

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Scrub typhus is an acute febrile infectious disease caused by Orientia tsutsugamushi, which is transmitted through bites of infected chigger mites. It is endemic in Asia-Pacific region and has a high burden in Korea, affecting more than 10,000 people every year (www.cdc.go.kr/npt). Characteristic eschar and a history of outdoor activities during the epidemic season provide critical clues for the diagnosis. However, the diagnosis and treatment of scrub typhus may be complicated by other tick-borne infections which share some epidemiologic risks and clinical features at presentation. Severe fever with thrombocytopenia syndrome (SFTS) and human granulocytic anaplasmosis (HGA) are emerging tick-borne infections in Korea.123 The emergence of both infections in Korea can be traced back to 2008 and 2006, respectively.456
Although these infections are not transmitted by same vectors, a recent study in Korea reported that among 17 patients with SFTS, 7 patients were also sero-positive for scrub typhus in one area, indicating the occurrence of possible co-infection7 which was unusual. Independent exposure to both pathogens could be a possible explanation. Heo et al.8 recently reported the co-infection with scrub typhus in 3 of 17 HGA patients. However, scrub typhus in 3 patients was diagnosed with only single titer of serology in one region. As there has been epidemiologic evidence of increasing HGA in Korea, case description for the co-infection in a nationwide cohort with more objective methods would be helpful to define the phenomenon of co-infection. We explored the co-infections of SFTS or HGA in scrub typhus patients confirmed by genotyping or paired serology in a nationwide retrospective cohort from 2006.
METHODS
Study subjects
Patients with suspected clinical scrub typhus were initially recruited in 2006. Among them, patients without laboratory confirmation of scrub typhus were excluded in the study. Clinical scrub typhus was defined as a case with typical eschar or maculopapular rash, fever and therapeutic response to treatment. Laboratory diagnosis of scrub typhus was made either through a four-fold or greater antibody titer rise in paired samples or polymerase chain reaction (PCR) and genotyping for variable domains I and II of the 56-kDa antigen gene of O. tsutsugamushi. Sera from the subjects were collected from eight hospitals (Sanggye Paik Hospital, Ilsan Paik Hospital, Pusan Paik Hospital, Dongguk University Ilsan Hospital, Dankook University Hospital, Namwon Medical Center, Chonbuk National University Hospital, and Sunlin Hospital) distributed nationwide in 2006. Part of the laboratory confirmation of scrub typhus was published in a previous study.9 The serum sample of the subjects was stored at −70°C until performing PCR assay.
Laboratory diagnosis of STFS virus and Anaplasma phagocytophilum
For molecular diagnosis of SFTS virus (SFTSV), real-time reverse transcription (RT)-PCR was performed to amplify the partial L segment of SFTSV as previously described.10 Template RNA was extracted from the 140 μL serum samples of scrub typhus patients using QlAamp Viral RNA Mini kit (Qiagen Inc., Mainz, Germany) according to manufacturer's instructions. We used GoTaq® 1-Step RT-qPCR System (Promega Corporation, Madison, WI, USA) and partial L segments primer pairs for real-time RT-PCR were as follow: forward primer (5′-AGTCTAGGTCATCTGATCCGTTYAG-3′), reverse primer (5′-TGTAACTTCGCCCTTTGTCCAT-3′), probe (5′-CAATGACAGACGCCTTCCATGGTAATAGGG-3′). The cut-off threshold cycle (Ct) value for a positive sample set at 35 cycles as previously suggested.10 Viral RNA sample from confirmed SFTS patients was used as positive control.
For molecular diagnosis of A. phagocytophilum, nested PCR was performed to detect 926 bp of the 16S rRNA gene in serum as previously described.1112 Template DNA was extracted from 200 μL serum samples of scrub typhus patients using the DNeasy Blood and Tissue kit (Qiagen, Melbourne, Australia) according to manufacturer's instruction. PCR amplification was performed with the AccuPower® PCR Premix Kit (Bioneer, Daejeon, Korea). First PCR was done using a set of outer primer pairs: EE1-F (5′-TCCTGGCTCAGAACGAACGCTGGCGGC-3′), EE2-R (5′-AGTCACTGACCCAACCTTAAATG-3′). Nested PCR was performed using 2 μL of corresponding primary products as templates. Inner primer pairs for nested PCR were as follow: EE3-F (5′-GTCGAACGGATTATTCTTTATAGCTTGC-3′), EE4-R (5′-CCCTTCCGTTAAGAAGGATCTAATCTCC-3′). The genomic DNA sample from confirmed HGA patient was used as a positive control.3 Positive PCR products were sequenced by the ABI PRISM BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA), and the sequences were matched using a BLAST search (http://blast.ncbi.nlm.nih/gov/Blast.cgi). A phylogenetic tree was constructed by neighbor-joining methods in MEGA 6.0 with 1,000 bootstrap replicates.
