

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Computed tomography-guided percutaneous transthoracic needle biopsy (PTNB) has become a widely accepted technique for establishing a diagnosis in patients with pulmonary lesions due to its high accuracy, ranging from 83–97% (123). This procedure is minimally invasive, safe, and has a short recovery time and a low complication rate (4567).
When a diagnosis of malignancy is established by PTNB, the management algorithm is usually straightforward because of the low false-positive rate (0–0.2%) (8). When a specific benign diagnosis is rendered, such as hamartoma or granuloma, the result is usually considered a true reflection of the biopsied lesion. The presence of a positive biopsy culture (when there is no suspicion of post-obstructive pneumonia) supports the likelihood of a benign lesion due to the low likelihood of a false positive culture (9). However, when a non-diagnostic result is obtained, uncertainty may arise over how to proceed.
Although PTNB is widely performed in daily practice, only a limited number of studies have analyzed the final diagnoses of non-diagnostic biopsies. Prior studies have reported a high percentage of non-diagnostic cases, up to 15% (10), which may result in a delay in diagnosis and treatment. Most of these prior studies were limited by a small number of cases or were focused on specific lesions, such as ground glass lesions or suspected infection. One of the largest studies included patients from three different centers and samples from lung, mediastinal, and pleura to achieve a study group of 980 cases (9). A more recent multicenter study examining the malignancy risk of non-diagnostic PTNB of lung lesions included patients from eight different centers and utilized many different imaging modalities to obtain a study group of 9384 cases (11).
We therefore performed a large single-center analysis of PTNB of lung-only lesions to determine the predictive factors for a non-diagnostic result and the final diagnosis of pulmonary lesions with an initial non-diagnostic CT-guided PTNB result.
Go to : 
MATERIALS AND METHODS
This study was designed as a retrospective single-center study and performed in accordance with the Health Insurance Portability and Accountability Act. Due to the retrospective nature of the study protocol, the Institutional ethical Review Board waived the need for informed consent.
Medical Record Review
Medical records and chest CT images of all patients who underwent a CT-guided PTNB between July 2009 to June 2013 were retrospectively reviewed by two board certified chest radiologists, both with 3 years of experience in chest radiology. A total of 894 consecutive CT-PTNBs were performed over the 4-year period in a single academic thoracic radiology institution.
The patients' records were reviewed to determine the histologic interpretation of the PTNB. The biopsy results were classified into the following three categories: malignancy, benign, and non-diagnostic. Malignancy included cases where malignant cells or cell suspicious for malignancy were described. Benign disease was defined as a benign neoplasm, such as hamartoma, a granulomatous lesion, such as sarcoidosis, a benign process, such as organizing pneumonia, or inflammatory cells with positive bacterial, fungal, or mycobacterial cultures. A non-diagnostic result was defined as the presence of normal respiratory elements, atypical cells, nonspecific inflammatory cells, blood, inadequate for interpretation, and cases where no specific diagnoses had been made.
The clinical variables, including age, sex, and history of prior malignancy, were also extracted from the patients' records. The radiologic variables analyzed for each patient included the size of the biopsied nodule, and whether the nodules were solid, part-solid, pure ground glass, or cavitary, or if a consolidation was biopsied. CT images obtained at the time of biopsy were reviewed. The biopsy-related variables included distance between the pleura and the nodule along the needle path, presence of emphysema along the needle path, whether the needle tip was in the lesion, and the procedure time (which was from the time of the initial localizing scan to the time when the last image was obtained prior to removing the needle). Any complications during or after the procedure were also recorded.
In the non-diagnostic cases, the final diagnosis was established either through surgical resection, repeat biopsy, or clinical and radiologic follow-up for least two years after the biopsy. A final diagnosis of benignity was made if 1) a specific benign diagnosis was made by pathology on the initial biopsy, re-biopsy, or surgical resection; 2) the lesion spontaneously resolved without chemotherapy or radiation; or 3) the lesion remained stable or decreased in size on imaging follow-up of at least two years. Those with imaging follow-up less than 2 years were excluded.
