

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Acinetobacter baumannii is a non-fermenting gram-negative bacteria with ability to acquire resistance easily to various antibiotics. In Korea, the carbapenem-resistance rate of A. baumannii is very high1 and carbapenem-resistant A. baumannii (CRAB) infections cause high-mortality in hospitalized patients.2 At the present time, colistin has been used as the treatment of choice for CRAB infections.
One of the strategies to reduce the mortality in patients with CRAB infections is to use colistin early because many patients infected with carbapenem-resistant organisms did not previously receive appropriate empirical antibiotics.34 However, because of the suboptimal concentration of colistin maintained by normal kidney function5 and the variable hydrolysis of colistimethate sodium,6 there is concern that colistin may not be an effective antibiotic. In addition, the high rate of acute kidney injury (AKI) during colistin use7 and concern for the development of colistin resistance8 causes hesitation in the empirical use of colistin. Some studies have investigated whether early colistin use affected the mortality from infections caused by carbapenem-resistant organisms but the results were not consistent.49
Therefore, we investigated the association of early colistin therapy with 28-day mortality in patients with CRAB bacteremia.
METHODS
Study population and design
This retrospective multicenter study was conducted at five hospitals with 700 to 900 beds in the Korea. All patients aged ≥ 18 years with a CRAB-positive blood culture were identified by review of the daily computerized reports of blood cultures between January 2012 and March 2015. A. baumannii identification was performed using standard methods. Susceptibility testing was done using the microdilution method (MicroScan system; Baxter Health Care, West Sacramento, CA, USA) and the results were interpreted according to the National Committee for Clinical Laboratory Standards guidelines published in 2011.10 A. baumannii isolates with a minimal inhibitory concentration of ≥ 16 μg/mL to imipenem were considered to be CRAB. As shown in Fig. 1, the patients who were transferred to other hospitals within 28 days from the time of the blood culture and patients who received antibiotics other than colistin were excluded from the study. Initially, to identify the risk factors associated with 28-day mortality in all enrolled patients with CRAB bacteremia, the clinical variables of the surviving patients were compared to those of the deceased patients. To reduce selection bias, subgroup analysis was done using a propensity score-matching method.

Definitions and data collection
The patients' demographic data was collected. Malignancy, neurologic diseases, chronic lung diseases, diabetes mellitus, liver cirrhosis classified as Child B or C, heart failure, and chronic renal diseases were searched as comorbidities. Any one of following conditions was defined as immunocompromised: 1) a human immunodeficiency viral infection or acquired immune deficiency syndrome, 2) a solid organ or hematopoietic stem cell transplant recipient, 3) chemotherapy within six weeks, 4) systemic steroids therapy equivalent to or higher than 20 mg of prednisone for two weeks, 5) receiving immunosuppressive agents within two weeks before hospitalization. The McCabe and Jackson Classification was used as index of the severity of the comorbidities.11 The source of the infection was determined according to the guidelines issued by the Centers for Disease Control and Prevention.12 Patients having two or more of compatible clinical signs, symptoms, and one or more of radiologic findings were defined as having pneumonia. Other diagnosis such as catheter-associated infection and intraabdominal infection took precedence over the diagnosis of pneumonia. Mechanical ventilation, vasopressor use, intensive care unit (ICU) admission and the Sequential Organ Failure Assessment (SOFA) scores13 were chosen as the indices of severity. AKI was identified if one of the following criteria was satisfied: 1) An increase in serum creatinine of two times over baseline, 2) a decrease in the glomerular filtration rate of more than 50%, and 3) urine output of < 0.5 mL/kg/hr for > 12 hours.7 Data on previous surgeries within one month were also collected. Previous CRAB colonization was defined as the isolation of CRAB from any clinical specimens within 30 days of the CRAB blood culture. Antibiotics use, such as with broad-spectrum cephalosporins, anti-pseudomonal penicillin/beta-lactamase inhibitors, fluoroquinolones and carbapenems at the time of blood culture were noted. A previous study of patients with CRAB bacteremia who did not receive any appropriate antibiotics reported that many died within five days.2 Consequently, the early colistin therapy was defined as intravenous colistin administration for > 48 hours within five days after the blood culture collection. Late colistin therapy was defined as intravenous colistin administration for > 48 hours after five days from the time of blood culture collection. The colistin used in this study was colistimethate sodium, supplied as 400 mg (150 mg of colistin base activity) per vial. The primary outcome was 28-day mortality and the secondary outcome was 14-day mortality following the blood culture collection.
