

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary progressive aphasia (PPA) is a clinical dementia syndrome characterized by progressive language dysfunction.1 Three clinical variants of PPA are recognized: the nonfluent/agrammatic variant (nfvPPA), the semantic variant (svPPA), and the logopenic variant (lvPPA).2
The underlying pathologies of PPA are heterogeneous and distinct for each PPA subtype. Tau is a key protein associated with various neurodegenerative diseases including PPA, and can be expressed with three repeat (3R) or 4R domains that arise from alternative splicing of the tau exon.3 Previous pathological studies have shown associations of 4R tau with nfvPPA and of 3R+4R tau with lvPPA.45 The svPPA variant is more commonly associated with TAR DNA-binding protein 43 (TDP43) than tau.456
Several radiotracers have been developed to facilitate the in-vivo visualization of tau pathology. [18F]-THK5351, an 18F-labeled THK arylquinoline tracer, has a high binding affinity and selectivity for tau.7 However, the potential for off-target binding with monoamine oxidase-B (MAO-B) has been reported recently.8 We previously reported our findings from an [18F]-THK5351 PET study of nfvPPA and svPPA patients.910 In the present study we sought to characterize the pattern of [18F]-THK5351 retention across all three PPA subtypes and determine the topography of [18F]-THK5351 retention correlated with each neurolinguistic score.
METHODS
Participants
Thirteen participants who had been clinically diagnosed with PPA at Gachon University Gil Medical Center from March 2015 to August 2017 were enrolled in the study. By using the clinical diagnostic criteria for the diagnosis of PPA and its variants,2 patients with PPA were classified into one of the three variants, which resulted in three nfvPPA, five svPPA, and five lvPPA classifications. All subjects underwent [18F]-THK5351 PET and 3.0-tesla magnetic resonance imaging (MRI).
Thirty-seven participants with normal cognition (NC) with no history of neurological or psychiatric illness or abnormalities detected in neurological examinations were also included. [18F]-flutemetamol (FLUTE) PET scans of all NC participants were negative for amyloid pathology.
This study was approved by the Institutional Review Board of Gachon University Gil Medical Center, and written informed consent was obtained from each participant (IRB No. GDIRB2015-272).
Neuropsychological and neurolinguistic tests
Eleven of the 13 PPA participants underwent a comprehensive neuropsychological evaluation using the Korean version of the Western Aphasia Battery, which comprises subscales to assess spontaneous speech, auditory verbal comprehension, repetition, naming and word finding, reading, and writing.11 All participants underwent a comprehensive neuropsychological evaluation using the Seoul Neuropsychological Screening Battery-II.12
Image acquisition and preprocessing
MRI image acquisition
All participants underwent a 3 dimensional (3D) T1-weighted magnetization-prepared rapid gradient-echo (T1-MPRAGE) scan using a 3-tesla MRI scanner (Verio, Siemens, Erlangen, Germany). The following 3D T1-MPRAGE imaging parameters were used: repetition time=1,900 ms, echo time=2.93 ms, flip angle=8°, pixel bandwidth=170 Hz/pixel, matrix size=256×208, field of view=256 mm, and total acquisition time=4 min and 10 s. The isovoxel resolution was 1.0 mm.
PET image acquisition
All PET scans were acquired using a Siemens Biograph 6 Truepoint PET/computed tomography (CT) scanner (Siemens) in list-mode emission acquisition. All PPA participants underwent a 20-min emission scan starting 50 min after 185 MBq [18F]-THK5351 was injected intravenously (i.e., from 50 to 70 min). The [18F]-THK5351 was synthesized and radiolabeled at the Gachon University Neuroscience Research Institute. All NC subjects and 7 of the 13 PPA patients underwent a 20-min emission scan 90 min after the intravenous injection of 185 MBq [18F]-FLUTE (i.e., from 90 to 110 min). Low-dose CT was performed for attenuation correction prior to all scans. The images were reconstructed onto a 256×256× 109 matrix with a voxel size of 1.3×1.3×1.5 mm3 using a 2D ordered subset expectation maximization algorithm (8 iterations and 16 subsets), with corrections for physical effects.