Needle Biopsy Technique
All biopsies were performed by one of six dedicated interventional thoracic radiologists with 10–25 years of experience. All procedures were performed under CT guidance using a 16-multidetector CT scanner (Lightspeed, GE Healthcare, Milwaukee, WI, USA). Patients were placed in the prone, supine, or oblique position, depending on the location of the lesion, to avoid crossing bullae, emphysema, and fissures. A localizing CT scan was performed using initially 5-mm and then 2.5-mm slices to decide on the point of entry and perform the biopsy.
The biopsies were performed under local anesthesia (1% xylocaine without epinephrine) and moderate sedation with intravenous midazolam and fentanyl. All biopsies were performed with a 19-guage thin-walled coaxial introducer needle (Chiba Ultrathin, Cook Medical, Bloomington, IN, USA). Once the needle was in the lesion, the inner stylet was removed and the 22-gauge Chiba needle (Cook Medical) was advanced through the lumen of the 19-gauge introducer-needle. Tissue samples were obtained in quick, short movements while suction was applied with an attached 10-mL syringe. To reduce the risk of air embolization, saline solution was placed in the well of the introducer needle during needle exchanges to provide a water seal (12).
Aspirates on sterile glass slides were reviewed by on-site cytopathologists to determine if diagnostic material was present. If infection was suspected or if malignancy was not confirmed by the on-site cytopathologist, further aspirates were obtained and sent to a microbiology laboratory. When appropriate and safe, core biopsy specimens were obtained using a 20-gauge biopsy needle (Cook Medical) with a 1- or 2-cm needle throw.
When an intraprocedural pneumothorax was present, if feasible, air would be aspirated as the needle was withdrawn. After removal of the biopsy needle, the patient was immediately rolled over to place the puncture site in the dependent position to minimize the risk of pneumothorax (13). The patient was encouraged to lie still and breathe gently during the 3-hour recovery period. Chest radiographs were obtained at 1 and 3 hours after the procedure.
Complications were categorized in accordance with the Society of Interventional Radiology clinical practice guidelines (14).
Statistical Analysis
Patients were classified into two groups according to the diagnostic performance (diagnostic vs. non-diagnostic) and final diagnosis of initially non-diagnostic biopsies (benign vs. malignant). We included all patients who underwent a CT-guided PTNB in the evaluation of predictive factors for a non-diagnostic biopsy. For the evaluation of final diagnosis of initially non-diagnostic biopsy, we excluded patients with a non-diagnostic biopsy and those in whom a final diagnosis could not be made, either because there was no diagnostic pathology by resection or repeat biopsy, or with imaging follow-up of less than two years.
Comparison of demographic data and target characteristics between the two groups was performed using binary logistic regression. Multivariable logistic regression, using variables yielding a p value of < 0.1 in the univariable logistic regression analysis, was performed to identify independent risk factors for diagnostic success. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. A p value less than 0.05 was considered statistically significant. All statistical calculations were performed using StataCorp. 2013. Stata Statistical Software (Release 13, StataCorp LP, College Station, TX, USA).
Go to :
RESULTS
Demographic Information
Between July 1, 2009 and June 30, 2013, 894 consecutive CT-guided PTNBs were performed in 861 patients. There were 149 non-diagnostic biopsies, yielding an overall non-diagnostic rate of 16.7% (149/894). Of 149 non-diagnostic biopsies, 27 were excluded because of follow-up less than 2 years. Thus, there were 867 biopsies which had been performed in 834 patients, 122 of which were non-diagnostic. Thirty-three patients had two biopsies of the same lesion, which were counted as separate events. There were 383 males and 451 females with patient ages ranging from 18 to 92 years (mean age, 67 ± 26 years). The distribution of all biopsy results is detailed in Figure 1. The final diagnosis was malignancy in 85% (734/867) (Fig. 2) and benign disease in 15% (133/867) of all biopsies (Fig. 3). The distribution of malignancy, including primary lung cancer, lymphoproliferative disease, and metastasis in both diagnostic and non-diagnostic biopsies is detailed in Table 1.
