

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cutaneous nerve biopsies have come to be considered one of the few reliable tools for evaluating peripheral neuropathies, including small-fiber neuropathy (SFN).1234 These conventional methods are confined to two-dimensional analyses, based on the XY plane of thin tissue sections of skin,125 which may fail to accurately quantify three-dimensionally arborized nerve fibers. Thus, alternative methods that take into account the entire, unsectioned nerve morphology would allow more-accurate quantifications and diagnoses of the relevant pathologies.
The recently reported tissue-clearing and labeling technique called active clarity technique-pressure related efficient and stable transfer of macromolecules into organs (ACT-PRESTO) can clear biological tissues as a whole without damaging the original architecture, and can also accelerate antibody penetration into thick specimens by applying pressure.67 These characteristics mean that the method could reduce the processing time relative to other tissue-clearing protocols7 and three-dimensional image reconstruction techniques,89 which is advantageous for clinical implementations as a diagnostic tool.
In the present study we sought to establish the usefulness of ACT-PRESTO in the three-dimensional quantification of intraepidermal nerve fibers density (IENFD) and in diagnosing peripheral neuropathies.
Go to : 
METHODS
The present data were obtained from a prospective clinical study evaluating the diagnostic value of the ACT-PRESTO skin-clearing and labeling technique for assessing peripheral neuropathies. The institutional review board of Korea University Medical Center (KUMC), Anam Hospital approved the clinical trial (approval no. 2016AN2056).
Participants
Healthy participants and neuropathy patients who were expected to show a reduced IENFD including SFN or postherpetic neuralgia (PHN) were recruited for this study. SFN was defined according to its indicative clinical symptoms, including distal dominant paresthesia despite normal results in a neurological examination, nerve conduction study (NCS), and electromyography (EMG). PHN was determined according to a medical history of herpes zoster infection and subsequent paresthesia appearing in the compromised area. All participants were fully informed about the possible risks before the study. A neurologist and dermatologists working at KUMC performed the clinical and/or neurological examinations, as well as the NCS and EMG.
Cutaneous nerve biopsies
Cutaneous nerve biopsies were performed with a commonly used 3-mm punch device under local anesthesia with lidocaine, as reported previously.1011 Two separate skin samples were collected from the distal leg of healthy participants and patients with SFN. For patients with PHN, cutaneous biopsy samples were obtained in the area where the neuropathy symptoms were most prominent. One pair of the biopsied tissues was cryosectioned and immunostained for protein gene product 9.5 (PGP 9.5; CEDARLANE, Burlington, NC, USA) and/or collagen type IV antibodies using two conventional methods: bright-field immunohistochemistry (IHC) and indirect immunofluorescence (IF). The other pair of biopsied tissues was processed using ACT-PRESTO followed by PGP 9.5 immunolabeling.
