

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery fistula (CAF) is a rare disease characterized by abnormal communication between the coronary artery and the heart chamber or the great vessels. It is usually congenital, but in some cases, it may be acquired. The exact prevalence is unknown, but CAF has been reported to occur in approximately 0.1% to 0.2% of all patients who underwent invasive coronary angiography (1). Further, the prevalence of CAF was reported to be up to 0.9% when it was detected as an incidental finding during coronary computed tomography angiography (CCTA), which has been widely used in recent years (23). The coronary-to-pulmonary artery fistula (CPAF) is the most common type of CAF found incidentally on CCTA, with a prevalence ranging from 0.17% to 0.68% (2345). Several studies have investigated the morphological characteristics of CPAF by using CCTA (5678).
The natural history of CPAF found incidentally on CCTA is unknown. Although CPAF is known to be asymptomatic in most cases, it has been reported to be associated with severe complications such as rupture of the aneurysm, ischemic heart disease, sudden cardiac death, pulmonary hypertension, and congestive heart failure in some cases (9101112131415161718). Studies have suggested that small fistulas can slowly increase in size, although most fistulas showed minimal changes over a period of 10 to 15 years (19).
Even though standardized treatment guidelines for the management of CPAF have not been established, it has been suggested that several factors such as the size of the fistula, hemodynamic changes on echocardiography, the presence of ischemia on myocardial perfusion imaging, and associated cardiac anomalies can be determinants for the choice between conservative treatment and invasive procedures (19). The most commonly used surgical treatment is fistula ligation (2021). However, endovascular interventional procedures can be successfully performed in some cases (2223). Antiplatelet agents or anticoagulants are often recommended for conservative treatment. However, most of these management strategies are controversial, since they are based on a relatively small number of retrospective studies. In this study, therefore, we aimed to analyze the natural clinical course of patients diagnosed with CPAF by using CCTA in two institutions and to suggest appropriate therapeutic strategies in these patients.
Go to : 
MATERIALS AND METHODS
The Institutional Review Boards of both institutions approved this retrospective study and the boards waived the requirement for informed consent.
Study Population
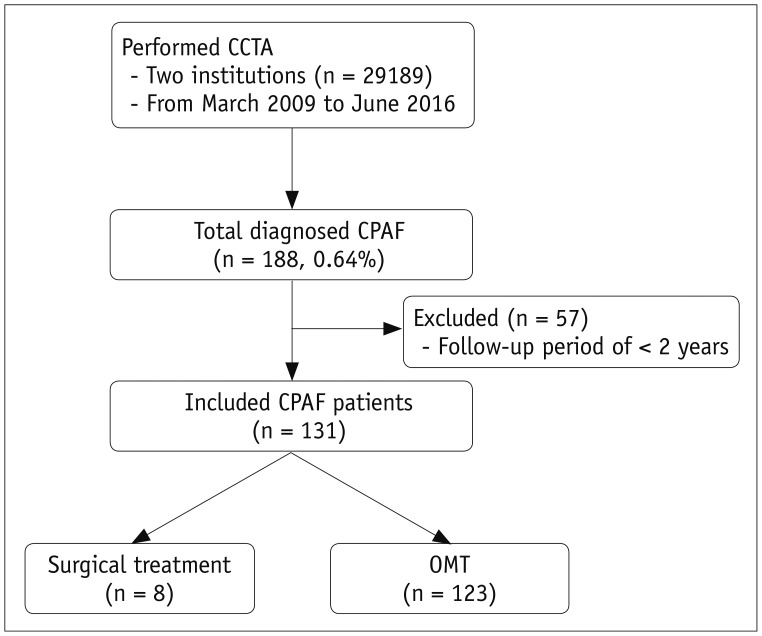
Two tertiary hospitals (Seoul St. Mary's Hospital and Samsung Medical Center) in Korea participated in this study. CPAF was defined as a communication between one or more coronary arteries and the pulmonary artery on CCTA. We retrospectively reviewed the CCTA reports generated by cardiovascular radiologists from March 2009 to June 2016 (Fig. 1). During this period, a total of 29189 patients underwent CCTA in two institutions (11956 and 17233 each). Among them, CPAF was diagnosed in 188 patients on CCTA (86 and 102 each). We excluded 57 patients who underwent less than 2 years of follow-up (FU). The FU period was defined as the period from the date of diagnosis to the date of the last medical record. Finally, 131 patients were included in the study. Data including age, sex, presence of underlying diseases, presence of coronary artery disease (CAD), awareness of CPAF before CCTA, smoking history, clinical history, prior cardiac testing, and reasons for undergoing CCTA were collected by a thorough review of the patients' electronic medical records. Underlying diseases included diabetes, hypertension, and hyperlipidemia. CAD was defined as a luminal narrowing of ≥ 50% on CCTA or invasive coronary angiographic images. Prior cardiac testing included myocardial perfusion single-photon emission computed tomography (SPECT), treadmill test, stress echocardiography, and invasive coronary angiography.