 | Fig. 1Flow diagram shows diagnoses and distribution of initial biopsy results of 894 consecutive biopsies.CLL = chronic lymphocytic leukemia, DLBCL = diffuse large B-cell lymphoma, PTNB = percutaneous transthoracic needle biopsy
|
 | Fig. 261-year-old woman with carcinoid tumor.Prone unenhanced chest CT scan obtained during PTNB revealed left lower lobe nodule surrounded with minimal alveolar hemorrhage. Diagnosis was made on FNA. FNA = fine needle aspiration
|
 | Fig. 377-year-old man with amyloidoma.Prone unenhanced chest CT scan obtained during PTNB revealed right upper lobe nodule with calcification. Diagnosis was made on CNB. CNB = core needle biopsy
|
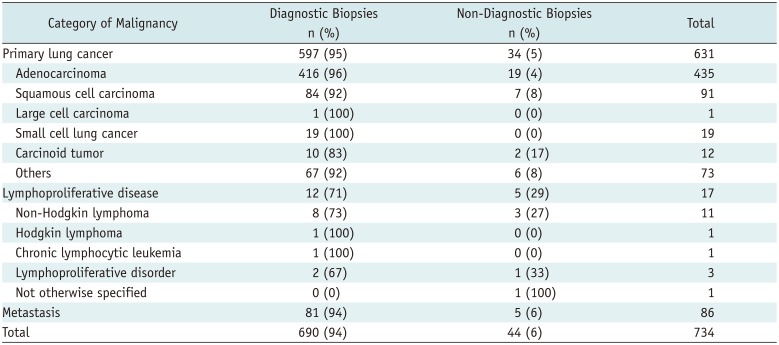
Table 1
Distribution of Malignant Diagnoses for Both Diagnostic and Non-Diagnostic Biopsies
![]()
Diagnostic Versus Non-Diagnostic Biopsies
The difference in non-diagnostic biopsy rates for patients with a malignant final diagnosis (44/734, 6%) and benign lesions (78/133, 59%) was statistically significant (p = 0.001). The differences in the non-diagnostic biopsy rates in the malignant group for primary lung cancer (34/631, 5%), lymphoproliferative disease (5/17, 29%), and metastasis (5/86, 6%) were statistically significant (p = 0.001). Among the lung cancers, carcinoid tumor had a higher percentage of non-diagnostic biopsy; however, the number of patients with carcinoid tumors was small.
There was a statistically significant difference in the non-diagnostic rates according to the lesion size, which were 19% (32/166) for lesions ≤ 15 mm and 13% (90/701) for lesions > 15 mm (p = 0.032). There were no statistically significant differences between the initially diagnostic and non-diagnostic groups in demographic data including age, sex, and lesion characteristics including attenuation, location, necrosis, and pleural contact.
There was a higher non-diagnostic rate when the biopsy needle traversed emphysematous lung parenchyma (18/74, 25%) compared to when it did not (104/793, 13%) (p = 0.008). The non-diagnostic rate was significantly higher when the introducer needle was outside the lesion (7/10, 70%) compared with when it was at the edge or within the lesion (115/857, 13%) (p = 0.001). There was also a significant difference in the non-diagnostic rates stratified by procedure time, which were 10% (48/504) for procedure time ≤ 60 minutes and 20% (74/363) for procedure time > 60 minutes (p = 0.001). There were no statistically significant differences between the initial diagnostic and non-diagnostic groups in other aspects of the biopsy technique, including the patient position, needle traversing aerated lung, and needle path length. There was also no statistically significant difference between these two groups based on the operator's experience (p = 0.907).
Among the 867 biopsies, 100% (867/867) had fine needle aspiration (FNA), 43% (371/867) had core needle biopsy (CNB), and 27% (230/867) had microbiology. The differences in the non-diagnostic biopsy rates for patients undergoing FNA with CNB (48/371, 13%) and FNA without CNB (74/496, 15%) were not statistically significant (p = 0.406). This remained true when the malignant final diagnosis and benign final diagnosis groups were reviewed separately (p = 0.551 and p = 0.521, respectively).