Clinical data collection
We collected the clinical information of the subjects via electronic medical record. Clinical information included demographic variables, suspected region of exposure, season, duration of fever before the visit to hospital, presence of symptoms and signs, laboratory parameters at the initial presentation, clinical response to antibiotics and in-hospital mortality. We defined leukocytosis as white blood cell count > 10 × 103/mm3, leukopenia as white blood cell count < 4 × 103/mm3, anemia as hemoglobin < 11 g/dL, thrombocytopenia as platelet count < 150 × 103/mm3 and severe thrombocytopenia as platelet count < 50 × 103/mm3. The Acute Physiology and Chronic Health Evaluation II score were calculated within 24 hours of initial admission. Glasgow Coma Scale (GCS) were also calculated and we defined altered mentality as the GCS < 15.
Statistical analysis
The lower and upper limits of the 95% confidence interval (CI) for the prevalence of co-infection were calculated by the Wilson procedure with a correction for continuity.13
Ethics statement
This study was approved by the Institutional Review Board (IRB) at Boramae Medical Center (IRB No. 30-2018-57). All personal identifiers were anonymized for confidentiality before data processing was performed. All clinical research was in compliance with the principles expressed in the Helsinki Declaration.
RESULTS
Subjects
A total of 167 scrub typhus patients were included in the analysis. Laboratory confirmation of scrub typhus was done by PCR in 146 patients and by serologic assay in 21 patients. The clinical and demographical characteristics of patients were shown in Table 1. The median time from the first onset of fever to sample collection was 6 days (range, 0–36). All patients were diagnosed in autumn season (September to December) and improved after appropriate antibiotic treatment (no mortality). Most patients (82.0%) were from western Korea.
Table 1
Characteristics of the study subjects

Data are presented as mean (range) or number (%).
ALT = alanine transaminase, AST = aspartate transaminase, APACHE II = Acute Physiology and Chronic Health Evaluation II, COPD = chronic obstructive pulmonary disease, CVA = cerebrovascular accident, LDH = lactate dehydrogenase, HGA = human granulocytic anaplasmosis.
![]()
Co-infections of scrub typhus and HGA
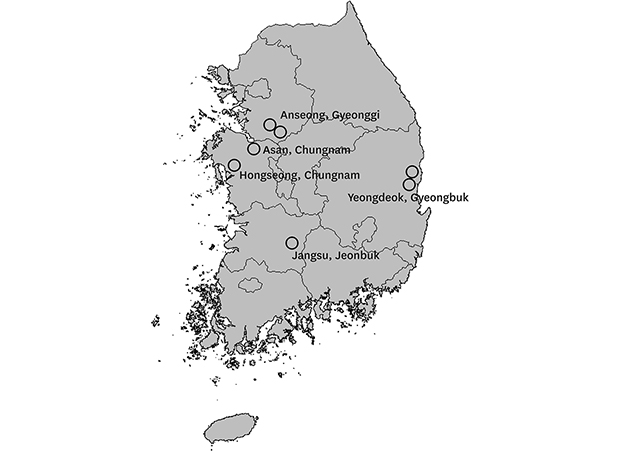
Seven patients with confirmed scrub typhus (7/167, 4.2%) showed positive results for A. phagocytophilum. The BLAST search showed high identity for A. phagocytophilum sequences, with a similarity ranging from 98.2% to 99.8% (deposited in GenBank; accession numbers MK271302–MK271308). The suspected regions of HGA infection were scattered nationwide (Fig. 1). The prevalence of co-infection was in the order of Gyeonggi province (2 of 9, 22.2%), Gyeongbuk province (2 of 14, 14.3%), Chungnam province (2 of 50, 4.0%) and Jeonbuk province (1 of 70, 1.4%). Most of these regions consisted of farm field. However, direct statistical comparison was limited due to the heterogeneity of sample sizes in each region. Phylogenetic tree analysis showed that the seven strains found in this study were closely clustered and constituted a clustered group with other human strains isolated in Korea and the United States (Fig. 2).
 | Fig. 1Geographic location of co-infection with scrub typhus and human granulocytic anaplasmosis. Epidemiologically suspected regions of infection are shown. Cases are concentrated in a northwestern farm field area and the other cases are also scattered in southern and eastern areas, raising the possibility of nationwide occurrence. One empty circle indicates one patient with co-infection and the location is specified.
|
 | Fig. 2Phylogenetic tree of A. phagocytophilum causing the co-infection. The phylogenetic tree was constructed using neighbor-joining methods based on the 16S rRNA gene sequences of A. phagocytophilum in reference to other strains from previous studies. The sequences from our study are closely clustered with other human strains in Korea and the United States. Our sequences are marked with arrows. The scale bar represents the evolutionary distance.KWD = Korean water deer.
aA first human isolate in Korea reported in 2014.
|
Among the 7 patients, 4 patients were men, and median age was 70 years (range, 38–76) (Tables 1 and 2). The co-infected patients had not different clinical manifestations compared to the patients with scrub typhus only. The longest time from first fever onset to serum collection was 12 days. Patients with HGA co-infection all presented with fever and maculopapular rash. Typical eschar was observed in 6 of 7 patients. Leukopenia (1/7) and thrombocytopenia (2/7) were not prominent. Scrub typhus was confirmed by PCR in 5 patients and by serology in 2 patients. Three patients were treated with azithromycin without failure. The prevalence of co-infection with HGA was estimated to be 4.2% (95% CI, 2.1–8.4). All patients in this study showed negative results for co-infection with SFTSV. The possible prevalence of co-infection was estimated to be 0% (95% CI, 0–2.3).