The CCTA findings of 43 and 17 patients included in the current study have been reported in two previous studies, respectively (824). In one publication, we reported the prevalence and types of CAFs detected with CCTA (8), while the hemodynamic characteristics of CPAF were evaluated using thallium-201 SPECT in the other publication (24). For the current study, we further used these data to evaluate the natural clinical history of CPAF detected on CCTA and proposed potential treatment strategies.
Image Acquisition
All CCTA scans were performed with dual-source CT scanners at the two institutions. The detailed scanning parameters are presented in Table 1. All images from both institutions were transferred to an external workstation equipped with image processing software (Advantage Workstation 4.3, GE Healthcare, Milwaukee, WI, USA; Syngo Multimodality Workplace, version 2008, Siemens Healthineers, Erlangen, Germany; Aquarius 3D Workstation, TeraRecon, San Mateo, CA, USA).
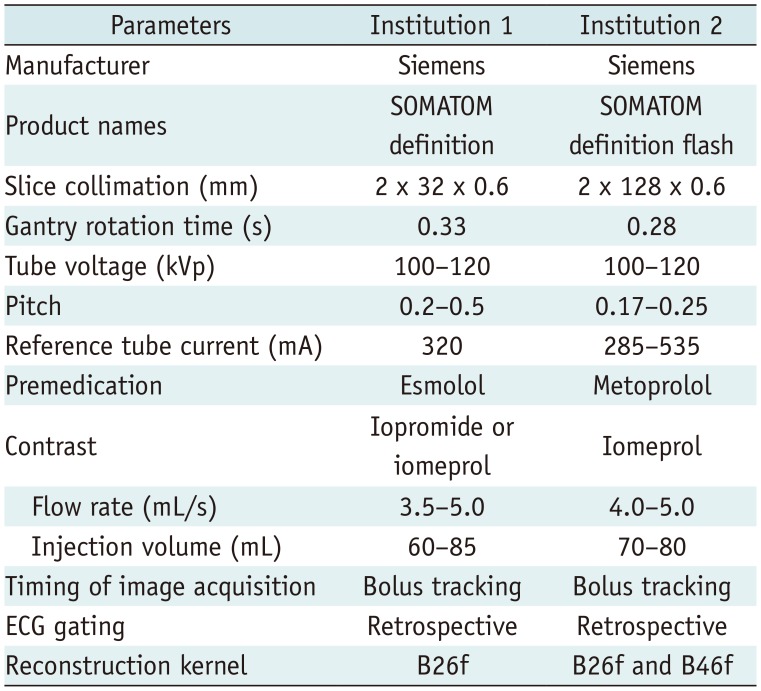
Table 1
Scanning Parameters of CCTA
![]()
Image Analysis and Follow-Up
The following morphologic features of CPAFs were analyzed with consensus by radiologists with cardiac imaging experience of 14 years and 1 year: the vessel of origin, size, and presence of an aneurysmal sac. Fistula size was determined by the largest diameter of the originating vessel and the aneurysmal sac was defined as a dilation that was 1.5 times larger than the adjacent vessels.
