

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The gait impairment in patients with Parkinson's disease (PD) is characterized by increases in the stride-to-stride variability in the stride length and stride time of the gait along with reductions in the gait speed, stride length, and step width.123 Many studies of gait analysis in PD have focused on the usual or comfortable walking in a forward direction, perhaps because forward gait (FG) is the most common and important type of gait in humans regardless of the presence of PD. Among the few studies that have investigated the dynamics of backward gait (BG) in patients with PD, Hackney and Earhart4 found that BG is more impaired than FG in patients with PD, and Bryant et al.5 reported that BG was improved similarly to FG after levodopa administration. Conversely, the dual-task gait (DG), such as walking while performing a cognitive task, has been extensively investigated in patients with PD in the context of cognitive impairment. Compared with the single-task gait, patients with PD performing DG exhibit more-severe deficits in gait speed, stride length, gait asymmetry, and stride-to-stride variability.6 Moreover, DG was more impaired in PD patients who exhibit the freezing of gait, which is considered to be associated with a high risk of falling.78
Most gait studies have investigated patients in the advanced stages of PD rather than the early stages of PD, because alterations of gait parameters are closely related to the progression of motor symptoms in PD patients. This focus has resulted in a dearth of information on the characteristics of gait dynamics in early-stage PD. However, some researchers have reported that even patients with de novo PD exhibited a slow gait with reductions in stride length and stride time.910 Our group recently showed that the slow gait in patients with de novo PD was related to a reduction in the stride length rather than the stride time; furthermore, after levodopa administration, their slow gait was improved by increasing the walking cadence; that is, shortening the stride time rather than increasing the stride length.11
In the present study we aimed to determine the type of gait (FG, BG, or DG) that is most strongly associated with pathophysiological changes reflecting motor symptoms or the risk of falling in patients with de novo PD. We hypothesized that DG is more closely related to motor symptoms and the risk of falling in PD patients because mild cognitive impairment is not uncommon in the early stages of PD,1213 and such cognitive difficulties could exert a greater impact on DG in patients with de novo PD.14 However, it was found that the results did not fully support this hypothesis.
METHODS
Participants
Drug-naïve patients with a clinical diagnosis of de novo PD15 and healthy controls were recruited prospectively from the Parkinson's Disease Center of Korea University Guro Hospital between 2014 and 2015. Patients who had PD for shorter than 5 years and were 50–75 years old participated in the study. Subjects who found it difficult to properly perform various gaits during the analysis were excluded, and hence none of the included subjects had any significant musculoskeletal condition or comorbidity of neurological disorder including dementia or vestibulopathy. In addition, to minimize the possibility of atypical parkinsonism, we excluded any PD patient with poor levodopa responsiveness after a levodopa trial, defined as an improvement in motor symptoms of less than 20% at 1 hour after receiving levodopa.16
After obtaining informed consents, initially 30 patients with PD and 30 age- and sex-matched healthy subjects were recruited. After applying the exclusion criteria, 24 patients with PD and 27 controls were included in the final analysis. The present study had a prospective design and was approved by the Institutional Review Board of Korea University Guro Hospital (IRB No. KUGH13034). A subset of the data reported here has been published previously.11
Clinical assessments
Clinical PD was diagnosed in all patients by a single movement-disorder specialist (S.-B.K.). All of the participants (both the PD patients and controls) were assessed by another movement disorder specialist (K.-Y.K.) applying the inclusion and exclusion criteria for subjects in the study. Clinical demographics and scores on the Korean version of the Montreal Cognitive Assessment were measured. The fear of falling was evaluated using the Fear of Falling Measure (FFM) with permission from the authors, for which the maximum score is 38.17 In addition to the Unified Parkinson's Disease Rating Scale (UPDRS) Part II, patients with PD were evaluated using UPDRS Part III (motor symptoms) at baseline and 1 hour after administering levodopa/carbidopa (100 mg/25 mg). The subscore for motor symptoms was derived as follows: the tremor score was calculated as the sum of UPDRS Part III items 3–9; the rigidity score was calculated as the sum of UPDRS Part III items 10–14; the bradykinesia score was calculated as the sum of UPDRS Part III items 15–22 and 27; and the postural instability and gait difficulty (PIGD) score was calculated as the sum of UPDRS Part II items 13–15 and UPDRS Part III items 25 and 26.
