

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pulmonary hypertension (PH) is common and is associated with high mortality and morbidity.1)2) Among various etiologies for PH, left ventricular (LV) dysfunction is the most common one and accounts for 65%–80% of all PH.3)4)5)6)7)8) A combination of elevated LV filling pressures and reactive pulmonary vascular remodeling results in PH secondary to left heart disease.3)6) Many patients with heart failure with reduced ejection fraction (HFrEF) have PH, and the presence of PH is associated with increased mortality and morbidity regardless of LV ejection fraction (LVEF) and stage of heart failure (HF).8)9)10)11)12)13) LVEF and degree of PH are not static and can change with treatment. A substantial number of patients with HFrEF recover LVEF in response to guideline directed medical therapy.14) Moreover, the presence and severity of PH can vary with treatment and it depend on the compensation status.15) Data on long-term prognosis of patients who experience improvement of LVEF and/or PH are scarce. Hence, we evaluated the long-term clinical outcome of patients with HFrEF and PH according to the improvement of PH and/or LVEF.
METHODS
Study population
We screened all consecutive patients with HFrEF and PH in Chungnam National University Hospital from September 2011 to March 2017. We collected baseline clinical profiles from their medical records and echocardiographic data from digitally stored echocardiographic images. HFrEF was defined when patients had symptoms and signs of HF and LVEF < 40%. Of them, we included only patients who underwent follow-up echocardiographic study within 12 months from the baseline echocardiography. Patients with other concomitant diseases including malignancy which can affect survival were excluded. We classified our study population into 4 groups according to the improvement of PH and/or LVEF based on the follow-up echocardiographic findings. Group 1 included patients with both improvements, group 2 with an improvement of PH only, group 3 with an improvement of LVEF only, and group 4 persistence of PH and no LVEF improvement. The primary endpoint was the development of major adverse cardio-cerebrovascular event (MACCE) including all-cause death, myocardial infarction, stroke or transient ischemic attack (TIA) and admission for HF for 5 years. HF hospitalizations were defined as unplanned hospitalizations of at least 24 hours due to worsening HF and were identified from their medical records. The study complied with the Declaration of Helsinki principles. The study protocol was approved by the institutional review board (IRB). The IRB waived the need for written informed consent from the study patients.
Echocardiographic measurement
We reanalyzed all echocardiographic images from baseline and follow-up echocardiographic studies. LVEF was calculated with the biplane modified Simpson's method with apical 4 chamber and apical 2 chamber views. The presence and degree of tricuspid regurgitation (TR) was found in the focused right ventricular view with color flow mapping. TR velocity was measured with the application of continuous wave Doppler to TR signal. Pulmonary artery systolic pressure (PASP) was estimated with the maximal velocity of TR (TR Vmax) and size of the inferior vena cava with respiratory change. In the follow-up echocardiographic examination, we checked the improvement of LVEF and change of PH based on baseline LVEF and TR Vmax levels. PH was defined TR Vmax ≥ 3.0 m/s by Doppler-derived velocity of optimal TR jet. The improvement of PH was defined when TR Vmax decreased to < 3.0 m/s in the follow-up echocardiography. Improvement of LVEF was defined as LVEF ≥ 15% from baseline to follow-up echocardiography.
Statistical analysis
Data are presented as numbers and frequencies for categorical variables and as mean ± standard deviations for continuous variables. For comparisons among the groups, the χ2 test (or Fisher exact test when any expected count was < 5 for a 2 × 2 table) was performed for categorical variables, and the one-way analysis of variance was used for continuous variables. We plotted survival curves according to our study groups using the Kaplan-Meier method with comparison using the log rank test. The time to first clinical event was analyzed using the multivariate Cox-proportional hazard analysis to determine the independent predictors of MACCE. In the multivariable analysis, we included all variables as covariates found to be statistically significant (p < 0.05) in the univariate analysis or variables known to be clinically important, excluding those with multicollinearity with others.
A two-sided p-value of < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 22.0 (IBM Co., Chicago, IL, USA)
RESULTS
We screened 1237 consecutive patients with HFrEF and PH from September 2011 to March 2017. Of them, 963 patients had no follow-up echocardiographic examination and 3 patients had malignancies affecting survival, so that total of 271 patients were included in this final analysis.
