

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Bombay and para-Bombay phenotypes are rare blood groups that have inherent defects in producing H antigens. The molecular basis of these rare blood types has been proven to be mutations of the FUT1 (H gene) or FUT2 (Se gene).1234 The para-Bombay type is different from the Bombay type in that the former has H antigens in secretions, whereas the latter does not.1
The first report of this rare blood type was from India in 1952.5 Following this, there have been several reports regarding these rare blood groups; to the best of our knowledge, none have been reported from Korea.678910 Herein, we report the case of a Southeast Asian patient admitted at a tertiary hospital in Korea with a para-Bombay phenotype.
CASE DESCRIPTIION
In December of 2018, a 23-year-old Indonesian man presented to Asan Medical Center with a 2-week history of fever, chills, and headache. He entered Korea 2 years previously. He had never received a blood transfusion. Initial blood tests revealed anemia and thrombocytosis. The initial laboratory test results were as follows: white blood cells, 14.8 × 109/L; hemoglobin, 8.2 g/dL (82 g/L); platelets, 624.0 × 109/L; mean corpuscular volume, 79.0 fL; mean corpuscular hemoglobin, 24.8 pg; mean corpuscular hemoglobin concentration, 31.4%; iron, 16 µg/dL (160 µg/L); total iron binding capacity, 156 µg/dL (1,560 µg/L) and ferritin, 1,267.9 ng/mL. Nontuberculous mycobacteria (NTM) isolates were identified in an axillary lymph node biopsy specimen using the nested MTB & NTM Kit (BioSewoom Inc., Seoul, Korea). He was diagnosed with disseminated NTM infection and was then treated accordingly.
The patient subsequently developed anemia of chronic disease combined with iron deficiency anemia and therefore a blood transfusion was recommended due to severe microcytic anemia. Blood typing was performed using IH-1000 (Bio-Rad Laboratories Inc, Hercules, CA, USA). His RBCs showed no reactivity against both anti-A and anti-B serum, while his serum showed agglutination with only B cells. The result of the pretransfusion RBC antibody screening test (ID-DiaCell I-II, BIO-RAD; Hercules) was negative.
Manual tube testing was then performed to resolve the discrepancy. Forward grouping showed no agglutination with monoclonal anti-A and anti-B serum (SIHDIA Anti-A and Anti-B; Shinyang diagnostics, Seoul, Korea). Reverse grouping using A1 and B cells (iMR.A1-B; MIRR. SciTech Corp., Seoul, Korea) showed trace and 4+ agglutinations with group A1 and group B cells, respectively. When we incubated the serum with RBCs for an extra 15–30 minutes, the results did not change. After cold adsorption and elution of RBCs with anti-A, the eluate showed trace agglutination with A1 cells. H antigen tests using two different antiserum (Lorne laboratories, Danehill, United Kingdom; ANTITOXIN GmbH, Bammental, Germany) revealed that the patient's RBCs did not express H antigens (Table 1). Crossmatching with 10 units of O type RBCs showed consistently incompatible results with a grade ± ~2+ agglutination of O type RBCs in the saline phase and 22% in the bovine albumin and antiglobulin phase.
Table 1
Results of ABO blood group typing

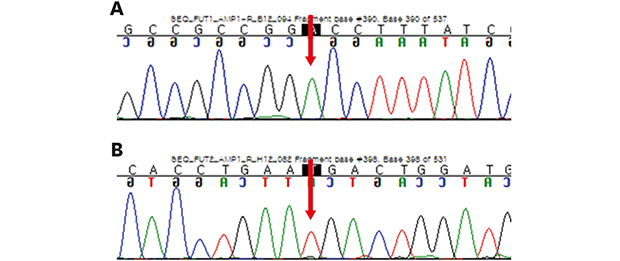
ABO genotyping using sequencing for exon 6, exon 7 and their flanking regions revealed that the patient had an A/O allele combination. Direct sequencing analysis for coding regions and their flanking areas of FUT1 and FUT2 were performed.9 We found one missense variation, NM_000148.3:c.328G>A (p.Ala110Thr, rs56342683, FUT1*01W.02), as a homozygote in FUT1. A synonymous variant, NM_000511.5:c.390C>T (p.Asn130=, rs281377, Se357), was found in FUT2, also in the homozygous state (Fig. 1). Based on these results, the patient's blood group was confirmed to be para-Bombay type.
Fig. 1
Sequencing chromatograms of analyzed genes. (A) Result for FUT1 and (B) result for FUT2. The arrows indicate the variants in FUT1 (c.328G>A, p.Ala110Thr) and FUT2 (c.390C>T, p.Asn130=). Each variant represents FUT1*01W.02 and Se357 allele, respectively.