The type of treatments administered after the diagnosis of CPAF and the occurrence of major late complications during the FU period were evaluated. Patients were divided into two groups according to treatment methods: surgical ligation and observation with optimal medical treatment (OMT). The occurrence of major late complications was considered as a major adverse cardiac event (MACE), which included death, myocardial infarction, or the need for revascularization or percutaneous intervention. To avoid the interference of confounding factors such as CAD or hypertension, we carefully interpreted the occurrence of MACE in relation to the clinical situation. Furthermore, for patients who had undergone FU CCTA imaging after the diagnosis of CPAF, morphological changes in CPAF on the FU CCTA were assessed.
Statistical Analysis
Continuous variables are presented as medians (25th–75th percentile ranges) and categorical variables are expressed as frequency (percentage). We analyzed the differences in the demographic and morphologic features of CPAF between the two treatment groups by using the Mann–Whitney U test for analysis of continuous data and the Fisher's exact test or chi-squared test for categorical data. The association between surgical treatment and various factors such as age, sex, underlying disease, smoking history, symptoms, and morphologic features of CPAF was estimated using a logistic regression analysis with backward elimination. All statistical analyses were performed with the free statistical software R (version 3.5.3, The R Project for Statistical Computing, Vienna, Austria), and a p value < 0.05 was considered statistically significant.
Go to :
RESULTS
Patient Demographics
Table 2 shows the demographic characteristics of the entire study population and a comparison between the two treatment groups. The median age of all patients was 63.0 years (range, 57.0–72.0 years), and the mean FU period was 5.72 years (range, 4.08–6.96 years). There were 65 men with a median age of 62.0 years (56.0–72.0 years) and 66 women with a median age of 65.0 years (58.3–72.0 years). The most common underlying disease was hypertension (n = 60, 45.8%), followed by hyperlipidemia (n = 40, 30.5%) and diabetes mellitus (n = 21, 16.0%). There were 28 patients (21.4%) with CAD. Four patients (3.1%) were already aware of the CPAF before CCTA. The most common prior cardiac testing procedure was invasive coronary angiography (n = 27), followed by the treadmill test (n = 26), myocardial perfusion SPECT (n = 18), and stress echocardiography (n = 7). The most common reasons for performing CCTA were chest pain (n = 57), asymptomatic screening (n = 27), preoperative evaluation (n = 17), palpitation/arrhythmia (n = 14), dyspnea (n = 12), and syncope (n = 5). There was a significant difference in the rate of awareness of the CPAF before CCTA between the surgical ligation and OMT groups (p = 0.030).
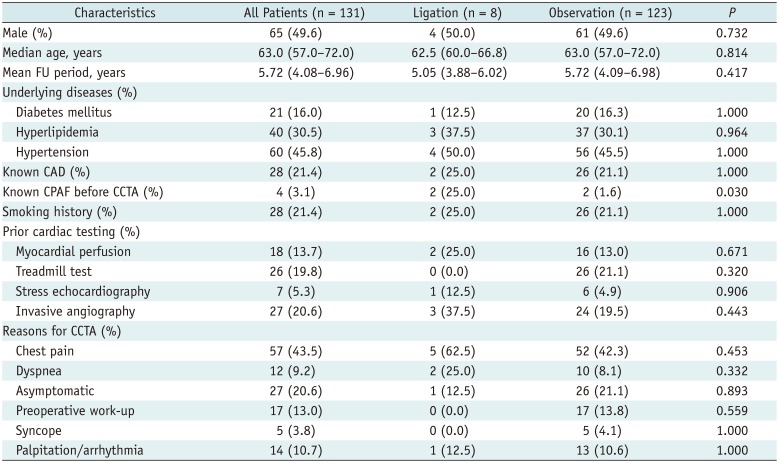
Table 2
Patient Demographics and Clinical Characteristics
![]()
Coronary-to-Pulmonary Artery Fistulas
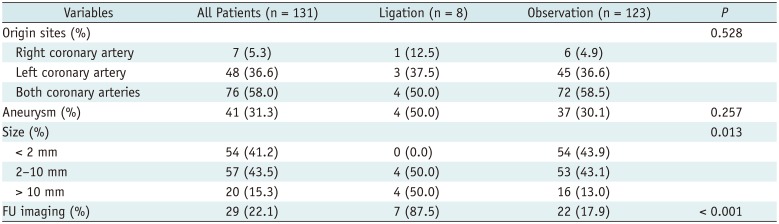
In the 131 CPAF cases detected, 76 fistulas (58.0%) originated from both coronary arteries, 48 from the left coronary artery, and only 7 from the right coronary artery (Table 3, Fig. 2). Approximately half the fistulas (n = 54, 41.2%) were less than 2 mm in size, while those in 57 cases were 2 to 10 mm in size. Only 20 fistulas were more than 10 mm in size. In 41 patients (31.3%), the CPAF was associated with aneurysmal dilatation.