Statistical analyses
SPSS for Windows (version 25.0; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The Mann-Whitney U test or the student's t-test were used for comparison of the continuous variables. Pearson's χ2 test or Fisher's exact test were statistical methods for comparison of the categorical variables. Binary logistic regression was used to identify the variables significantly associated with 28-day mortality in patients with CRAB bacteremia. The variables with statistical significance at the 5% level in the univariate analysis were chosen for the multivariate analysis. SOFA scores ≥ 8 were chosen as a binary variable according to calculations from the receiver operating curve. Kaplan-Meier survival curves were drawn to compare the survival between patients with and without early colistin therapy. The 1:1 pair-matched case-control cohort was prepared using a propensity-score matching method to adjust for all variables except AKI, because colistin-induced AKI should not be adjusted. All significance testing was 2-tailed and P < 0.05 was considered statistically significant.
RESULTS
A total of 332 patients with CRAB bacteremia were identified. The blood culture results were received a median of four days (interquartile range [IQR], 3–4 days) after the blood collection. After excluding 15 patients who transferred out of the hospital and 14 patients who received antibiotics other than colistin, 303 patients were included in the analyses. Of them, 76 (25.1%) patients received early colistin therapy, 35 (46.1%, 35/76) as monotherapy and 41 (53.9%, 41/76) as combination therapy. The median starting day for colistin therapy was 3 days (IQR, 2–5 days) after blood culture collection. The median duration for colistin therapy was 9 days (IQR, 4–15 days). In 76 patients receiving early colistin therapy, carbapenem (71.4%, 30/76) was the most frequently used as combination therapy, following by ampicillin/sulbactam (11.8%, 9/76), rifampin (9.2%, 7/76), piperacillin/tazobactam (3.9%, 3/76), and aminoglycoside (2.6%, 2/76). In 227 patients without appropriate empirical therapy, empirical antibiotics were chosen as follows: carbapenems (55.9%, 127/227), piperacillin/tazobactam (21.1%, 48/127), fluoroquinolones (13.7%, 31/227), broad-spectrum cephalosporins (11.9%, 27/227), aminoglycoside (2.2%, 5/227), and ampicillin/sulbactam (0.8%, 2/227). In patients without appropriate early antibiotics, 57.3% (130/227) died within 5 days after blood culture collection and 8.4% (19/227) patients received late colistin therapy (Fig. 1).
As shown in Table 1, before propensity score-matching, the vasopressor use (early colistin therapy, 28.9% [22/76] vs. inappropriate early antibiotics, 44.5% [101/227], 44.2%; P = 0.02) was higher in patients receiving early colistin therapy, as indicated by the initial severity index. AKI (early colistin therapy, 45.1% [32/76] vs. inappropriate early antibiotics, 31.0% [65/227]; P = 0.04) developed more frequently after CRAB bacteremia in patients receiving early colistin therapy.
Table 1
Comparison of the clinical characteristics between CRAB bacteremic patients who received and did not receive early colistin therapy

Data are numbers (%) of patients.
CRAB = carbapenem-resistant Acinetobacter baumannnii, IQR = interquartile range, ESRD = end stage renal disease; ICU = intensive care unit, SOFA = Sequential Organ Failure Assessment, AKI = acute kidney injury.