Gait studies were performed using the GAITRite system (CIR Systems Inc., Franklin, NJ, USA) with a 4.6-m-long walkway mat. FG, BG, and DG (which involved walking while subtracting serial 7s) were randomly assessed in each patient in order to minimize possible learning effects. Each of the three gaits was tested 10 times while walking at a comfortable speed. Participants were asked to start two steps before the mat and stop two steps after the mat in order to avoid acceleration and deceleration effects. The following spatiotemporal gait parameters were measured: speed (cm/s), cadence (steps/min), stride time (s), stride length (cm), swing phase (%), double-support phase (%), and step width (cm). The following gait parameters were also calculated: coefficient of variation (defined as 100×SD/mean) of any given variable, and the gait asymmetric index [defined as 100/ln (short-swing time/long-swing time)]. The parkinsonian motor symptoms and FG, BG, and DG parameters were only analyzed at baseline (before levodopa administration), although evaluation of motor symptoms and gait tests were also conducted after levodopa administration.
Statistics
Comparisons between the PD patients and controls were performed using Student's t-test. Spearman's rank correlation was used for correlation analyses. A p value of <0.05 was considered statistically significant. Statistical analyses were conducted using SPSS (version 20.0, IBM Corp., Armonk, NY, USA).
RESULTS
Between-group comparisons of FG, BG, and DG
Between-group comparisons of FG, BG, and DG The clinical characteristics of the study participants are listed in Table 1. The follow-up period of the PD patients was 4.09±1.03 years (mean±SD), and the condition of all of them had altered since the initial diagnosis of PD. There were no significant differences in their baseline demographics, with only the FFM score being lower in patients with PD than in the normal controls (p=0.002). Table 2 presents the spatiotemporal, gait variability, and gait asymmetry-associated parameters for the three gaits (FG, BG, and DG) in the healthy controls and the patients with de novo PD. Compared with controls, patients with de novo PD showed a slower gait (p=0.014, p=0.001, and p=0.004 in FG, BG, and DG, respectively), a shorter stride (p=0.001, p<0.001, and p<0.001), and an increased double-support phase (p=0.028, p=0.049, and p=0.003) in all three gaits. However, compared with the controls, the patients with de novo PD exhibited different results regarding the variabilities in stride time and stride length among the three gaits (Fig. 1). BG revealed both increased variability in both stride time (p=0.024) and stride length (p<0.001). DG revealed only altered stride-length variability (p=0.044), and between-group differences in stride-time and stride-length variability were not observed for FG. In addition, there were no between-group differences in any parameters associated with gait asymmetry.