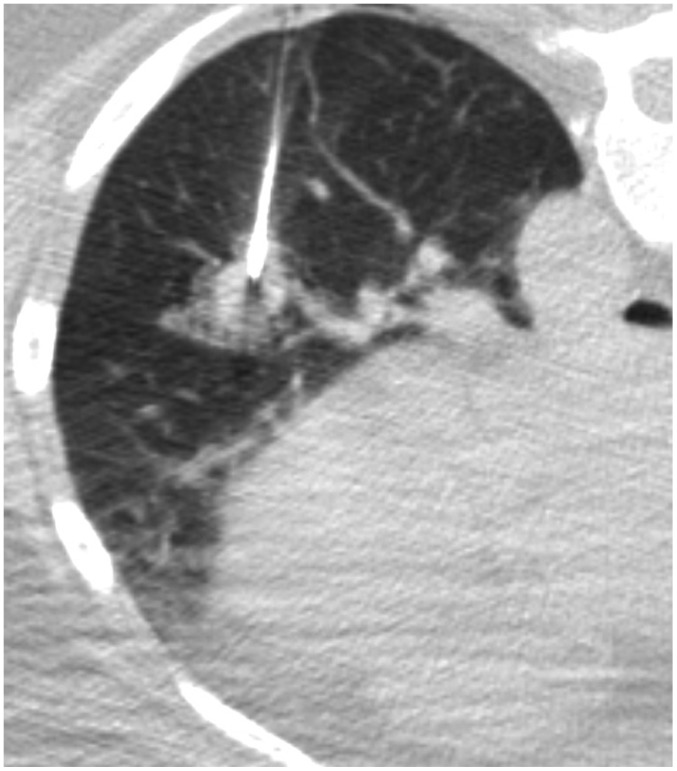
A pneumothorax was detected in 207 cases (24%) and 20 cases (2%) required chest tube drainage. There was a significant difference in pneumothorax rate between cases in which the needle traversed emphysema (33/74, 45%) and cases in which it did not (174/793, 22%), respectively (p = 0.001) (Fig. 4). However, there was no statistically significant difference in the non-diagnostic rate between the presence (18%, 37/207) or absence (13%, 85/660) of pneumothorax (p = 0.071).
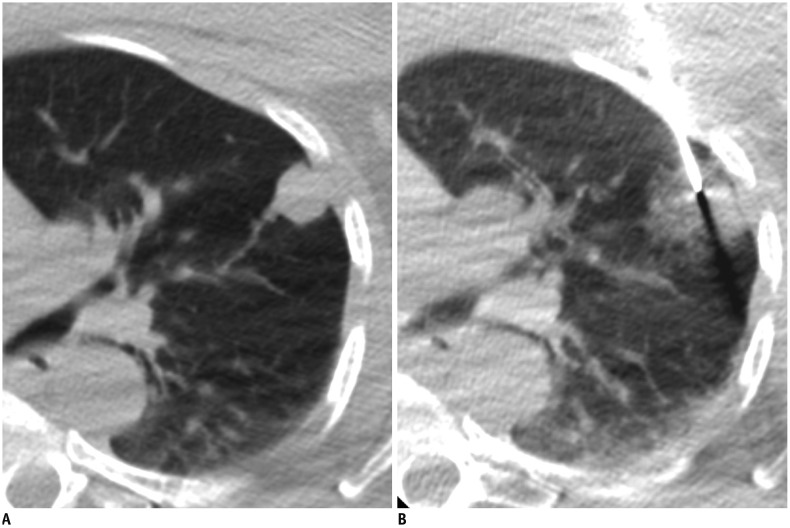
 | Fig. 477-year-old woman with final diagnosis of squamous cell carcinoma.
(A) Localizing CT scan showed 1.4-cm central right lower lobe nodule (B) CT scan during biopsy revealed small pneumothorax and minimal alveolar hemorrhage around nodule and along needle tract. Fine needle aspirate was non-diagnostic and CNB was not performed. Final diagnosis was made at surgery.