![]()
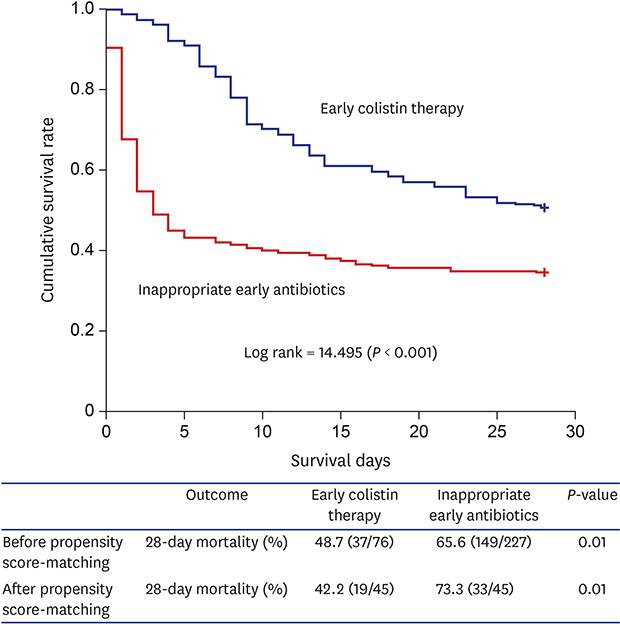
The five-day, 14-day mortality, and 28-day mortalities were 45.5%, 56.8%, and 61.4%, respectively. The 28-day mortality was not different between patients receiving late colistin therapy and those not receiving any appropriate antibiotics (late colistin therapy, 15.8% [3/19] vs. never appropriate antibiotics, 21.8% [17/78]; P = 0.75) (Fig. 1). In patients receiving colistin therapy, the 28-day mortality was lower in patients receiving late colistin therapy, compared to patients receiving early therapy (early colistin therapy, 50.0% [38/76] vs. late colistin therapy, 15.8% [3/19]; P = 0.01). The 28-day mortality was lower in patients who received early colistin therapy compared to patients who did not receive appropriate early antibiotics (early colistin therapy, 48.7% [37/76] vs. inappropriate early antibiotics, 65.6% [149/227]; P = 0.01). Notably, the survival curves within the five days after blood culture collection were dramatically different between both groups (Fig. 2).
 | Fig. 2Kaplan-Meier survival curve of patients with carbapenem-resistant Acinetobacter baumannii bacteremia who received early colistin therapy and inappropriate early antibiotics.
|
The comparison of the clinical characteristics between CRAB bacteremic patients with and without 28-day mortalities and prognostic factors associated with the 28-day mortality are shown in Table 2. The variables of fatal or rapidly-fatal McCabe classification, an immunocompromised state, ICU admission, SOFA scores ≥ 8, mechanical ventilation use, vasopressor use, the previous use of carbapenems, pneumonia and catheter-related infections as the source of the bacteremia, removal of the bacteremia source, AKI, and early colistin therapy were included in the multivariate analyses. Finally, fatal or rapidly-fatal McCabe classification as an underlying condition (adjusted odds ratio [aOR], 3.57; 95% confidence interval [CI], 1.78–7.13), ICU admission (aOR, 3.28; 95% CI, 1.48–7.23), SOFA scores ≥ 8 (aOR, 4.37; 95% CI, 2.10–9.09) and vasopressor use (aOR, 4.08; 95% CI, 1.82–9.15) as indices of severity, and AKI (aOR, 2.42; 95% CI, 1.18–4.94) were statistically independent poor prognostic factors. Early colistin therapy (aOR, 0.83; 95% CI, 0.21–0.94) and catheter-related infection as the source of the bacteremia (aOR, 0.21; 95% CI, 0.07–0.65) were independent favorable prognostic factors associated with 28-day mortality in patients with CRAB bacteremia.
Table 2
Prognostic factors associated with the 28-day mortality in patients with CRAB bacteremia

Data are numbers (%) of patients.
CRAB = carbapenem-resistant Acinetobacter baumannnii, OR = odds ratio, CI = confidence interval, aOR = adjusted odds ratio, ICU = intensive care unit, SOFA = Sequential Organ Failure Assessment, AKI = acute kidney injury.
![]()
After 1:1 paired propensity score-matching, 45 patients receiving early colistin therapy and 45 patients without appropriate early antibiotics were analyzed. As shown in Table 3, early colistin therapy was still significantly associated with lower 28-day mortality in the propensity score-matching analysis (aOR, 0.31; 95% CI, 0.11–0.88).
Table 3
Prognostic factors associated with the 28-day mortality in patients with CRAB bacteremia in a propensity score-matched analysis

Data are numbers (%) of patients.