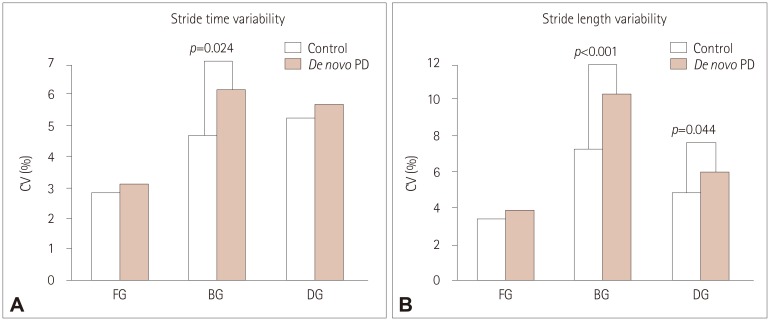
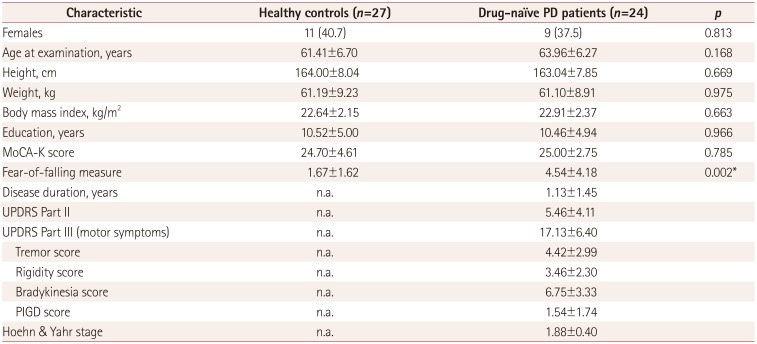
Fig. 1
Stride-to-stride variability in stride time (A) and stride length (B) in FG, BG, and DG in patients with de novo PD and healthy controls. BG: backward gait, CV: coefficient of variation, DG: dual-task gait, FG: forward gait, PD: Parkinson's disease.
![]()
Table 1
Demographic and clinical characteristics of the participants
Data are n (%) or mean±SD values. Modified from the original version of Kwon et al. Gait Posture 2017;58:1–6.11
*p<0.05.
MoCA-K: Korean version of the Montreal Cognitive Assessment, n.a.: not applicable, PD: Parkinson's disease, PIGD: postural instability and gait difficulty, UPDRS: Unified Parkinson's Disease Rating Scale.
![]()
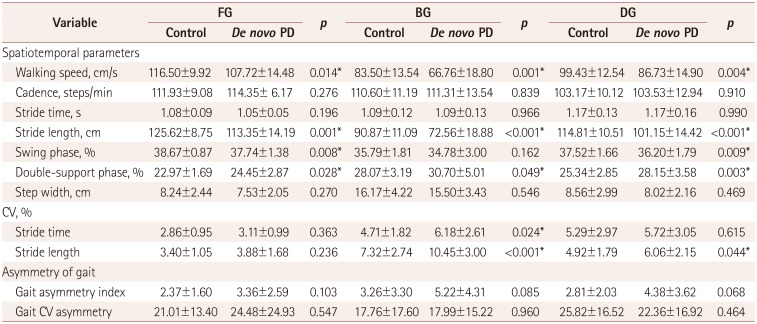
As a post-hoc analysis, comparisons between gait tasks (FG vs. BG vs. DG) in the same group were evaluated (Supplementary Tables 1 and 2 (in the online-only Data Supplement) for healthy controls and patients with de novo PD, respectively). Most of the gait-task parameters differed significantly not only in the control group but also in the PD group. The findings of the within-group comparisons were similar in all groups.
Correlations between FG, BG, and DG speeds and motor symptoms in patients with de novo PD
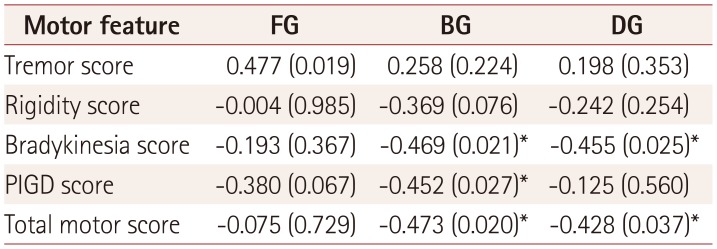
We investigated whether gait speed in each gait condition was correlated with motor symptoms in patients with de novo PD. The results in Table 3 indicate that the BG speed was negatively correlated with bradykinesia score (rs=−0.469, p=0.021), PIGD score (rs=−0.452, p=0.027), and total motor score (rs=−0.473, p=0.020). Whereas, the DG speed was negatively correlated with the bradykinesia score (rs=−0.455, p=0.025) and the total motor score (rs=−0.428, p=0.037). Unexpectedly, the tremor score was positively correlated with the FG speed (rs=0.477, p=0.019).