Image processing and analysis
Individual [18F]-THK5351 PET images were coregistered onto individual T1-weighted images using FreeSurfer software (version 6.0, surfer.nmr.mgh.harvard.edu) and MRI parcellation was performed as described previously.13 Region-based partial volume correction (PVC) was applied to the PET images using the PETSurfer tool in FreeSurfer. In order to compare [18F]-THK5351 retention in each group quantitatively, we defined the following 18 regions of interest (ROIs): the precentral cortex, prefrontal cortex (frontal pole, pars orbitalis, orbital frontal, pars triangularis, pars opercularis, and rostral middle frontal, superior frontal, caudal middle frontal, and medial orbital frontal regions), inferior frontal cortex (triangular part of the inferior frontal gyrus, opercular part of the inferior frontal gyrus, and orbital part of the inferior frontal gyrus), Broca's area (triangular and opercular parts of the left inferior frontal gyrus), lateral temporal cortex (superior, middle, and inferior temporal cortices), mesial temporal cortex (hippocampus, amygdala, and parahippocampal and entorhinal cortices), fusiform gyrus, inferior temporal cortex, temporal pole, superior parietal cortex, inferior parietal cortex (inferior parietal and supramarginal regions), insula, anterior cingulate cortex (accumbens, caudal anterior cingulate, and rostral anterior cingulate regions), posterior cingulate cortex, occipital cortex (cuneus, and pericalcarine and lateral occipital regions), striatum (putamen and pallidum), neocortex (comprising the prefrontal, superior parietal, lateral temporal, inferior parietal, occipital, anterior cingulate, mesial temporal, and posterior cingulate cortices, and precuneus), and brainstem. Regional standardized uptake-value ratios (SUVRs) were created with reference to the cerebellar gray matter for THK images1415 and to the pons for FLUTE images.16 SUVR images were generated from the coregistered MRI and PET images with voxel-wise PVC.1718 An SUVR threshold of 0.62 for amyloid positivity was applied to the [18F]-FLUTE PET data.16
Statistical analysis
When performing group comparisons of the demographic and clinical data, we used the Kruskal-Wallis test with Dunn's procedure for comparing continuous variables and the chi-square test chi square test for comparing categorical variables for comparing categorical variables. The mean and standarddeviation values for the regional THK SUVRs from the 37 NC subjects were used to calculate regional Z scores for the SUVR. Spearman's correlation was used to explore the relationship between the score in each neurolinguistic test and [18F]-THK5351 retention. Correlations between the regional cortical thickness and regional [18F]-THK5351 retention or each neurolinguistic score were also evaluated with Spearman's correlation analyses.
All statistical analysis was performed using SPSS Statistics (version 19, IBM Corp., Armonk, NY, USA). A voxel-wise analysis was also conducted to compare regional patterns of THK retention using SPM (Statistical Parametric Mapping) software (version 12, Wellcome Trust Centre for Neuroimaging, London, UK). For each diagnostic group, voxelwise comparisons of SUVR images were performed using a one-way analysis of covariance with adjustment for age, sex, and years of education. Voxel-wise analyses of the correlations between the various neurolinguistic scores and [18F]-THK5351 retention were performed using Spearman's correlation. The results are presented for a significance threshold of p<0.001.
RESULTS
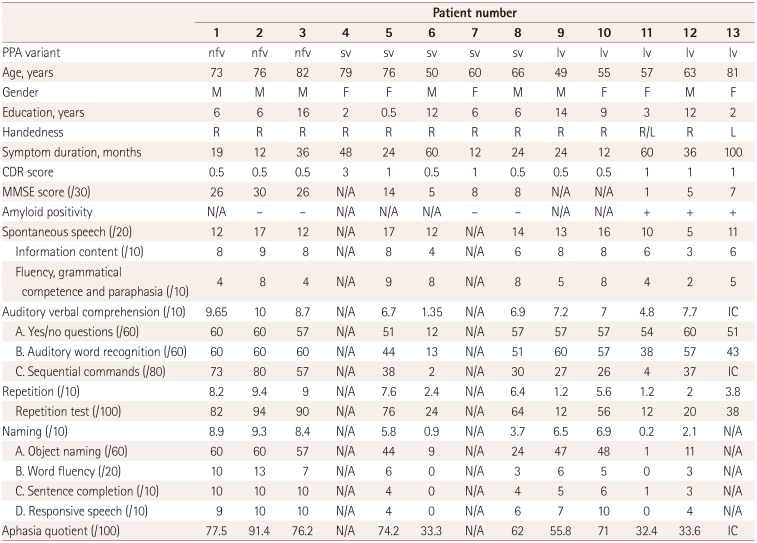
Individual PPA cases are summarized in Table 1, and the demographics and clinical characteristics of each group are presented in Supplementary Table 1 (in the online-only Data Supplement). The age and sex distributions did not differ significantly between the NC subjects and PPA patients. Individual [18F]-THK5351 and MRI images are shown in Supplementary Fig. 1 (in the online-only Data Supplement).