The mean age was 65 ± 14 years, 167 (62%) were males, 219 (81%) had de novo onset of HF. Baseline, echocardiographic characteristics and clinical outcomes were summarized in the Table 1. Hypertension and dyslipidemia were common in our study population (48% and 47%, respectively). At baseline, the mean LVEF was 28.1 ± 8.3% and that of TR Vmax was 3.4 ± 0.4 m/s. Regarding the medical therapy, 91% received beta-blockers and 86% received renin-angiotensin system inhibitors. Follow-up echocardiographic examinations were performed at an average of 5.5 ± 3.6 months from the baseline echocardiography. One-hundred and eighty-three patients (68%) showed improvement of LVEF, and 165 (61%) demonstrated improvement of PH. The improvement of LVEF (74.4% vs. 38.5%, p < 0.001) and improvement of PH (67.1% vs. 34.6%, p < 0.001) were more frequent in patients with de novo HF group. According to the improvement of PH and LVEF based on the follow up echocardiogram, we classified the study population into 4 groups as follows: 134 patients (49%), 31 patients (11%), 49 patients (18%) and 57 patients (21%) were classified as group 1, 2, 3, and 4, respectively (Figure 1). Overall, patients in group 4 were older, less likely to have de novo onset of HF. The use of guideline-directed medical therapy did not differ between the groups. In follow-up echocardiography, the mean LVEF were 45.3 ± 11.1% in patients with improved LVEF (group 1 and 3) and 29.8 ± 8.5% in patients without LVEF improvement (group 2 and 4). The TR Vmax was significantly lower in patients with improved PH (group 1 and 2) than patients with sustained PH (group 3 and 4) (2.4 ± 0.3 m/s vs. 3.4 ± 0.4 m/s, p < 0.001).
Table 1
Baseline and follow-up echocardiographic findings and clinical outcomes according to the study groups

ACEI: angiotensin converting enzyme inhibitor, ARB: angiotensin receptor blocker, eGFR: estimated glomerular filtration rate, ESRD: end-stage regnal disease, HF: heart failure, LVEDVi: body surface area indexed left ventricular end-diastolic volume, LVEF: left ventricular ejection fraction, LVESVi: body surface area indexed left ventricular end-systolic volume, LVIDDi: body surface area indexed left ventricular internal dimension, end-diastole, LVIDSi: body surface area indexed left ventricular internal dimension, end-systole, MACCE: major adverse cardio-cerebrovascular event, NT proBNP: N terminal pro B type natriuretic peptide, TIA: transient ischemic attack TR Vmax: maximal velocity of tricuspid regurgitation.
![]()
 | Figure 1Scheme of study population. ΔLVEF: change of left ventricular ejection fraction, HFrEF: heart failure with reduced ejection fraction, PH: pulmonary hypertension, TR Vmax: maximal velocity of tricuspid regurgitation.
|
Adverse clinical outcomes
During the follow-up period (31 ± 20 months) from the follow-up echocardiography, 52 patients (19%) died, 65 (24%) had hospital admission for HF more than 1 episode and 17 (6%) admitted for stroke or TIA. Thus, 97 patients (36%) experience MACCEs. Group 4 had the lowest 5-year MACCE-free survival rate (19.0 ± 9.2%) than other groups (p < 0.001, Figure 2A). Patients with improvement of PH (62.7 ± 5.4% vs 38.2 ± 6.7%, p < 0.001) and improved LVEF (60.5 ± 4.8% vs 36.6 ± 7.9%, p < 0.001) had significantly higher 5-year MACCE-free survival rate than the other group (Figure 2B and 2C).
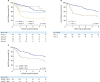 | Figure 2MACCE free survival according to the group by Kaplan-Meier survival analysis. Group 4 has the lowest 5- year MACCE-free survival rate (19.0 ± 9.2%) than other groups (A, p < 0.001 by Log-rank test). The group with improved PH (B, 62.7 ± 5.4% vs 38.2 ± 6.7%, p < 0.001 by Log-rank test) and improvement of left ventricular ejection fraction (C, 60.5 ± 4.8% vs 36.6 ± 7.9%, p < 0.001 by Log-rank test) have better 5-year MACCE-free survival rate than the other group. ΔLVEF: change of left ventricular ejection fraction, MACCE: major adverse cardio-cerebrovascular event, PH: pulmonary hypertension.
|
In the univariate analysis, age, male sex, hypertension, diabetes and NT proBNP concentration were associated with higher incidence of MACCE. Also, de novo HF, hemoglobin concentration, use of angiotensin converting enzyme inhibitor or angiotensin receptor blocker, improvement of LVEF and disappearance of PH were associated with lower MACCE (Table 2). Study group showed statistical significance, and group 4 had significantly higher MACCE rate. In the multivariate analysis, older age (hazard ratio [HR] = 1.045, 95% confidence interval [CI] = 1.023-1.072, p < 0.001) and study group remained statistical significance. Group 4 had statistically significantly lower MACCE free survival (HR = 4.332, 95% CI = 2.396-7.833, p < 0.001, Table 2).