Conventional two-dimensional assessments
Biopsy specimens were fixed in Zamboni's solution (2% paraformaldehyde and picric acid) for two-dimensional assessments. The fixed samples were cryosectioned at thicknesses of 50 and 80 µm for IHC and IF, respectively. The first few and last few sections were discarded owing to potential artifacts.12 Three randomly selected sections of each thickness were used for subsequent immunostaining. The 50-µm-thick sections were immunolabeled with PGP 9.5 (1:2,000) using 3,3′-diaminobenzidine staining for IHC. The immunolabeled sections were imaged using bright-field microscopy (BX51, Olympus, Tokyo, Japan). The 80-µm-thick sections were immunostained with PGP 9.5 (1:800) and type IV collagen (1:800; Sigma-Aldrich, St. Louis, MO, USA) using indirect IF. We used confocal microscopy (LSM 700, Carl Zeiss, Jena, Germany) for image acquisition, and serial optical sections taken at 1-µm intervals were reconstructed using the related software (ZEN, Carl Zeiss). The maximum projection image derived from the stacked results was used to quantify cutaneous nerve fibers. The guidelines of the European Federation of Neurological Societies (EFNS) were adopted for quantification of the IENFD and the unit of results were represented as ‘IENFs/mm’.12
Three-dimensional evaluations using ACT-PRESTO
The remaining biopsied skin samples were processed according to the cutaneous ACT-PRESTO protocol (Fig. 1), which was registered as a patent in South Korea in August 2018 (patent number: 10-1888782). The epidermis was separated from the dermis using the salt split skin test12 and was fixed in Zamboni's solution. The ACT tissue-clearing method essentially comprised three stages: hydrogel monomer embedding, polymerization, and electrophoretic tissue clearing (ETC). More specifically, the epidermis was immersed in a 4% acylamide solution mixed with the thermal initiator 2,2′-azobis [2-(2-imidazolin-2-yl) propane] dihydrochloride (Wako Pure Chemical, Osaka, Japan) overnight at 4℃. The hydrogel monomer infused into the tissue was polymerized at −70 kPa and 37℃ in a vacuum chamber. The polymerized sample was then transported to an ETC chamber filled with 4% sodium dodecyl sulfate in a solution of 200 mM boric acid in H2O (pH 8.5). ETC proceeded for 4 h under static conditions, including 1.5 A and 37℃; precise conditions are required for ETC to ensure effective tissue-clearing and prevent significant morphological changes that could interfere with IENFD quantification (Fig. 2). The cleared epidermis was immunolabeled with PGP 9.5 (1:400) aided by centrifugal force; this process is thus called c-PRESTO (Fig. 3). The cleared skin was immersed in a solution with PGP 9.5 or Cy3 (1:500; Jackson Immuno Research, West Grove, PA, USA) and centrifuged at 800×g for 3 and 2 h to accelerate the penetration of primary and secondary antibodies, respectively. The immunostained tissue was subsequently immersed in a reflective-index matching solution (RIMS) to increase the transparency.