|
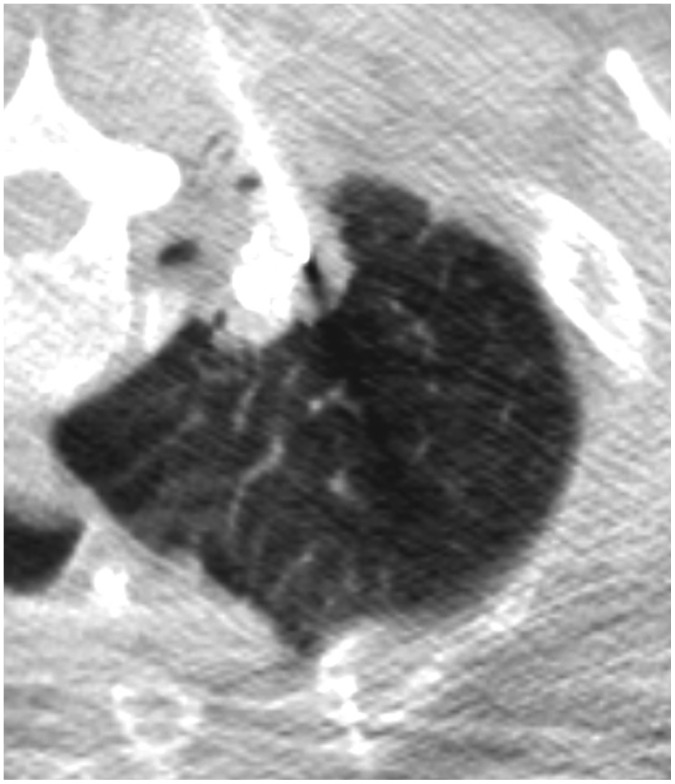
Mild perilesional hemorrhage was seen in the majority of cases (55%); however, self-limiting hemoptysis was seen in only 17 cases (2%). Non-diagnostic rates in patients with alveolar hemorrhage (83/478, 17%) were significantly higher than those in patients without alveolar hemorrhage (39/389, 10%) (p = 0.002) (Fig. 5). Hemothorax was detected in eight cases (1%), only one case (0.001%) required chest tube drainage and a blood transfusion. Table 2 details the demographic data, lesion characteristics, technique of PTNB and complications of initially diagnostic and non-diagnostic groups of 867 biopsies.
 | Fig. 556-year-old woman with final diagnosis of histoplasmoma.
(A) Localizing CT scan revealed 1.6-cm peripheral nodule in left upper lobe (B) CT scan obtained during biopsy revealed minimal alveolar hemorrhage around nodule. PTNB (both FNA and CNB) was non-diagnostic and final diagnosis was made at surgery.
|
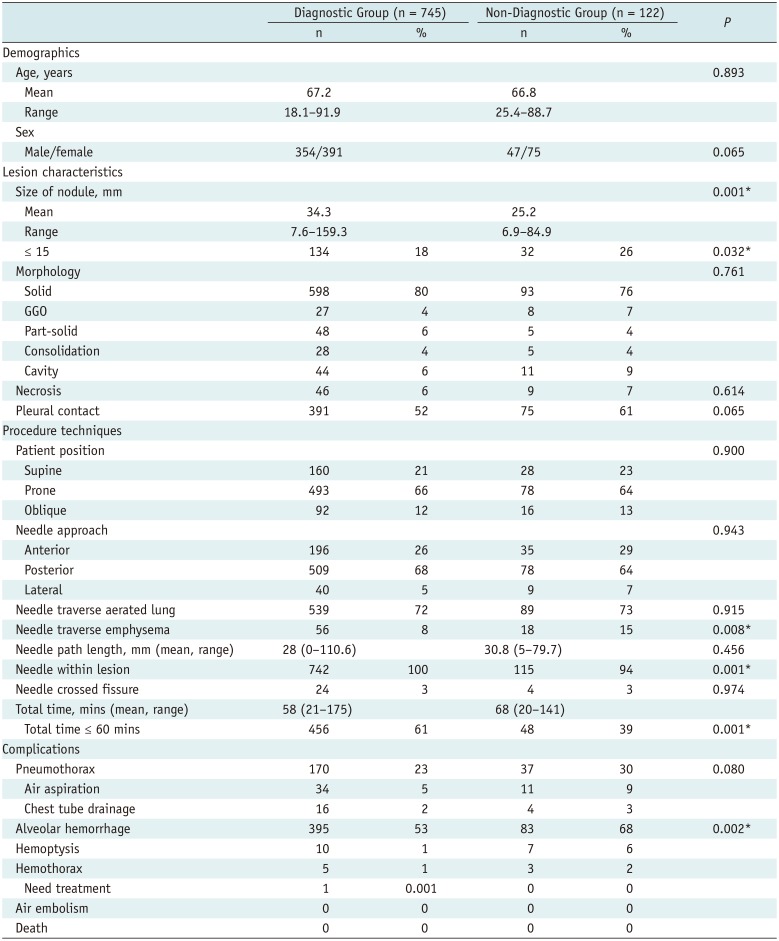
Table 2
Demographics, Characteristics, Technique of PTNB and Complications Associated with Initial Diagnostic and Non-Diagnostic Results
![]()
A multivariable regression model was made including sex, lesion size, pleural contact, procedure length, needle traversing emphysema, needle within the lesion, pneumothorax and alveolar hemorrhage as significant univariate regression variables. In this model, we could demonstrate that smaller lesion size (OR 1.027; 95% CI 1.011–1.044; p = 0.001), the presence of pleural contact (OR 0.359; 95% CI 0.277–0.568; p = 0.001), needle traverse emphysema (OR 0.424; 95% CI 0.229–0.785; p = 0.006), needle not within the lesion (OR 12.562; 95% CI 3.167–49.829; p = 0.001) and longer procedure time (OR 0.983; 95% CI 0.974–0.992; p = 0.001) were independent risk factors for a non-diagnostic biopsy in our study.
