results on both study tests, and the likelihood of negative results increased as the CD4+ level decreased. This suggests that TST and T-SPOT.TB test results are influenced by CD4+ levels. The low sensitivity of both TST and T-SPOT.TB to detect latent tuberculosis infection in HIV-infected individuals may due to the immunosuppression associated with a low CD4+ level.14172324 A low CD4+ level impairs the function of T-helper cells and consequently reduces the secretion of interferon gamma by the T helper cells.25 The reduction of interferon gamma leads to macrophage activation, which in turn leads to monocyte infiltration of the tissue via CCL2 chemokines, which suppresses induration in response to the TST.26 The reduction of interferon gamma leads to a reduction of the number of spots read by T-SPOT.TB, increasing the likelihood of a negative result.26 However, among participants with a CD4+ level < 200 cells/mm3, the number with positive T-SPOT.TB was greater than the number with positive TST results. This suggests that T-SPOT.TB is better than the TST at detecting latent tuberculosis infection in individuals with a low CD4+ level. This result is similar to the findings of a previous study, which showed that IGRA is less affected by CD4+ level than the TST.27 It has been reported that immunosuppression in HIV-infected individuals may lead to false-negative TST results.27 Therefore in individuals with a low CD4+ level, negative results of TST and T-SPOT.TB does not rule-out latent tuberculosis infection. In addition, the World Health Organization recently recommended that prophylactic tuberculosis treatment should be offered for all HIV-positive patients without active tuberculosis and a positive or unknown TST result, regardless of the CD4+ count.3
In this study, the TST and T-SPOT.TB results had good agreement. A previous prospective study comparing IGRA and TST for the detection of latent tuberculosis infection, conducted in India, had similar results to this study.22 However, most of the other previous studies have shown poor to fair agreement between these two test methods.1719232428 This may be because most of these studies were conducted in settings with a low prevalence of tuberculosis. It has been reported that IGRA may be more accurate than TST for the detection of latent tuberculosis infection in patients older than 60 years with radiographic lesions.16 In addition, in countries with a high burden of tuberculosis, people are continuously exposed to environmental Mycobacteria, which may have a greater impact on the response to M. tuberculosis compared to those living in settings with a low tuberculosis prevalence. This is supported by studies that have shown geographical variations in response to M. tuberculosis antigen.29 In addition there is also a possibility of patients being exposed to non-tuberculous mycobacteria from contact with other patients.
Due to the lack of gold standard to detect latent tuberculosis infection in HIV-infected individuals, the choice of test to screen for latent tuberculosis infection depends on the available resources and logistic considerations.3031 The World Health Organization recommends that all HIV-infected individuals, with an unknown or positive TST result, and who are unlikely to have active tuberculosis, should be given prophylactic treatment for tuberculosis as part of a comprehensive package of HIV care.3 The US Centers for Disease Control and Prevention and the Canadian Tuberculosis Committee recommend dual testing using TST and an IGRA.12 Health authorities in several European countries and South Korea, also recommend dual testing, but health authorities in some countries with a low prevalence of tuberculosis, such as Germany and Japan only recommend IGRA as an initial test.30 Health authorities in some other countries recommend testing using an IGRA when the TST result is negative.30 Indonesia is a country with a high burden of tuberculosis and a low prevalence of HIV infection (0.3%).1 To prevent the progression of active tuberculosis in HIV patients, Indonesian government recommends giving isoniazid preventive treatment (IPT) to all HIV positive patients without TST or IGRA tests, unless they have clinical signs and symptoms of active tuberculosis.332 This recommendation causes unnecessary treatment to the HIV positive patients. This study indicates that TST is useful to diagnose latent tuberculosis to reduce unnecessary treatment in HIV positive patients.
A limitation of this study is the small number of participants. However, it is the first study to compare TST and IGRA for the diagnosis of latent tuberculosis in HIV-positive individuals in Indonesia and provides useful results.
In conclusion, there was good agreement between the TST and T-SPOT.TB results in diagnosing latent tuberculosis infection in HIV-infected individuals. Based on our study findings, we recommend that the TST remain the preferred test for the diagnosis of latent tuberculosis infection in HIV-infected individuals, especially in resource-limited settings because this method is simple and cost-effective. However, in individuals with immunodeficiency, T.SPOT.TB might be useful to rule out latent tuberculosis infection if a false-negative TST result is suspected.
 XML Download
XML Download