

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Small-fiber neuropathy (SFN) is a peripheral nerve disorder that selectively affects the thinly myelinated Aδ fibers and unmyelinated C fibers, and commonly presents with neuropathic pain, autonomic dysfunction, and hypesthesia to pain and temperature. Symptoms typically show a symmetric length-dependent pattern that develops from the distal part of the body. Many patients report the gradual onset of abnormal sensations in the feet, such as burning pain, electric-shock-like pain, tingling sensation, or pins-and-needles sensation. A non-length-dependent distribution with patchy or proximal involvement has also been reported.1 Autonomic symptoms of varying severities including abnormal sweating, dry eyes, dry mouth, orthostatic dizziness, diarrhea, constipation, and/or erectile dysfunction can occur. Although several causes of SFN have been identified, the etiology is unknown in 30–50% of cases.2 Diabetes mellitus that includes glucose intolerance, autoimmune disease, and sodium channelopathy are known to the most-common underlying causes of pure SFN.23
Clinically diagnosing SFN is challenging because the clinical signs of small-fiber damage are often not definite. In addition, routine nerve conduction studies (NCSs) cannot detect abnormalities that are confined to small fibers.4 Diagnosing SFN can be supported by using quantitative sensory testing (QST) to assess the thermal and pain thresholds. However, the visualization and quantification of epidermal nerve fibers in skin biopsies facilitate more-reliable diagnoses of SFN and the recognition of SFN as a distinct clinical entity. The quantitative sudomotor axon reflex test (QSART) could provide additional information about autonomic dysfunction by evaluating the postganglionic sympathetic cholinergic sudomotor function. In Korea, skin biopsies are used to evaluate epidermal nerve fibers in research studies, but QST and QSART are only performed in some tertiary hospitals. Although we commonly encounter patients who are suspected as having SFN, few clinical studies have investigated SFN. In addition, Korean patients frequently report a cold sensation and cold dysesthesia that is called ‘Sirim’ in Korean. However, this symptom is not well characterized and its pathophysiology is currently unknown. There is no equivalent term for ‘Sirim’ in English, but it usually overlaps with an unprovoked unpleasant cold sensation and/or high sensitivity to cold on the skin and/or deeper parts of the body such as the bones and joints. Here we also describe ‘Sirim’ (cold) pain as a ‘Sirim’ sensation that is sufficiently severe to cause pain, and have added it as one of the SFN-associated symptoms.
The objective of the present study was to identify the clinical symptom profile, including their ‘Sirim’ pain, diagnostic test results of QST and QSART, possible etiologies, and quality of life (QOL) in patients with clinically suspected SFN.
METHODS
This prospective study was performed between March 2016 and March 2017 at Samsung Medical Center, which is tertiary referral center in Korea. We defined clinically suspected SFN as follows: 1) the presence of at least two sensory symptoms suggestive of SFN, such as pain (e.g., burning, shooting, or prickling), allodynia, lower thermal sensation, hyperesthesia, or paresthesia in which symptoms are length-dependent; 2) abnormal results in either QSART or QST [cold detection threshold (CDT)]; 3) normal NCS findings; and/or 4) signs of small-fiber damage.5 The application of these criteria resulted in the enrollment of 63 consecutive patients with clinically suspected SFN (Fig. 1). The exclusion criteria were 1) the involvement of large nerve fibers or the CNS in neurologic examinations, as indicated by muscle weakness, decreased position/vibration sense, decreased deep tendon reflex, or upper motor neuron signs; 2) the presence of obvious causes, other than SFN, explaining sensory symptoms; 3) an inability to understand and/or sign a written consent form; or 4) being younger than 18 years.
Motor and sensory NCSs were performed using standard surface stimulation and recording techniques6 with in-house normal values to measure the bilateral median, ulnar, peroneal, and tibial motor nerves, and the median, ulnar, and sural sensory nerves. If needed, needle EMG of intrinsic foot muscles (abductor hallucis and extensor digitorum brevis muscles) was performed to rule out radiculopathy.