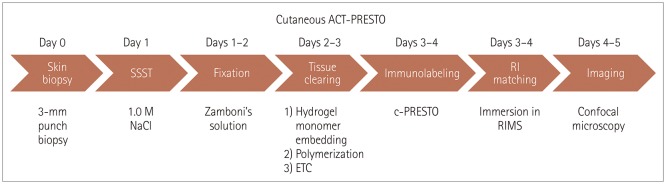 | Fig. 1Summary of the processing steps of the cutaneous ACT-PRESTO protocol, from separating the epidermis from biopsied skin samples to imaging with confocal microscopy. ACT-PRESTO: active clarity technique-pressure related efficient and stable transfer of macromolecules into organs, c-PRESTO: centrifugal-PRESTO, ETC: electrophoretic tissue clearing, RI: reflective index, RIMS: reflective-index matching solution, SSST: salt split skin test.
|
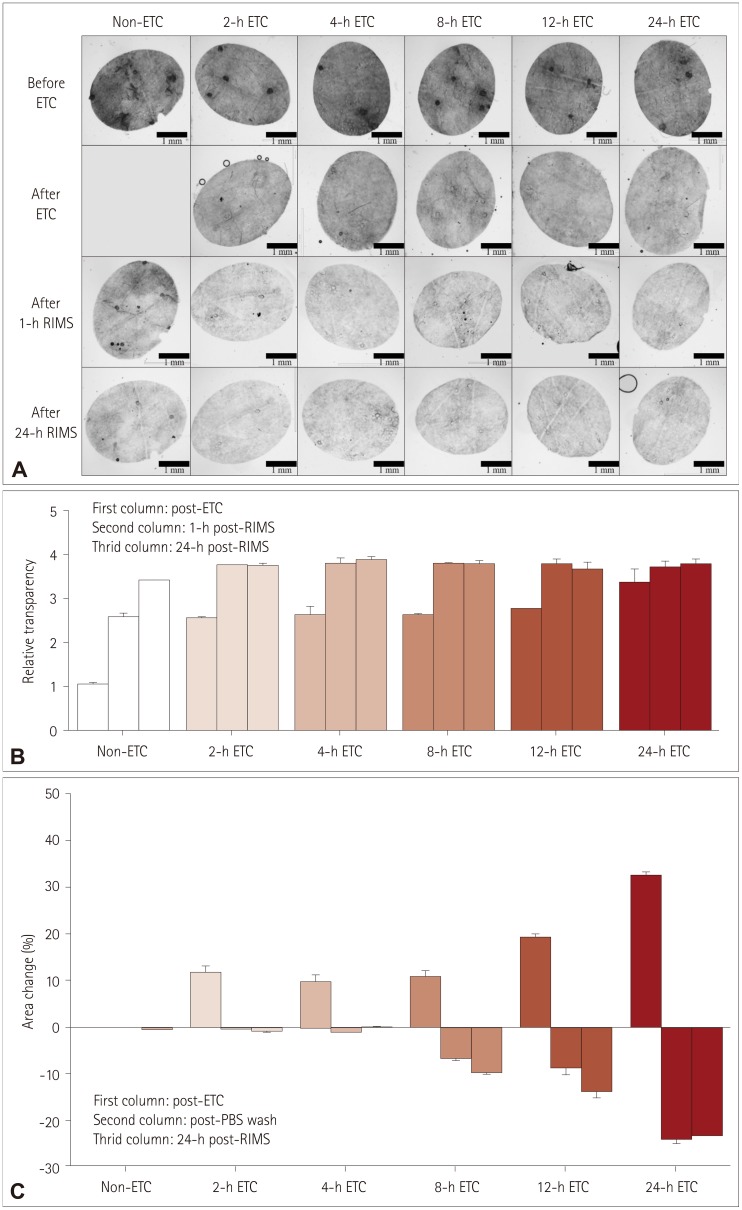 | Fig. 2Serial changes in transparency and area during the cutaneous ACT-PRESTO process, focusing on ETC and immersion in RIMS. A: Morphological changes in transparency according to the duration of ETC. B: Quantitative alterations of the relative transparency according to the duration of ETC. The improvement in relative transparency was proportional to the duration of ETC, but the differences were standardized after immersion in RIMS. C: Extent of area change related to the duration of ETC. The skin specimens consistently expanded after ETC in proportion to the duration of ETC. The enlarged tissues returned to their original size after washing with PBS. However, ETC durations exceeding 4 h resulted in irreversible shrinkage of the original tissues to an extent proportional to the ETC duration. ACT-PRESTO: active clarity technique-pressure related efficient and stable transfer of macromolecules into organs, ETC: electrophoretic tissue clearing, PBS: phosphate-buffered saline, RIMS: reflective-index matching solution.
|
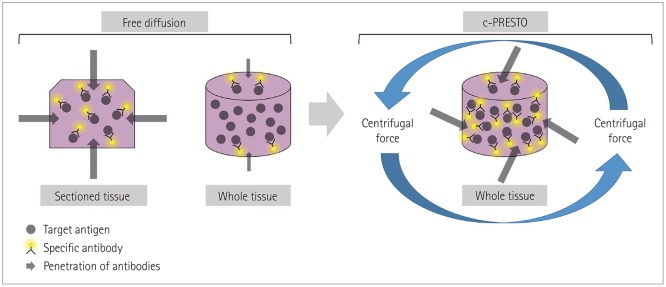 | Fig. 3Schematic diagram of immunohistochemistry for whole-tissue processing after tissue-clearing. The effectiveness of combinations of target antigens and specific antibodies was substantially impeded by the thicker whole tissue compared with conventional sectioned tissue. Tissues for c-PRESTO were centrifuged to obtain sufficient penetration depths of the primary and secondary antibodies, and so the technique could increase the probability of binding between target antigens and specific antibodies. c-PRESTO: centrifugal-pressure related efficient and stable transfer of macromolecules into organs.
|
The immunostained cutaneous nerve fibers were imaged by confocal microscopy (LSM 700) with z-stacking at intervals of 1 µm. Twenty images with an overall area of 0.58 mm2 in the XY plane were consecutively imaged and merged by a tile scan, and the reconstructed three-dimensional cutaneous nerve fibers were quantified and unit of the results were represented as ‘IENF/mm’. All of the PGP 9.5-stained nerve fibers were manually counted, and the nerve fibers that clearly arose from the basement of the epidermis were regarded as significant data. The basal side of the epidermis could be readily verified by its more-compact cellular composition compared with the upper side in the nuclear staining.