Because compatible blood could not be found and familial donors were unavailable, he was administered intravenous iron sucrose (Venoferrum; Vifor International, Ltd., St Gallen, Switzerland) for five consecutive days for treating anemia. After 15 days of admission, the hemoglobin level increased to 7.9 g/dL, and his clinical symptoms were relieved. He was discharged without receiving the RBC transfusion (Fig. 2).

DISCUSSION
Molecular mechanisms underlying Bombay and para-Bombay blood groups were identified several decades ago.11 Individuals with para-Bombay type may have weak A or B antigens depending on their ABO alleles.12 In this case, the patient's phenotype was determined as Ah, i.e., weak A expression revealed by adsorption-elution.
The Bombay blood group is mostly confined to South East Asian countries. Approximately 1/1,000 individuals in India have a “Bombay blood group.” In Caucasians, the incidence was found to be 1/250,000.13 The para-Bombay phenotype may be less frequent than the Bombay phenotype, particularly in Japan, where the incidence of Bombay and para-Bombay phenotypes were shown to be 1–2 in 300,000.14 In Taiwan, the incidence of the para-Bombay phenotype was estimated to be 1 in 8,000 residents based on the serological analysis.15
Bombay and para-Bombay phenotypes arise from the inheritance of two non-functional FUT1 alleles (usually designated as hh). Two entities are distinguished by the presence or absence of FUT2, known as a secretory gene. The H antigens are deficient on RBCs, but they are present in secretions from para-Bombay individuals (hh, Se/Se or Se/se).12 These can be absorbed into RBCs which then demonstrate weak A (Ah) or B (Bh) expressions.
In this case, FUT1 gene sequence analysis revealed that the patient harbored a homozygous variation, c.328G>A (p.Ala110Thr, rs56342683, FUT1*01W.02). Although this variant has been classified as a weak H allele according to the International Society of Blood Transfusion classification, a Chinese study reported that this allele was found in para-Bombay phenotype.1617 FUT2 gene sequence analysis revealed a synonymous variant Se357 that has been reported as a major secretor allele in various races.1819 From the results of these studies and the patient's phenotype, we could conclude that the patient has a para-Bombay blood type. These mutations pose huge challenges when performing transfusions on patients. Thus, laboratory staff should be aware of these variations.
Naturally occurring anti-H is of clinical relevance to individuals with Bombay and para-Bombay blood types. These patients should be transfused with only Bombay or para-Bombay blood due to the presence of preformed antibodies in their serum, which makes it impossible to find compatible blood in institutions’ blood banks. As para-Bombay blood type has been reported several times in Asia, especially in China, it is highly likely that this rare blood type is also found in Korea.919 This highlights the urgency and importance of establishing frozen blood banks for rare blood groups.
At the first instance, the patient was interpreted to have O blood group. The suspicion of a rare variant arose from the results of reverse typing. This re-emphasizes the importance of the concurrent use of forward and reverse grouping techniques for blood group determination. Rare blood groups such as Bombay and para-Bombay cannot be determined without using anti-H reagents; in the absence of anti-H antigens, such individuals are misidentified as having blood group O, and this could lead to fatal transfusion reactions. Unfortunately, some clinical laboratories in Korea are still not equipped with anti-H reagents. The use of anti-H reagents should be expanded in Korea.
Although the hemoglobin levels decreased to 5.6 g/dL, iron supplementation alone increased the hemoglobin levels to 7.9 g/dL. This exemplifies that unnecessary transfusions could be avoided with appropriate medication. This management also illustrated the possibility of managing blood inventories.
Although there have been no formal reports regarding Bombay and para-Bombay blood types in Korea, several cases have been published from Southeast Asia and China.79 As the ethnic diversity in Korea is expanding, laboratory staff and clinicians in Korea should be aware of this rare blood group and be prepared to manage patients appropriately.
 XML Download
XML Download