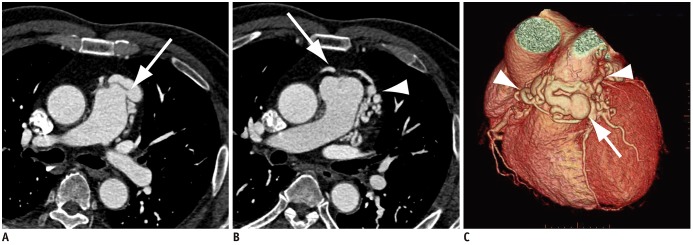 | Fig. 2CCTA images of 62-year-old man with CPAF.Axial CCTA images show fistula draining from left coronary artery to main pulmonary artery (arrow, A) with several small aneurysmal dilatations (arrowhead, B). Other fistula tract originating from right coronary artery is also seen (arrow, B). C. Three-dimensional volume-rendered image clearly shows CPAF supplied by right coronary artery and left coronary artery (arrowheads) with aneurysmal dilatation (arrow).
|
Table 3
Comparisons of Origin Sites, Presence of Aneurysm, and FU Imaging Data between Two Treatment Groups
![]()
Treatments and Prognosis
Of the 131 patients, 8 (6.1%) underwent surgical fistula ligation. Although the decision regarding the treatment method was made on the basis of the subjective judgements or discretion of the cardiologist and cardiovascular surgeon, our analysis also showed that the size of the fistula was significantly different between the two treatment groups (p = 0.013) (Table 2). The origin site and presence of an aneurysm were not different in the two groups. Logistic regression analysis demonstrated a significant association between the fistula size and surgical treatment (odds ratio = 1.14, p = 0.021), but statistical analysis was limited due to incomplete data (only a small number of patients underwent surgical treatment). Symptoms disappeared after surgery in all eight patients. One patient developed palpitation as a new symptom postoperatively, which resolved after radiofrequency catheter ablation of the left atrium.
The remaining 123 patients were managed with OMT. Drugs such as beta-blockers, calcium channel blockers, anti-hyperlipidemic agents, and antiplatelet agents were used for OMT. Only one patient in the observation with OMT group reported a MACE. This patient was a 71-year-old woman incidentally diagnosed with a small CPAF of less than 2 mm on FU imaging after coronary artery bypass grafting (CABG) surgery; she needed a revascularization intervention after one year of FU. However, none of the patients treated with fistula ligation surgery experienced MACE during the FU period.
Of the 131 patients, 29 (22.1%) underwent FU CCTA imaging one or more times after the CPAF diagnosis. The median interval between diagnosis and imaging FU in these patients was 3.81 years (range, 13 days to 7.18 years). None of the 22 patients in the OMT group showed a definite change in the morphological features of CPAF on FU CCTA imaging. FU imaging examinations were performed in these patients because of other reasons such as regular FU after CABG surgery, Takayasu's arteritis, CAD, and heart valve disease, rather than CPAF.