Statistical analysis
Statistical differences between the results obtained from conventional two-dimensional assessments and the three-dimensional evaluations were analyzed using Wilcoxon's signed-rank test. All analyses were performed with IBM SPSS software (version 20.0 for Windows, IBM Corp., Armonk, NY, USA).
Go to :
RESULTS
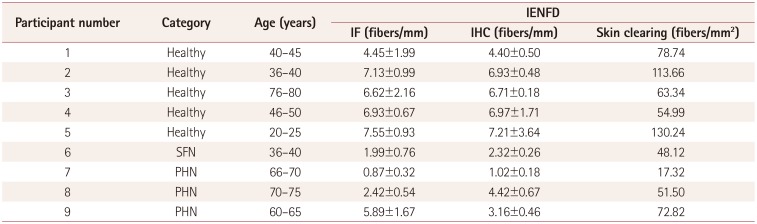
Nine subjects comprising five healthy individuals and four patients with peripheral neuropathies voluntarily participated in the study (Table 1). The sex ratio was 1:0.8, and they were aged 52.56±18.93 years (mean±SD). The patient group comprised one patient with SFN and three with PHN. The compromised regions of patients with PHN were confined to the trunk (T4 or T6 dermatome).
The ETC process transformed each opaque skin specimen into an optically translucent sample, and adjustment of the reflective index with RIMS additionally increased the transparency (Fig. 2A, B) without substantially changing any areal dimensions from the original state (Fig. 2C). This process also made the skin specimen more penetrable by macromolecules, such as antibodies, through effective lipid removal, without deterioration of the original architecture. Within a few days the ACT-PRESTO process yielded distinctive three-dimensional images of IENFs (Figs. 4E, F, and 5) that differed from conventional two-dimensional images (Figs. 1 and 4A–D) and also provided reliable quantitative data on the IENFD (Table 1).