CRAB = carbapenem-resistant Acineotobacter baumannii, OR = odds ratio, CI = confidence interval, aOR = adjusted odds ratio, ICU = intensive care unit, SOFA = Sequential Organ Failure Assessment, AKI = acute kidney injury.
![]()
The prognostic factors associated with 14-day mortality were also analyzed (Supplementary Table 1). Fatal or rapidly-fatal McCabe classification as an underlying condition (aOR, 3.41; 95% CI, 1.75–6.65), SOFA scores ≥ 8 (aOR, 4.88; 95% CI, 2.41–9.87) and vasopressor use (aOR, 3.94; 95% CI, 1.83–8.47) as indices of severity, pneumonia as the source of the bacteremia (aOR, 2.05; 95% CI, 1.05–4.02), and AKI (aOR, 2.31; 95% CI, 1.15–4.63) were statistically independent poor prognostic factors. Early colistin therapy (aOR, 0.32; 95% CI, 0.15–0.69) was also an independent favorable prognostic factor associated with 14-day mortality, as it was associated with 28-day mortality in patients with CRAB bacteremia.
DISCUSSION
This study reports that patients with CRAB bacteremia who received early colistin therapy died less often than patients who did not receive appropriate early antibiotics. This study supports the opinion that early colistin therapy may be a strategy to reduce the mortality of CRAB bacteremia. The result is expected to be used to establish treatment strategies for sepsis in facilities with a high prevalence of CRAB infections.
Some studies on the association of appropriate empirical antibiotics with mortality in patients with carbapenem-resistant organism infections have been conducted. In a retrospective study including 54 patients with CRAB bacteremia, appropriate empirical therapy, mostly intravenous colistin (92.6%), lowered intensive care unit mortality (aOR, 0.15; 95% CI, 0.03–0.96).4 In a recent prospective study including 406 patients with carbapenem-resistant gram-negative bacterial infections, mostly with CRAB (77%), the 14 day-mortality was not different between the group that received appropriate empirical therapy, mostly intravenous colistin (94%), and the group that received inadequate empirical therapy (OR, 1.42; 95% CI, 0.91–2.22).9 These previous inconsistent results might derive from the heterogeneity of the study population and design. Our study included specific patients, only those with CRAB bacteremia who were treated with intravenous colistin. This study design helped to draw more specific conclusions.
Our study showed that AKI was independently associated with the 28-day mortality in CRAB bacteremia. Whether colistin-associated nephrotoxicity increases mortality in carbapenem-resistant organism infections is controversial. In previous studies on colistin-associated nephrotoxicity, AKI was reported to be a poor prognostic factor.1415 However, some studies have reported that AKI was not associated with mortality in CRAB infections.71617 In our study, AKI, a poor prognostic factor, frequently developed in the patients receiving early colistin therapy, although this association failed to be proven in propensity score-matching analysis. Despite this negative effect of AKI during colistin use, the 28-day mortality was lower in patients who received early colistin therapy.
This study had several limitations. First, owing to the nature of the retrospective study, empirical antibiotics other than colistin and definite therapy were not well-controlled. In order to accurately determine whether the time of administration of colistin affects mortality, only patients who finally received definite colistin should be analyzed. Only well-designed prospective studies in which all patients received identical empirical antibiotics except colistin and finally were treated by colistin will overcome this survival bias. Second, some significant prognostic variables may have been omitted from the analyses. Third, CRAB bacteremia might not have been a cause of death in some patients. Alternative causes of death, such as terminal cancer or impediments to care, such as refusal of intensive care treatment were not considered. Fourth, catheter-related infection as source of infection may be underestimated, because some patients died before central venous catheter tip culture. Last, this is a study of A. baumannii complex rather than A. baumannii, although about 90% of A. baumannii complex bacteria with multi-drug or carbapenem resistance belonged to the genomic species A. baumannii. The variable of species could affect mortality,18 but isolates were not collected and identification of the genomic species was not possible.
In conclusion, our data suggest that early colistin therapy may reduce the mortality of patients with CRAB bacteremia. However, owing to the toxicity of intravenous colistin, it is not clear who will benefit from the strategy of empirical colistin therapy.
 XML Download
XML Download