Voxel-wise and ROI-based analyses of [18F]-THK5351 retention in the three PPA subtypes
Voxel-wise analyses revealed that the [18F]-THK5351 retention in the left inferior frontal and precentral gyri was higher in the nfvPPA patients than the NC participants (Fig. 1A), while that in the anteroinferior and lateral temporal cortices was higher in svPPA patients than in the NC group (left>right) (Fig. 1B). lvPPA patients exhibited increased [18F]-THK5351 retention in the inferior parietal, lateral temporal, and dorsolateral prefrontal cortices, and precuneus (left>right) (Fig. 1C).
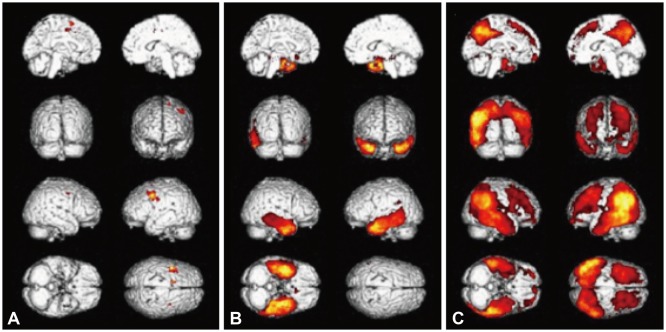
Fig. 1
[18F]-THK5351 retention in nfvPPA, svPPA and lvPPA patients. Voxel-wise comparisons of [18F]-THK5351 retention between PPA and NC subjects. Results are presented for a significance threshold of p<0.001, uncorrected for multiple comparisons after adjustment for age, gender, and years of education. A: nfvPPA>NC. B: svPPA>NC. C: lvPPA>NC. lv: logopenic variant, NC: normal cognition, nfv: nonfluent/agrammatic variant, PPA: primary progressive aphasia, sv: semantic variant.
![]()
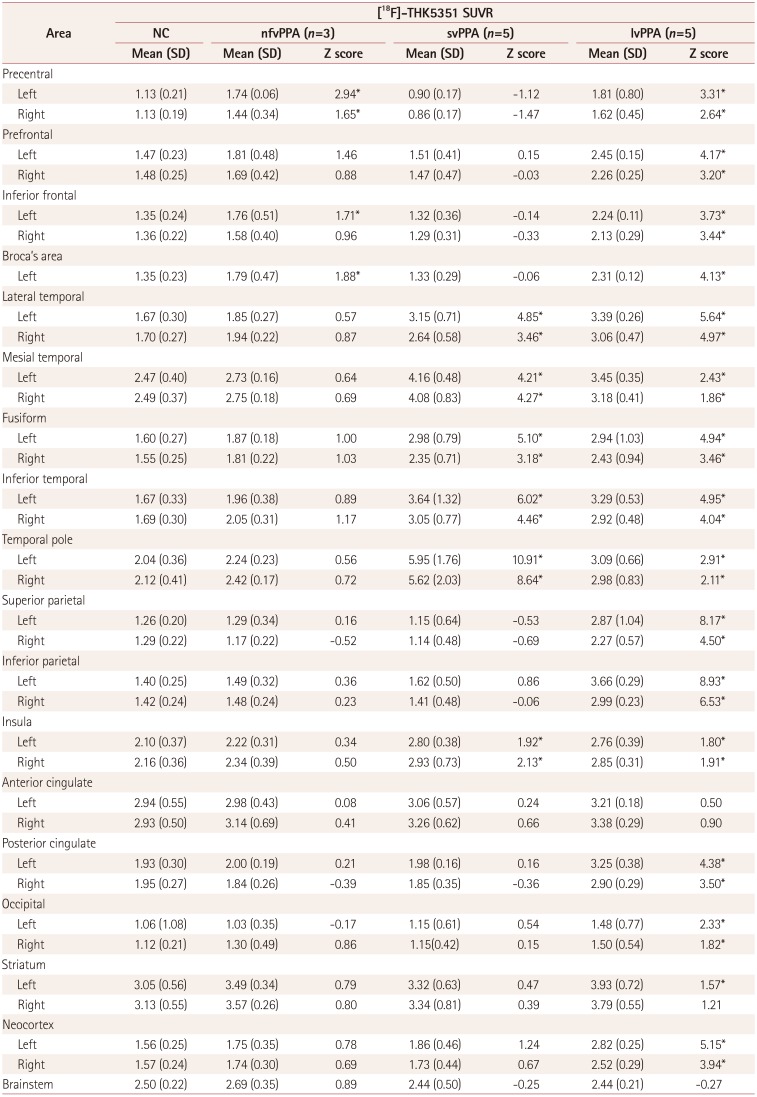
The results of the statistical ROI assessments after performing PVC are summarized in Table 2. With a cutoff Z score of 1.5, nfvPPA patients showed greater [18F]-THK5351 binding than NC subjects in the Broca's area, bilateral precentral gyri, and left inferior frontal lobe. svPPA patients had higher [18F]-THK5351 retention in the bilateral lateral temporal, mesial temporal, and inferior temporal cortices, temporal poles, fusiform gyri, and insula, while lvPPA patients showed higher [18F]-THK5351 retention than NC subjects over widespread regions (except the anterior cingulate area and brainstem), with predominance in the left parietal area. The detailed findings from the ROI analysis of the 13 PPA patients are presented in Supplementary Tables 2, 3, 4 (in the online-only Data Supplement).