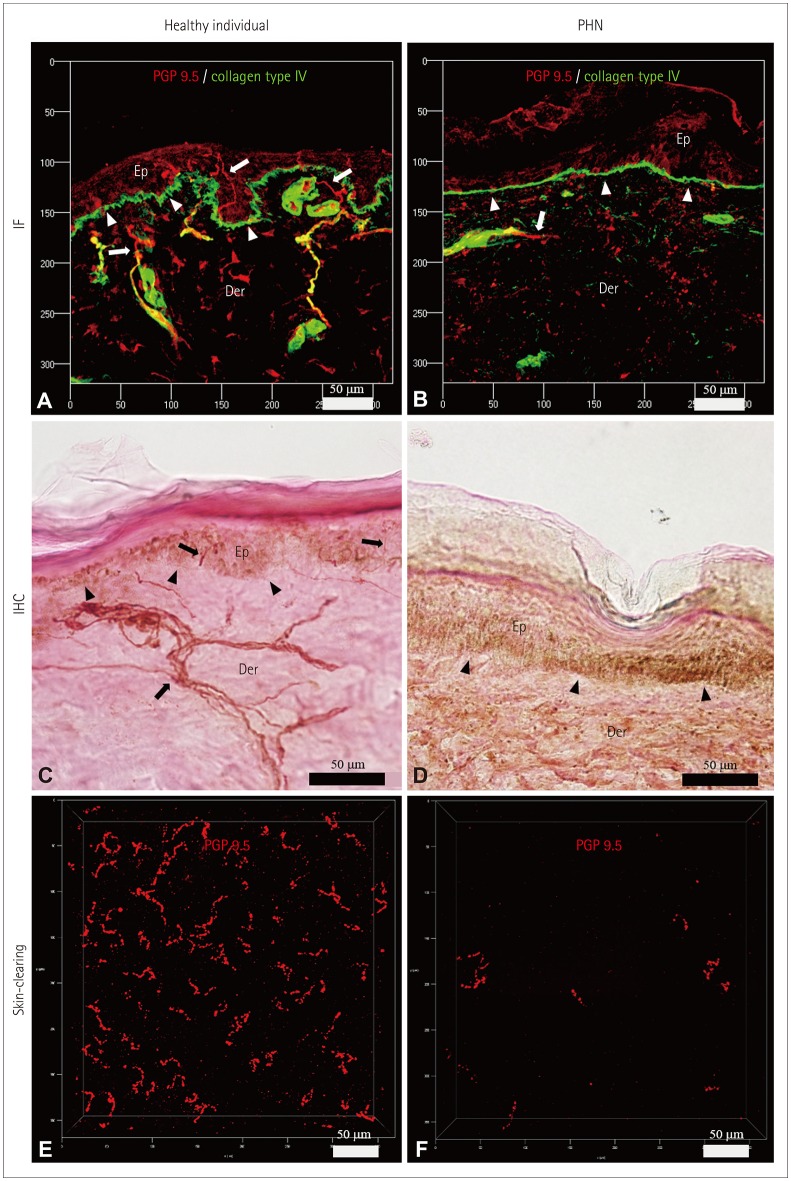 | Fig. 4Characteristics of the IENFs of a healthy participant (A, C, and E) and a PHN patient (B, D, and F). IENFs were quantified using the conventional methods of indirect IF (A and B) and IHC (C and D), as well as the ACT-PRESTO tissue-clearing technique (E and F). Cross-sectional views (A–D) and bird's-eye views (E and F) of IENFs. IF images (A and B) were obtained using confocal microscopy with a Plan-Apochromat 20×/0.8 M27 lens (maximum projection; stack size, 80 µm; stack step, 1 µm). IHC images (C and D) were produced using bright-field microscopy with a UPlanApo 40×/0.85 lens. Cutaneous nerve fibers (arrows) and the basal layer of the epidermis (arrowheads) (A–D). Images associated with skin-clearing (E and F) were also obtained using confocal microscopy with a Plan-Apochromat 20×/0.8 M27 lens (stack size, 200 µm; stack step, 1 µm). ACT-PRESTO: active clarity technique-pressure related efficient and stable transfer of macromolecules into organs, Der: dermis, Ep: epidermis, IENFs: intraepidermal nerve fibers, IF: immunofluorescence, IHC: immunohistochemistry, PGP 9.5: protein gene product 9.5, PHN: postherpetic neuralgia.
|
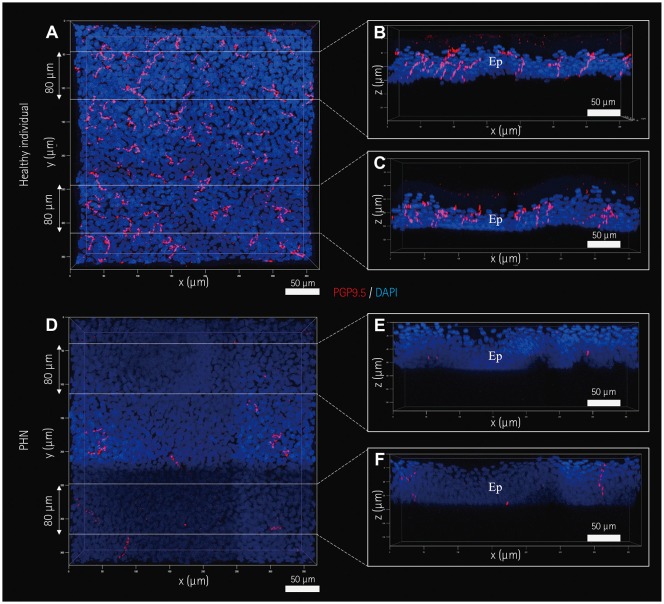 | Fig. 5Images of IENFs produced by the skin-clearing technique. IENFs of a healthy subject (A–C) and a PHN patient (D–F). Selected areas of three-dimensional images (A and D) in Fig. 4E and F, respectively, were optically sectioned at a thickness of 80 µm (B–F). All images were obtained and processed using confocal microscopy with a UPlanApo 40×/0.85 lens and the related software. Ep: epidermis, IENFs: intraepidermal nerve fibers, PGP 9.5: protein gene product 9.5, PHN: postherpetic neuralgia.