We assessed SFN by performing QST and QSART. CDT and the warm detection threshold (WDT) were determined by QST on either side of the hand and foot that was more symptomatic using the Computer Aided Sensory Evaluator-IV (WR Medical Electronics, Maplewood, MN, USA). However, we adopted an elevated CDT as the standard for abnormality with an established reference value. Postganglionic sudomotor functions at the forearm, proximal leg, distal leg, and foot on the side with the worst symptoms were assessed by QSART using a Q-Sweat machine (WR Medical Electronics). Some of the patients refused to undergo QST (n=6/63, 9.5%) or QSART (n=7/63, 11%) because of the personal cost to them or for other personal reasons.
SFN-associated symptoms were assessed using the ordinal 13-item Small-Fiber Neuropathy Symptoms Inventory Questionnaire (SFN-SIQ) plus a ‘Sirim’ item scored as follows: 0, never present; 1, sometimes present; 2, often present; and 3, always present. The pain profile was evaluated using the Neuropathic Pain Symptom Inventory (NPSI) questionnaire plus ‘Sirim’ pain. Each of these items was quantified on an 11-point numerical rating scale (NRS) ranging from 0 to 10 for the average pain over the past 24 hours. The bilateral dorsalis pedis and posterior tibial pulses were palpated to exclude peripheral artery disease. In addition, the ankle-brachial index and peripheral vessel ultrasonography were applied to patients with clinical suspicion of vascular insufficiencies. QOL was assessed using the 36-item Short-Form Health Survey (SF-36), with scores ranging from 0 to 100, and higher scores indicating better QOL. Two summary scores of SF-36 were used for the analysis: physical component score (PCS) and mental component score.
To determine the etiology of SFN, we obtained the past medical history and social history, including the use of drugs and alcohol. We performed blood tests including the complete blood count, erythrocyte sedimentation rate, fasting glucose, glycosylated hemoglobin, fasting lipid profile (cholesterol and triglycerides), liver function test, renal function test, thyroid function test (thyroid stimulating hormone, free thyroxine, and triiodothyronine), electrolytes (sodium, potassium, and chlorine), vitamin B12, folate, antinuclear antibodies, antibodies against SSA/SSB and double-strand DNA, rheumatoid factor, angiotensin-converting enzyme, serum protein electrophoresis, and serologies (hepatitis B and C viruses, HIV, and rapid plasma regain). Additional laboratory tests (oral glucose tolerance test, serum immunofixation, α-galactosidase, and/or GLA for Fabry's disease, and abdominal fat biopsy for amyloidosis) were added based on clinical suspicions. Genetic tests for sodium- or potassium-channel mutations were not performed. This study was approved by the Institutional Review Board of Samsung Medical Center (IRB No. 2015-10-158), and written informed consent was obtained from all participants.
Correlations between scores for SFN-related symptoms (SFN-SIQ items and ‘Sirim’) and neuropathic pain symptoms (NPSI items and ‘Sirim’ pain) were assessed using Spearman's correlation analysis. A correlation was considered to be significant for Spearman's rho (ρ)>0.3 and p<0.01. Logistic regression analysis was performed to evaluate predictors for QST (CDT) or QSART abnormalities after controlling for age, sex, and disease duration. Each NPSI item or each SFN-SIQ item and ‘Sirim’ pain were included as independent variables. Multiple linear regression analysis was used to evaluate risk factors associated with QOL. The presence of possible etiology for SFN was added as an independent variable to the aforementioned independent variables. Group differences (patients with idiopathic vs. nonidiopathic SFN) were analyzed using the chi-square test or Fisher's exact test for categorical variables, and using Student's t test or the Mann-Whitney U test for continuous variables. All data analyses were performed with SPSS (version 20.0, IBM Corp., Armonk, NY, USA) and R software, which is freely available from the CRAN repository (https://cran.r-project.org/).