Correlations between [18F]-THK5351 retention or cortical atrophy and neurolinguistic test scores
Fig. 2 presents the brain areas where [18F]-THK5351 retention increased as each neurolinguistic score decreased. Reduced fluency was associated with [18F]-THK5351 retention in the left inferior frontal gyrus. Impairment of comprehension was associated with [18F]-THK5351 retention in the fusiform gyri and the mesial temporal and lateral temporal cortices, including the temporal pole. The areas of [18F]-THK5351 retention associated with repetition were the bilateral inferior parietal and posterior part of the lateral temporal cortices (left>right). Naming difficulty was correlated with [18F]-THK5351 retention in the left fusiform gyrus and left mesial temporal area and bilateral posterior parts of the lateral temporal cortices.
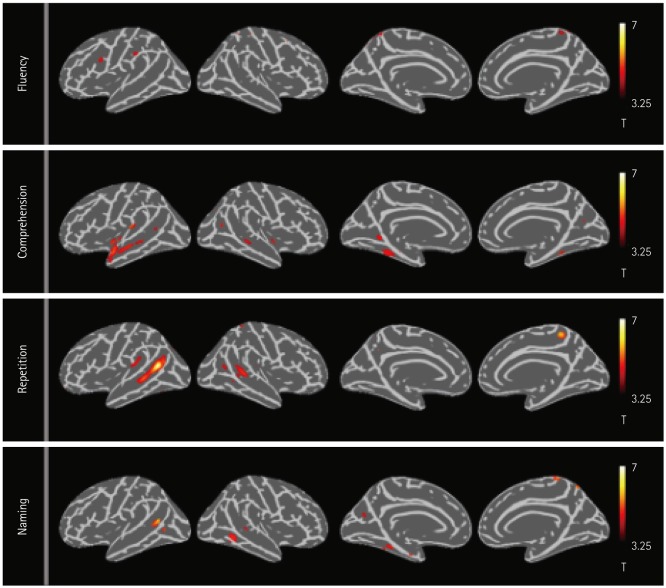
Fig. 3 shows the ROIs that were significantly correlated with each neurolinguistic score. The comprehension score was negatively correlated with [18F]-THK5351 retention in the left mesial temporal cortex and temporal pole. THK SUVR values for the left inferior parietal lobe were negatively correlated with the repetition score. The naming score was negatively correlated with THK SUVR values for the left lateral temporal and mesial temporal cortices, fusiform gyrus, and temporal pole.