|
The IENFD values obtained by IF and IHC in the healthy participant group were 6.54±1.21 and 6.44±1.41 fibers/mm, respectively; the corresponding values for patients with SFN were 1.99±0.76 and 2.32±0.26 fibers/mm, respectively, and those for the patients with PHN were 3.06±2.57 and 2.87± 1.72 fibers/mm, respectively. The three-dimensional evaluation using ACT-PRESTO showed that the IENFD in the healthy groups was 90.19±30.18 fibers/mm2. The mean IENFD for the patients with SFN was 48.12 fibers/mm2, and the IENFD in the patients with PHN was 47.21±28.00 fibers/mm2. There was a significant correlation between the IENFD values quantified using conventional two-dimensional methods and the new three-dimensional approach, with a correlation coefficient of 0.65 for IF (p<0.01) and 0.56 for IHC (p<0.05).
Go to :
DISCUSSION
Cutaneous nerve biopsies are a credible method for evaluating the loss and regeneration of sensory nerve fibers in patients with peripheral neuropathies.12345 A cutaneous nerve biopsy with quantification of the IENFD could be used to diagnose SFN or groups of conditions in which small nerve fibers are compromised.4 The presence of PHN after herpes zoster infection is also reportedly related to a significant loss of IENFs.1314 In addition, nerve regeneration after multiple types of treatment is reportedly associated with neuropathies including diabetes mellitus and HIV.1516
The EFNS guidelines for performing cutaneous nerve biopsies describe a series of procedures, including 3-mm punch biopsies at the distal leg; examination of the linear epidermal density in at least three sections per biopsy, fixation in Zamboni's solution, and staining with anti-PGP 9.5 antibodies; and imaging by bright-field IHC or IF using confocal microscopy as the diagnostic standard for SFN.12
However, this traditional method has two unavoidable limitations. First, the original skin biopsy sample must be sectioned into thin specimens to ensure the effective penetration of macromolecules and valid microscopic visualization without unwanted light scattering,171819 and this cutting process could disturb the intrinsic structural organization. Second, previous assessments have been restricted to images of tissue sections in the XY plane.127 Consequently, intact complex arborizing patterns of cutaneous nerve fibers have never been evaluated in peripheral neuropathies, and extremely limited aspects of whole structures have been used in conventional quantification procedures.
The ability to perform volume imaging of intact cutaneous nerve fibers at high speed and in a consistent manner by using cutaneous ACT-PRESTO could offer a new perspective in the field of diagnostic assessment for sensory nerve dysfunctions. Previously reported tissue-clearing methods for volume imaging not only require prolonged times for clearing (typically more than 1–2 weeks), these techniques also have a possible risk of tissue damage owing to unstable temperatures, uncontrolled alteration of pH, and impeding of circulatory currents by air bubbles.719 In comparison, the cutaneous ACT-PRESTO technique considerably shortens the duration of the overall procedure to 4 days, including only 4 h of tissue-clearing, with little damage to the cleared tissue owing to controlling the electric current, pH, temperature, and air bubbles.67 These improvements in the required time and reliability could facilitate the acquisition of three-dimensional information on cutaneous nerve fibers in a clinical setting. When using ACT-PRESTO, patients with sensory nerve dysfunction can expect to receive examination results based on volume imaging within 4 days from the time of performing the cutaneous nerve biopsy to obtaining images of intact peripheral nerve fibers and related quantitative data.
The present study was originally designed to determine whether three-dimensional imaging and related volume information could be utilized to diagnose sensory nerve dysfunctions. The obtained results indicated that the quantified IENFD values obtained from volume imaging were also significantly correlated with the results obtained using the conventional gold-standard approach. However, this study was subject to the limitations of relatively small numbers of subjects and the heterogeneous constitution of the included neuropathy patients, although both the SFN and PHN patients showed reduced IENFD values.
In our future work we will assess intact three-dimensional structures of cutaneous nerve fibers in more-detailed morphological analyses, including of the total length, complexity, and various angles among distinct segments of nerve fibers. Such a study involving larger numbers of subjects and detailed analyses of volume information could contribute to elucidating the pathophysiological mechanisms of certain peripheral neuropathies at the subclinical stage, by broadening the understanding of important morphological changes in sensory nerve endings.
Go to :
 XML Download
XML Download