RESULTS
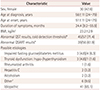
This study included 63 patients (30 females and 33 males) aged 56±11 years (mean±SD) (Table 1). The QST (CDT) and QSART findings were abnormal in 71% (n=45/57) and 62% (n=39/56) of the patients, respectively. The most-common cause was idiopathic, comprising 65% (n=41) of the patients. The most-common known cause was poor glycemic control (11%, n=7), followed by thyroid dysfunction (6%, n=4). In a few cases, autoimmune dysfunction, infections, and alcohol consumption also contributed.
SFN symptom profile
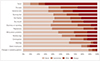
‘Sirim’ was the most-common symptom questionnaire item. Fifty-seven patients (90%) experienced ‘Sirim’ while 70% of them (n=43) always suffered from it (Fig. 2). Other frequently reported symptoms included dry eyes (65%), sensitive skin (65%), and burning feet (59%). Changes in the sweating pattern and sheet intolerance were the least-common symptoms.
Neuropathic pain symptom profile
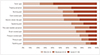
Every patient reported that they experienced pain. Among the pain symptom categories, the most-common and most-severe symptom was ‘Sirim’ pain (NRS score=6.3±3.5, 84% of the patients had ‘Sirim’ pain and 59% of them showed an NRS score of >7) (Fig. 3), followed by tingling sensation (4.3±3.6), cold-evoked pain (3.8±4.1), electric-shock-like pain (3.6±3.3), burning pain (3.3±3.6), squeezing pain (2.9±3.5), and pins-and-needles sensation (2.2±2.9). Among pain symptoms, only the severity of ‘Sirim’ pain was associated with age (ρ=0.316, p=0.013): patients with more-severe ‘Sirim’ pain tended to be older. When we divided patients into two groups using a pain cutoff score of 4 on NRS, patients with higher pain scores (NRS score ≥4, n=47) were older (p=0.012), had longer disease duration (mean=52 months vs. 22 months in patients with NRS scores <4, p=0.008), and possible causes of SFN (47% vs. 0%, p<0.001).
Correlations between SFN-symptom and pain measures
Spearman's correlation analysis revealed weak positive correlations (ρ=0.3–0.5) between SFN-associated symptoms (Fig. 4). The frequencies of autonomic and sensory symptoms tended to be correlated with each other. However, burning feet was only correlated with hot flashes and sheet intolerance, while ‘Sirim’ was not correlated with other symptoms.
Most NPSI items exhibited significant correlations with each other. The correlations were strongest between squeezing and pressure pain (ρ=0.492, p<0.001), between stabbing pain and pins-and-needles sensation (ρ=0.559, p<0.0001), and between brush-evoked and pressure-evoked pain (ρ=0.720, p<0.0001). However, ‘Sirim’ pain was only positively correlated with cold-evoked pain (ρ=0.420, p<0.0001) and tingling sensation (ρ=0.248, p<0.0001).
QST and QSART
Fifty patients underwent both QST (CDT) and QSART, whose findings were abnormal in 76% (n=38) and 66% (n=33) of them, respectively. In 38 patients with abnormal CDT, elevated CDT was found in the foot of 26 patients (68%), while 14 patients (out of 26, 54%) also had abnormal CDT in the hand. QSART findings were abnormal in the foot in 24 patients (out of 33 patients with an abnormal result; 73%), while a length-dependent pattern of abnormality (abnormal QSART findings in the foot only; foot and distal leg; and foot, distal leg, and forearm) was found in 15 patients (45%). Global sudomotor dysfunction was found in 1 patient (3%), while regional or patchy sudomotor dysfunction was found in 17 patients (52%).