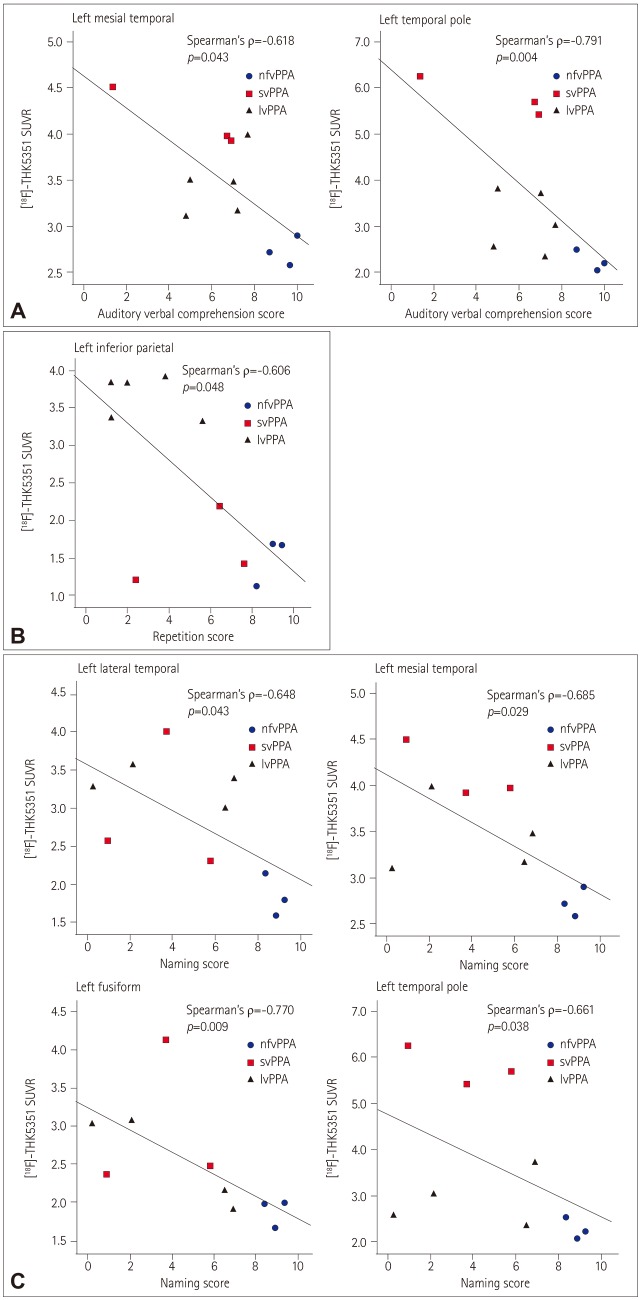
Fig. 3
Correlations between neurolinguistic test scores and regional SUVR for [18F]-THK5351. Spearman's rho and p values are presented. A: Comprehension. B: Repetition. C: Naming. lv: logopenic variant, nfv: nonfluent/agrammatic variant, PPA: primary progressive aphasia, SUVR: standardized uptake-value ratio, sv: semantic variant.
![]()
Supplementary Fig. 2 (in the online-only Data Supplement) shows the regional cortical thickness was correlated with [18F]-THK5351 retention in the same region. The regional cortical thickness was correlated with [18F]-THK5351 retention in the bilateral fusiform gyri, bilateral temporal poles, bilateral inferior parietal cortices, and left prefrontal, left precentral, left inferior temporal, left superior parietal and left posterior cingulate cortices, and right insula.
Supplementary Fig. 3 (in the online-only Data Supplement) shows that the regional cortical thickness was significantly correlated with each neurolinguistic score. Fluency was positively correlated with the regional cortical thickness in the left precentral gyrus and left superior and inferior parietal cortices. Comprehension was correlated with the cortical thicknesses of the left temporal pole, bilateral lateral temporal and inferior temporal cortices and bilateral fusiform gyri. Repetition was positively correlated with the regional cortical thicknesses of the left inferior temporal and fusiform gyri, and bilateral lateral temporal cortices. The naming score was positively correlated with the regional cortical thicknesses of the bilateral lateral temporal and inferior temporal cortices and left fusiform gyrus, temporal pole, and insula.
DISCUSSION
In this study, we found distinct regional patterns of [18F]-THK5351 retention across the three PPA subtypes, which is consistent with the findings of previous studies using a different tau radiotracer.1920 The regional patterns of [18F]-THK5351 retention were well matched with the clinical and radiological findings for each PPA subtype. A recent study found that [18F]-THK5351 retention might be detectable even in the very early stage and suggested that [18F]-THK5351 PET imaging might facilitate early diagnosis of PPA.21 Our findings, along with those of previous studies, indicate that [18F]-THK5351 PET imaging could support the diagnosis and differentiation of PPA variants.
We observed that in PPA patients, [18F]-THK5351 retentions were related to language deficits, which was well matched with findings from previous neuroanatomical and neurofunctional studies. Declining speech fluency is a key feature of nfvPPA. In our SPM analysis, the areas of THK retention correlated with reduced fluency scores included the left inferior frontal and precentral gyri, the same areas that showed prominent atrophy in the nfvPPA patients. The left inferior frontal gyrus is the location of Broca's area responsible for speech production. Apraxia of speech (AOS), an impairment of the motor programming of speech that might affect the capacity for speech fluency and frequently manifests in nfvPPA. Previous studies have found AOS to be associated with damage to the left precentral gyrus22 and atrophy of the left inferior frontal gyrus.23 However, our ROI analysis did not reveal any areas that were significantly correlated with declining fluency, which might have been due to less robust and more focal [18F]-THK5351 uptake in the nfvPPA patients.