Table 2
Univariate and multivariate analysis in the prediction of major adverse cardio-cerebrovascular event during five year
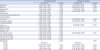
ACEI: angiotensin converting enzyme inhibitor, ARB: angiotensin receptor blocker, CI: confidence interval, HF: heart failure, HR: hazard ratio, LVEF: left ventricular ejection fraction, LVESVi: body surface area indexed left ventricular end-systolic volume, LVIDSi: body surface area indexed left ventricular internal dimension at end-systole, NT proBNP: N terminal pro B type natriuretic peptide, PH: pulmonary hypertension.
![]()
DISCUSSION
In this study, we evaluated changes in LVEF and PH from baseline to follow-up echocardiography in patients with HFrEF and PH, and showed that different long-term prognosis in patients with PH and HFrEF. Patients with improvement of LVEF and/or PH had better prognosis that those with persistent PH and LV systolic dysfunction.
The PH secondary to left-sided heart disease is classified as group 2 in the WHO classification.1)16) Within Group 2 PH, there are subtypes characterized by the presence or absence of pulmonary vascular disease.16) Left heart disease, including HFrEF, HF with preserved ejection fraction (HFpEF) and valvular heart disease results in an increase in left atrial pressure due to mainly diastolic dysfunction. The elevation of the left atrial pressure eventually increases the hydrostatic pressure in the pulmonary capillaries. Increased pulmonary artery pressure in patients with HF often represents a combination of increased left-sided filling pressures (passive component) and elevated pulmonary vascular resistance attributable to functional and structural abnormalities of the pulmonary vascular bed (reactive component).17)
PH due to left heart disease is common in HFrEF patients and has been shown to be associated with worse clinical outcome.4)5)8)9)11)12)13)18) Aronson et al.9) first reported that TR Vmax > 2.5 m/s was associated higher mortality in patients with dilated cardiomyopathy. Since then, several studies have reported a strong association between PH and mortality and morbidity in HF patients. However, few studies have reported long-term prognosis according to the improvement of LVEF and/or PH. We have shown through this study that the improvement in PH was indicative of a better long-term prognosis in HFrEF patients with PH. Similar to our findings, Shalaby et al.19) reported that higher PASP at baseline was associated with worse survival in a study of cardiac resynchronization therapy recipients. They found that patients with reductions in PASP on the follow-up had better outcomes. In some patients with PH and HFrEF, acute phase with increased left atrial pressure may be reversible with standard HF treatment. However, chronic exposure to elevated pulmonary capillary wedge pressure may lead to permanent vascular remodeling, irreversibly.3)20) Although there may be differences depending on the timing of follow up echocardiography and patient status, we thought that reactive PH was the main mechanism in patients with persistent PH regardless of LVEF. Reactive PH means chronic PH and irreversible vascular remodeling and may have caused a bad prognosis. Aronson et al.9) reported similar results. In a subgroup analysis of 242 patients from the Vasodilation in the Management of Acute Congestive Heart Failure trial, reactive PH patients had higher mortality rate than passive PH patients.
Limitations
There are several limitations in our study. First, this is a retrospective observational study in single-center. A large number of patients were excluded because a follow-up echocardiography was not performed. Second, patients were not in the same states at the time of taking follow-up echocardiographic examinations. Some patients underwent follow-up examination at a stable state when heart failure was well controlled, while others were followed up for acute exacerbations such as worsening of symptoms, hospitalization, or other problems. Third, we used echocardiography in the diagnosis of PH with HFrEF. It may be less accurate than the invasive method. Right heart catheterization (RHC) is a gold standard in the diagnosis of PH and accurate method for the measurement of PASP.3) However, RHC is an invasive procedure with associated risks, complications and cost.21) Thus, RHC is not indicated all PH patients with HFrEF and is recommended in patients considered heart transplantation.1) Echocardiography is a useful non-invasive imaging modality for estimating PASP using the Doppler-derived technique and also provides valuable information of the cardiac structure and performance. It is important for identification of the cause of PH.22) Because of its non-invasiveness, echocardiographic examinations can be performed repeatedly without giving no harm to patients. Further prospective studies with standardized protocols are needed to solve these limitations.
Conclusion
In patients with HFrEF and PH associated with HFrEF, the improvement of PH and LVEF were associated with favorable outcomes. The follow-up echocardiographic studies may help to determine prognosis in these patients by confirming the improvement of LVEF and PH compared with the baseline echocardiography.
 XML Download
XML Download