We divided patients into three groups according to CDT and QSART results: 1) abnormal CDT and normal QSART findings (n=17), 2) normal CDT and abnormal QSART findings (n=12), and 3) abnormal CDT and abnormal QSART findings (n=21) (Fig. 5). The stabbing pain was more severe in the group with only abnormal CDT (odds ratio=2.23, 95% CI=1.02–4.87, p=0.045) than in the group with both abnormal CDT and abnormal QSART findings in multinomial multiple logistic regression analysis after controlling for age, sex, and disease duration. There were no significant differences in pain descriptors (NPSI and ‘Sirim’ pain) between the group with only abnormal QSART findings and the group with both abnormal CDT and QSART findings.
Idiopathic and nonidiopathic SFN patients
The demographic characteristics, the presence of CDT or QSART abnormality, and QOL (physical and mental aspects) did not differ significantly between patients with idiopathic and nonidiopathic SFN (Supplementary Table 1 in the online-only Data Supplement). However, nonidiopathic SFN patients experienced burning feet and ‘Sirim’ more frequently (uncorrected p=0.011 and p=0.003, respectively), and more-severe brush-evoked pain, tingling sensation, and ‘Sirim’ pain (uncorrected p=0.001, p=0.023, and p=0.004, respectively).
Predictors of QOL
In multiple linear regression analysis, restless-leg symptoms (β=−7.077, p=0.046) and pressure-evoked pain (β=−5.034, p=0.016) were independent predictors of the physical aspects of QOL (R2=0.671). However, there was no significant predictor of the mental aspects of QOL in the patients. Abnormal CDT or QSART findings or the presence of probable etiology was not associated with QOL in patients with clinically suspected SFN.
DISCUSSION
SFN has received increasing attention over the past few years. SFN is a relatively common disorder that often presents with neuropathic pain, especially burning or sharp pain, and dysesthesia that might be difficult to control. In the present study we found that ‘Sirim’ and ‘Sirim’ pain were the most-common and most-severe complaints in patients with clinically suspected SFN. Because ‘Sirim’ refers to a cold sensation in one part of the body that is severe enough for the patient to feel cold throughout, the characteristics of ‘Sirim’ pain are closely related to those of cold pain.
Cold pain has been recognized as one of the SFN-associated symptoms, but its frequency and mechanism remain unclear. A previous study of 67 patients with pure SFN (defined as those with abnormal CDT and/or WDT and reduced density of intraepidermal nerve fibers) found that only 2 patients (3%) described their pain as cold, while 18 patients (26.8.%) reported cold allodynia.7 However, ‘Sirim’ was very common in our study (with 70.5%, 8.2%, 11.5%, and 9.8% of the patients describing it as being always, often, sometimes, and never present, respectively), while cold allodynia (56%) was also frequently accompanied with ‘Sirim.’ Recognition of cold pain as a common symptom of SFN in our study and ethnicity differences compared with the previous study7 might explain such differences. SFN-SIQ does not include cold pain. Among neuropathic pain screening questionnaires, only Neuropathic Pain Questionnaire (NPQ) and Douleur Neuropathique (DN4) contain an item questioning pain of a cold nature.8 Previous studies have suggested that the experience of pain differs among different ethnic groups,910 with African Americans showing lower thermal and ischemic pain tolerances than non-Hispanic Whites.1011 However, few studies have examined other ethnic groups, including Koreans.
Cold pain may result from defective regulation of the skin microcirculation. Intact adrenergic vasoconstrictor nerves and thermally sensitive afferents are required to regulate peripheral blood flow in response to local warming or cooling.4 Hypothermic skin is also frequently found in patients with cold hyperalgesia or allodynia, and either sympathetic denervation supersensitivity or exaggeration of the sympathetic vasoconstrictor outflow mechanism could contribute to this.12 Our study found that cold pain was more severe in older patients, which might be partly due to the presence of cutaneous vasomotor dysfunction.13 In addition, dysfunctional Aδ and nociceptive C fibers can cause an abnormal skin cold sensation and cold pain/allodynia. The characteristics of the cold hypersensitivity differed between patients, which might reflect different underlying neurophysiological mechanisms. Defective cold-specific Aδ afferent input might disinhibit cold-sensitive C-polymodal nociceptive fiber pathways. Thus, paradoxical burning pain could be provoked by innocuous cooling.14 Peripheral sensitization of Aδ fibers or cold-sensitive C fibers also might cause cold hypersensitivity via the abnormal expression or function of sodium, potassium, and calcium channels.1516 The frequency and severity of ‘Sirim’ and ‘Sirim’ pain were not associated with the CDT or QSART results in our study.