In the surgical ligation group, seven patients (87.5%) underwent post-operative CCTA imaging, and only one patient demonstrated recurrence of a small CPAF (less than 2 mm in size), but the patient was asymptomatic. No residual fistula or recurrence was found in the remaining six patients in the surgical ligation group.
Go to :
DISCUSSION
Our study suggests that CPAFs diagnosed incidentally on CCTA are mostly benign. Of all 131 patients, only one patient in the OMT group reported MACE, which required intervention for occlusion of the arterial bypass from the left internal mammary artery to the left anterior descending artery. In this case, it was unlikely that the MACE was due to the CPAF, considering the size of the CPAF (less than 2 mm) and the patient's clinical history of severe CAD and previous surgical history of CABG. These results are consistent with the findings of previous studies that evaluated all types of CAFs, including CPAF, and another study that only evaluated CPAF (192526).
In most patients with imaging FU data, no significant morphological changes were observed in CPAF. Though the FU period was relatively short and varied, it appears that morphological changes in the CPAF do not occur rapidly over a short period of time, especially in adults. In the future, research with long-term imaging FU may be needed.
Of the 123 patients who were managed with OMT alone without any surgical intervention, 122 did not experience MACE, and their symptoms were well controlled with OMT. These results indicate that medical treatment alone is sufficient in most cases for the treatment of CPAF discovered incidentally on CCTA. Previous studies have suggested the use of beta-blockers, calcium channel blockers, and antiplatelet agents to prevent thrombosis as non-surgical treatment options (25262728293031). Our study also reaffirmed that these drugs are effective in controlling the symptoms of CPAF.
It is important to differentiate between patients who require surgical treatment and those who do not. The American Heart Association 2018 guidelines refer to a study that showed that myocardial infarction can occur after surgical treatment of CAF (3233). Some studies have recommended surgical treatment in cases of severe systemic shunt, right ventricle volume overload, ischemia, and congestive heart failure (27303435). One recent study reported that myocardial perfusion SPECT might be a useful non-invasive tool for evaluating hemodynamic status and for risk stratification in patients with CPAF (24); perfusion abnormalities correlated with symptoms, and they improved after surgical treatment. Our study showed an association between fistula size and surgical treatment. Hence, we presume that a large fistula size might be a real-world determinant for surgical treatment.
Percutaneous transcatheter closure is suggested for patients with a proximally located fistula or a single drainage site and for those with a high perioperative risk profile for open surgery (2526). The recurrence rate after CPAF ligation surgery was 12.5% in our study (one out of eight cases), which seems to be consistent with the rate of recurrence reported in previous studies, up to 20–30% (2536).
This study had several limitations. First, there is the possibility of selection bias due to the retrospective nature of our study. Although we assumed that clinicians made their judgments based on fistula size and symptoms (based on electronic medical records), they decided the treatment method based on their discretion. Therefore, future prospective studies are strongly warranted to set up consistent criteria for surgical treatment. In addition, although this was a multicenter study, recruiting patients from only tertiary hospitals could have caused another selection bias. Second, the number of patients in whom morphological changes in the CPAF were definitely confirmed by FU imaging studies was relatively small, and the FU period was insufficient considering the slowly progressive nature of the disease. Finally, statistical comparison between the two treatment groups was difficult, because the number of patients in the surgical group (n = 8) was too small compared to that in the OMT group (n = 123).
To the best of our knowledge, most of the similar studies conducted so far have included all types of CAF cases. The significance of this study is that it evaluates only cases of CPAF found on CCTA and includes a relatively large number of cases obtained from two institutions. Therefore, the results of the study could be used for establishing patient treatment guidelines.
In conclusion, CPAFs detected on CCTA are usually benign, and OMT may be sufficient in most cases. Fistula size could be a determinant for surgical ligation.
Go to :
 XML Download
XML Download