Table 2
Details of 7 patients with co-infection of scrub typhus with human granulocytic anaplasmosis

ALT = alanine transaminase, AST = aspartate transaminase, AZT = azithromycin, COPD = chronic obstructive lung disease, CRP = C-reactive protein, DC = doxycycline, Ig = immunoglobulin, NA = not available, PCR = polymerase chain reaction, WBC = white blood cell; W = woman, M = man.
aThe serologic assay of paired sample was performed b22 days and c15 days after the initial assay.
![]()
DISCUSSION
A previous study published in 2002 suggested that co-infection might exist because six seropositive samples for A. phagocytophilum were also seropositive for O. tsutsugamushi.14 However, because of the possibility of cross-reactivity of serological test, this study could not confirm the co-infection. Co-infection of mites and tick-borne pathogens may occur through multiple exposures to different vectors carrying each pathogen or through an exposure to one vector carrying multiple pathogens. Co-infection of HGA and other tick-borne diseases mediated by one vector has been well documented.15 For example, A. phagocytophilum shares the same vector with Borrelia burgdorferi and co-infections of both pathogens have been identified where HGA and Lyme disease is endemic.161718 However, chigger mites are not known to transmit HGA. Multiple exposures to different vectors in a short time interval may be a more plausible explanation at this time. Ixodes species which mainly transmit HGA is distributed in nationwide of Korea.19 Chigger mites which transmit the causative agent of scrub typhus are distributed nationwide and more densely distributed in western and southwestern Korea.20 Although these diseases do not share same vectors, the co-infection may be possible in areas where the density of chiggers mites and ticks are simultaneously high. The enzootic cycle including Ixodes ticks and rodents plays a critical role to maintain A. phagocytophilum.21 The mites, as main vectors for O. tsutsugamushi, reside in relatively humid and grassland environment, consistent with where the rodents live.22 This enzootic commonality supports the possibility of a co-infection.
Although the incidence was not high, our study showed that HGA was not uncommon and suggested that HGA may be prevalent. In febrile patients with outdoor activities, 7.9% (47/594 cases) had serological evidence of HGA in a recent study in Korea.23 Compared to scrub typhus, HGA might have been missed or neglected during clinical practice in Korea. HGA is often not considered to be a differential diagnosis, and the diagnostic assay for HGA has not been routinely available in most Korean hospitals.
It is known that many cases of HGA are asymptomatic to mild illness.24 Doxycycline is a primary drug used to treat for infection of O. tsutsugamushi and A. phagocytophilum, and the response to this treatment is favorable. Azithromycin has not been known to have a therapeutic effect on A. phagocytophilum,25 in contrast to O. tsutsugamushi.26 Considering that the clinical outcome of all patients was good even though 3 patients received an azithromycin treatment, it seems that the co-infection did not increase the clinical severity of our subjects. However, caution may be needed when azithromycin is prescribed as an initial treatment for scrub typhus in an endemic area of HGA, especially in immunocompromised patients whose A. phagocytophilum infection may be more severe and even fatal.24 Most patients in this study showed normal leukocyte and platelet counts, although most HGA patients are known to have transient leukopenia or thrombocytopenia. Generally, transient laboratory abnormality of HGA patients may return to normal after one week of onset.24 Significant leukopenia and thrombocytopenia may not have been observed because the sample was taken a considerable time after the onset of fever. Another possible explanation is that the clinical manifestation of HGA was so mild that that of scrub typhus was dominating.
The potential for carryover contamination of the nested PCR reactions is a major concern due to the use of PCR-amplified products as template. To avoid such contamination, we performed the different parts of manipulations in distinct areas not sharing reagents and equipment. Amplicons from our nested PCR assays showed some distances from each other and positive control (gene accession No. KF805344) (Fig. 2).
We did not observe any scrub typhus and SFTS co-infections, in contrast to a previous study.7 As our study samples were collected in 2006, and it is uncertain whether there was a sufficient concurrent epidemic of SFTS in Korea, in contrast to the presence of HGA at least since 2006.6 Another possible explanation is that there is a possibility of false negatives in few cases because laboratory detection of another gene of SFTSV, such as S segment or M segment, was not performed.
This study has a few limitations. First, as this study investigated only past samples, contemporary prospective study is needed to check the continuity of the co-infections. Second, we could not check the change of antibody titer for HGA and SFTSV because we could not obtain paired samples from the patients. As we only used a PCR method for both agents, we might miss patients in non-bacteremic/viremic phase resulting in underestimation of the prevalence.
In summary, we confirmed the co-infections of HGA and scrub typhus in Korea although the frequency was low. This finding suggests that HGA may be more prevalent than expected and more active diagnostic approach is needed in febrile patients in Korea.
 XML Download
XML Download