In SFN, Aδ and C fibers might be affected differently during the disease course and possibly also according to the etiology.17 Therefore, diverse individual somatosensory profiles could exist that reflect pathophysiological mechanisms.18 Our study found that an abnormal CDT in the setting of normal QSART findings was associated with more-severe stabbing pain of a spontaneous paroxysmal nature, whereas abnormal QSART findings were not associated with neuropathic pain symptoms. Because Aδ-fiber-mediated pain is usually described as sharp pain of short duration, dysfunctional Aδ fibers—reflected by decreased CDT—might contribute to the severity of stabbing pain. Studies of patients with polyneuropathy have found a positive correlation between deteriorated thermal thresholds and pain intensity.1920 However, the lack of reports on the correlation between specific neuropathic pain symptoms and single QST parameters means that these findings need to be confirmed.
We adopted QSART as one of diagnostic tools, and 24% of the patients were included due to their QSART findings being abnormal. QSART may have complementary roles in addition to QST (CDT and WDT) and skin biopsy considering the different major neural substrates of the test.2 Small fibers consist of thinly myelinated Aδ fibers that transmit sharp pain and cold impulses, and unmyelinated C fibers that transmit slow pain sensations such as burning pain, warm sensation, and postganglionic autonomic information. Therefore, CDT, WDT, and QSART can evaluate the functioning of Aδ fibers, somatic C fibers, and autonomic C fibers, respectively. A skin biopsy detects the number of intraepidermal nerve fibers, mostly somatic C fibers. Previous studies have found that somatic and autonomic evaluations are independent in the diagnosis of SFN and recommended that concurrent assessments be performed.2122 Adding QSART to existing SFN criteria that include clinical findings, QST, and skin biopsy was found to increase the diagnostic yield from 38% to 66%.22
Probable underlying causes were not found in most (65%) of the patients in this study even after performing extensive investigations, with the exception of genetic testing for sodium-channel mutations. However, the prevalence rates of idiopathic causes in patients with SFN were also found to be high (≥50%) in other studies.3 Longitudinal assessment and follow-up might be needed to properly identify the cause in individual patients. Patients with a probable etiology tended to experience burning feet and ‘Sirim’ more frequently and more-severe tingling sensation, brush-evoked pain, and ‘Sirim’ pain compared to those with unidentified causes. However, there was no significant difference in their QOL. Restless-leg symptoms and pressure-evoked pain were associated with decreased physical aspects of QOL, explaining about 67% of the physical QOL scores. Another study found that changed sweating pattern, dry eye, and total VAS scores were independent predictors of the PCS in SFN patients, but these predictors only explained 32% of the decrease in QOL.23
This study was subject to several limitations. First, the intraepidermal nerve fiber density—which reportedly has the highest sensitivity and specificity in diagnosing SFN—was not evaluated. Second, clinical signs favoring small-fiber dysfunction, such as pinprick and thermal sensory loss, were not investigated in most patients. Third, genetic tests for sodium-channel mutations were not performed in the etiology workup. Further studies are warranted to determine ethnicity differences in SFN symptoms including cold pain, and to identify the types of impairment of small somatic and autonomic nerve fibers (e.g., nerve density or morphometry) associated with small-fiber damage.



 XML Download
XML Download