Non-Diagnostic Biopsies
Thirty-six percent (44/122) of non-diagnostic biopsies ultimately yielded a diagnosis of malignancy. The only statistically significant difference in the demographic data between the benign and malignant groups was the age (p = 0.027). There were no statistically significant differences in the other demographic data, including sex, smoking history, and lesion characteristics and how the nodule behaved on imaging prior to the PTNB. Table 3 details the demographic data and lesion characteristics of malignant and benign groups in the 122 non-diagnostic cases.
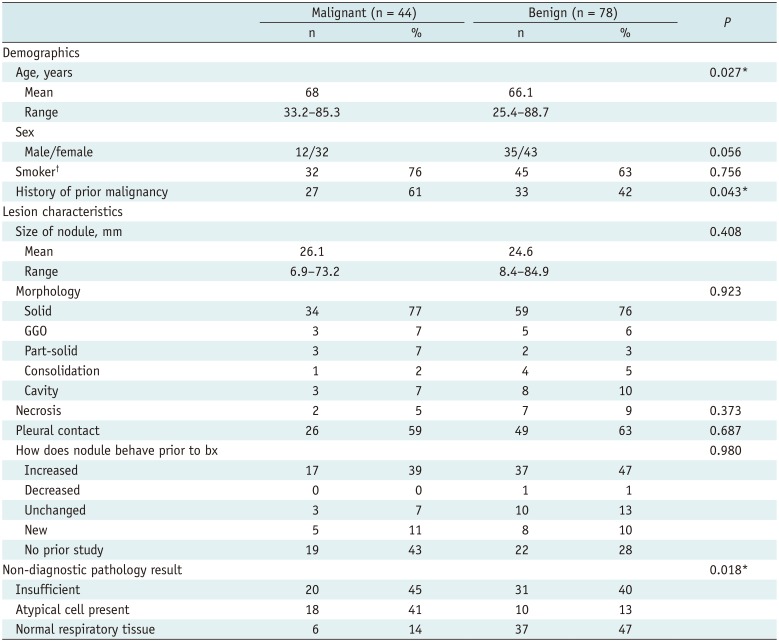
Table 3
Characteristics Associated with Final Malignant and Benign Diagnoses of 122 Non-Diagnostic Biopsies
![]()
Of 60 patients with a history of prior malignancy (60/122, 49%), 27 cases were malignant (45%) and 33 were benign (55%). In the 62 patients without a prior history of malignancy, 17 cases were malignant (27%) and 45 were benign (73%). This difference in final diagnosis of malignancy between those with a history of malignancy and those without history of malignancy was statistically significant (p = 0.043).
Of the 122 non-diagnostic biopsies, 42% (51/122) had insufficient tissue for diagnosis, 23% (28/122) had atypical cells present, and 35% (43/122) described normal tissue elements in the pathology report. In cases where atypical cells were present, 64% (18/28) had a final diagnosis of malignancy, compared to 39% (20/51) of cases where there was insufficient tissue for diagnosis and 14% (6/43) in cases where normal respiratory tissue was obtained (p = 0.001).