[18F]-THK5351 uptake was increased in the anteroinferior and lateral temporal regions in the svPPA patients (bilaterally, left>right). Impaired comprehension of word meaning is the primary feature of svPPA. The comprehension score was negatively correlated with [18F]-THK5351 retention in the left temporal areas in this study. The region of the brain traditionally associated with the comprehension of language is Wernicke's area located in the superior temporal gyrus. Other temporal regions have been also identified as being involved in language comprehension. The middle temporal gyrus is important for comprehension at the word level,24 and the semantic hub, a part of the language network, might be located in the anterior temporal lobe.25
The inferior parietal and posterior temporal areas featured lesions showing predominant [18F]-THK5351 uptake in lvPPA patients and a negative correlation with repetition score. lvPPA is characterized by a compromised ability to repeat phrases and predominant atrophy of the left temporal and parietal areas. Many studies have suggested that the left inferior parietal lobe is an important area for speech repetition, 26 and the temporoparietal junction plays a role in translating auditory speech code into articulatory code.27
Naming difficulty was correlated with [18F]-THK5351 retention in the left temporal area, including the lateral and posterior temporal cortices. A recent study showed that superior portions of the left temporal pole and left posterior temporal cortices impact semantic and lexical naming mechanisms in svPPA and lvPPA, respectively.28 That study found that naming deficit occurred only rarely in nfvPPA patients.28 Our nfvPPA patients also exhibited relatively good naming scores compared to the other PPA subtypes.
In this study, we evaluated the brain regions of [18F]-THK 5351 retention that was correlated with neurolinguistic deficits in PPA patients with heterogeneous pathologies. The pathological heterogeneity of three PPA subtypes could have affected the results because the binding affinity of [18F]-THK5351 and the mechanism underlying [18F]-THK5351 retention might differ according to the pathology underlying each PPA subtype. The most common pathology of nfvPPA is known to be frontotemporal lobar degeneration tau, including 4R tau, whereas TDP43 and Alzheimer's disease pathologies are predominantly observed in svPPA and lvPPA, respectively.6 A previous postmortem study suggested that [18F]-THK5351 is a sensitive and selective tracer for tau deposits in Alzheimer's disease and 4R tauopathy diseases, including corticobasal degeneration and progressive supranuclear palsy, but with a low binding affinity of [18F]-THK5351 to TDP43.29 [18F]-THK 5351 binding to MAO-B, a biomarker for astrocytosis in neuroinflammation and neurodegeneration,8 has been suggested as a possible mechanism underlying [18F]-THK5351 retention in svPPA with TDP43 pathology. [18F]-THK5351 retention can be explained by tau pathology itself in lvPPA and nfvPPA, but the possibility of MAO-B-related retention remains.
Several limitations of this study should be noted when considering its findings. The study only examined a small number of patients, and so validation in a larger population is needed. Another major limitation was the lack of pathological confirmation. In addition, one svPPA patient (case 5) showed Wernicke's aphasia, however, THK retention and cortical atrophy were more prominent in the right than the left temporal area. Her initial symptom was abnormal behavior, but language problems in comprehension developed about 1 year thereafter. Finally, visual inspection of the THK images showed high [18F]-THK5351 retention in the frontal white matter (WM) in nfvPPA patients. This could be confounded by the marked cortical atrophy in the corresponding area, and so all images were corrected for partial volume effects and WM spillover to confirm higher cortical [18F]-THK5351 retention in this study. However, previous [18F]-flortaucipir PET studies found that [18F]-flortaucipir uptake was also increased in the frontal WM as well as the frontal cortex.1920 Although we did not evaluate the regional WM SUVR due to the strong nonspecific WM binding of [18F]-THK5351,7 this was also a limitation of the present study.
In conclusion, the distribution of [18F]-THK5351 retention might be informative when diagnosing and differentiating PPA variants. The topography of [18F]-THK5351 retention correlating with each language domain deficit was well matched with the findings of previous neuroanatomical and neurofunctional studies. However, issues regarding the ligand's specificity remain, and pathological confirmation would improve the ability to interpret the present findings.
 XML Download
XML Download