Another multivariable regression model was constructed including age, sex, history of prior malignancy and non-diagnostic pathology result as significant univariate regression variables. In this model we could demonstrate that female gender (OR 0.382; 95% CI 0.161–0.905; p = 0.029), history of prior malignancy (OR 2.756; 95% CI 1.212–6.627; p = 0.016), and presence of atypical cells (OR 0.541; 95% CI 0.334–0.877; p = 0.013) were significant independent risk factors for a final diagnosis of malignancy.
In the 44 cases of malignancy initially found to be non-diagnostic on PTNB, the final diagnosis was made at surgery in 26 cases, with re-biopsy in 10 cases, and clinical-radiologic follow-up in 8 cases. In the 78 benign cases initially found to be non-diagnostic on PTNB, the final diagnosis was made at surgery in 22 cases, and clinical-radiologic follow-up in 56 cases. The median and interquartile range of follow-up duration of all 122 initially non-diagnostic biopsies was 227 days and 1161 days, respectively, and for the 64 cases in which the final diagnosis was made by clinical-radiologic follow-up was 1164 and 1080, respectively. Table 4 details the main method by which the final diagnosis was determined after the initial non-diagnostic biopsy.
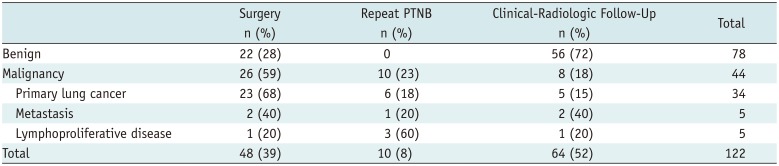
Table 4
Non-Diagnostic Biopsies and Methods by Which Their True Diagnoses Were Determined
![]()
Go to :
DISCUSSION
PTNB of the thorax is commonly performed to obtain the diagnosis of pulmonary lesions discovered on imaging. However, when the PTNB result is non-diagnostic, a clinical decision must be made as to whether the patient needs repeat PTNB, surgical intervention, bronchoscopy, serial imaging, or empiric therapy. Knowledge of the outcome and predictive factors of non-diagnostic biopsies can help inform such patient management decisions.
Prior studies have calculated that the non-diagnostic rate of CT-guided PTNB ranges from 1.3–15% (21011151617). Studies evaluating outcomes after a benign nonspecific biopsy found that false negative rates varied between 7–29% (18192021). The sensitivity of FNA (with or without CNB) in evaluating benign thoracic diseases varied from 17–91% (222324).
In our four-year retrospective analysis of 894 CT-guided PTNBs, there were 149 non-diagnostic biopsies for a non-diagnostic rate of 16.7%. Our slightly higher non-diagnostic rate may be due to a broader definition of a non-diagnostic biopsy compared to that in prior studies. Quint et al. (15) categorized biopsy results into malignant, benign specific, benign non-specific, and non-diagnostic categories. In their study, non-diagnostic was defined as a case with only normal pulmonary tissue and/or insufficient tissue to render a diagnosis. We considered the benign nonspecific group also as a non-diagnostic result because the management and clinical implications of benign nonspecific and non-diagnostic categories were similar. Our non-diagnostic rate was lower than that in a recently published study of malignancy risk of non-diagnostic PTNB of lung lesions in which 27.6% of cases were non-diagnostic (11). This difference may be related to their inclusion of patients who underwent fluoroscopy- and ultrasound-guided biopsy, as well as CT-guided biopsy. The difference in the non-diagnostic rate may also be explained by their categorizing granulomatous inflammation, abscess or organizing pneumonia as nonspecific benign results. The availability of onsite cytopathology may also explain our lower non-diagnostic rate.
Our total study population of 894 patients had a high rate of malignancy (85%). This is similar to the findings of Fontaine-Delaruelle et al. (10) who also reported a high rate of malignancy (79%) in a series of 980 PTNBs. In our initially non-diagnostic PTNBs, we found a 36% rate of malignancy underscoring the need for further evaluation and follow-up of non-diagnostic biopsies. Prior studies also showed a 29–50% rate of malignancy on initially non-diagnostic biopsies (101520). In our study, the false negative cases for malignancy were proven by surgery (59%), repeat biopsy (23%) or clinicoradiologic follow-up (18%). Repeat biopsy was performed in 16 patients of which 10 (63%) yielded a final diagnosis of malignancy. In prior studies, Fontaine-Delaruelle et al. (10) found that repeat PTNBs of the same target provided a final diagnosis in 95% of cases and Montaudon et al. (25) found a 100% negative predictive value on second biopsy. In our non-diagnostic cases, a malignant final diagnosis was more likely in patients with a history of malignancy and patients with atypical cells reported on pathology. Lee et al. (11) also reported a higher likelihood of malignancy in lesions categorized as atypical cell lesions, compared to that for lesions with insufficient specimens and nonspecific benign categories.
Of the patients with a malignant final diagnosis, we found that lymphoproliferative disease had a statistically higher non-diagnostic rate. Of the 17 patients ultimately diagnosed with a lymphoproliferative disease, the initial biopsy diagnosed only 71% (12/17), compared to 95% of primary lung cancers (597/631), and 94% of metastasis (81/86). The difficulty in diagnosing lymphoma on PTNB is consistent with a prior report of PTNB of mediastinal lymphoma (26). For patients with benign lesions, the rate of non-diagnostic PTNB was significantly higher (59%, 78/133) than that in patients with malignant lesions (6%, 44/734).
Predictive factors of non-diagnostic results included lesion size ≤ 15 mm, an introducer needle outside the lesion, a needle tract traversing emphysematous lung parenchyma, the presence of alveolar hemorrhage during the procedure, and a total procedure time > 60 minutes. A target ≤ 15 mm was also found to be predictive of a non-diagnostic biopsy result by Fontaine-Delaruelle et al. (10). An introducer needle inside the target is obviously important to achieve diagnostic material as reported by Klein and Zarka (27). Biopsy complications have also been previously reported to increase the likelihood of a non-diagnostic result (10). We found that the presence of alveolar hemorrhage independently increased the risk of a non-diagnostic result, possibly due to hemorrhage obscuring the lesion or early termination of the biopsy. Our study and prior studies showed that the presence of emphysema around a lesion increased the risk of pneumothorax (28); however, our study also showed an increased likelihood of a non-diagnostic result when the needle tract traversed emphysema (p = 0.008). There was also a higher rate of non-diagnostic biopsy when the total procedure time > 60 minutes. This longer procedure time may reflect the greater difficulty due to small size, difficult location, development of a complication, and/or the additional time required for the cytopathologist to process additional passes that are often required in non-diagnostic cases.
Some studies have found increased accuracy in both malignant and benign lesions when core biopsy is obtained in addition to FNA (2930). However, we found no statistically significant difference in the diagnostic performance between FNA alone and FNA with core biopsy. This is consistent with a systemic review by Yao et al. (30) which concluded there was insufficient evidence to support a difference in the diagnostic yield between FNA alone and FNA with core biopsy when diagnosing malignancy; however, they did comment that it appeared that core biopsy may be superior to FNA for classifying benign disease.
Our rate of pneumothorax was similar to that in prior reports ranging between 11.7–34% (710202231), with a low rate of chest tube drainage (2%) compared to prior studies (2531). Our incidence of mild perilesional hemorrhage (55%) was slightly higher than previously reported values (2325); however only 2% developed self-limited hemoptysis. Eight patients developed hemothoraces (1%), with chest tube drainage required in one patient (0.001%).
Our study has several limitations, the first of which is the retrospective design. Second, we were required to exclude 27 non-diagnostic biopsies (18%) due to the absence of a 2-year follow-up to determine a final diagnosis. Finally, our study was based on the experience of a single academic medical center with dedicated thoracic interventional radiologists and thoracic cytopathologists which may be different than practice at other medical institutions.
In conclusion, the predictive factors for a non-diagnostic biopsy were lesion size ≤ 15 mm, needle tract traversing emphysema, introducer needle outside the lesion, procedure time > 60 minutes, and presence of alveolar hemorrhage. Thirty-six percent of the non-diagnostic cases yielded a malignant diagnosis. In non-diagnostic cases with a history of malignancy, pathology showing atypical cells, or in cases where lymphoma is suspected, a repeat biopsy or surgical intervention should be considered due to the higher rate of malignancy. In cases where further intervention is not performed, we recommend repeat imaging to document stability or resolution of the lesion. If a lesion demonstrates growth, then a repeat biopsy or surgical intervention should be considered.
Go to :
 XML Download
XML Download