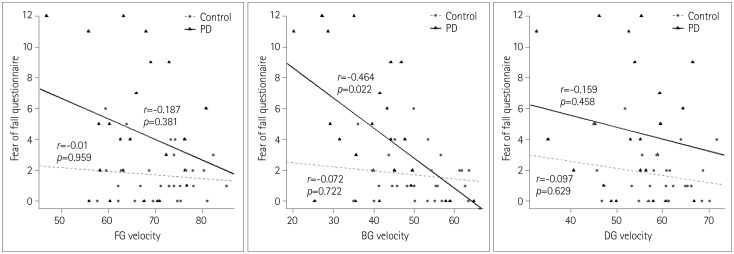
Associations of fear of falling with FG, BG, and DG parameters in controls and patients with de novo PD
The fear of falling is a risk factor for falling in patients with PD,1819 and so we investigated the correlation between gait speed and FFM score (Fig. 2). Notably, the FFM score in patients with de novo PD was negatively correlated with the BG speed but not with the FG or DG speed. Conversely, no correlation between FFM score and gait speed was observed in the control group for all three gaits.
DISCUSSION
To the best of our knowledge, this is the first study to investigate the differences in gait parameters among three gaits (FG, BG, and DG) between patients with PD and normal controls. This study investigated drug-naïve patients with de novo PD to determine the earliest association between motor symptoms and gait dynamics based on gait. Furthermore, we assessed the correlations between gait speed and FFM score in patients with de novo PD and in healthy controls. The obtained results will help to improve the understanding of the detailed clinical relationship between gait parameters among FG, BG, and DG and motor symptoms or fear of falling in the early stages of PD.
The patients in this study with de novo PD showed a slower gait and shorter stride in FG, BG, and DG compared with normal controls. However, the stride-to-stride gait variability results differed among the three gaits (Table 2, Fig. 1): compared with the healthy controls, the patients with de novo PD showed no difference in the variabilities of stride length and stride time in FG, an increased variability in both stride length and stride time in BG, and an increased variability in stride length in DG. These results indicate that slow walking with a short stride is a clear feature of de novo PD regardless of the gait task being performed, and the earliest alterations of gait variability may first become apparent in BG, followed by DG and then FG.
The exact reason why the stride-to-stride variability is more impaired in BG than in FG or DG in patients with de novo PD remains unclear. The stride-to-stride variability of BG in patients with PD has not been fully investigated, although one study found no significant differences between patients in advanced stages of PD and controls.4 Accordingly, further well-designed studies of stride-to-stride variability in different gait types (including BG) need to be performed in patients with PD to determine the clinical relevance or pathomechanisms of disease progression. Conversely, in agreement with the results obtained in the present study, the stride-to-stride variability of DG has been reported to be greater than FG in patients with PD with a moderate disease severity.20 In addition, although asymmetric limb symptoms are a key feature of PD, the degree of gait asymmetry was not altered in any of the gaits in patients with de novo PD compared with normal controls in the present study, which implies that gait asymmetry is a relatively late change in the gait dynamics.
Various factors (including motor symptoms) can affect the gait speed in patients with PD. We investigated whether parkinsonian motor symptoms were correlated with the walking speed in FG, BG, and DG. As indicated in Table 3, the BG speed was associated with a wider range of motor symptoms. Notably, the BG speed was negatively correlated with PIGD score in patients with de novo PD. Our findings indicate that the BG speed is a potential surrogate marker for the progression of motor symptoms or gait impairment in PD. Since there has been relatively few studies of BG in PD, the exact reason for the BG speed being mostly closely related to motor symptoms in patients with de novo PD remains unclear. The basal ganglia are known to function primarily to control and regulate voluntary movements more smoothly. FG could be influenced by visual information, and DG might be affected by the degree of cognitive impairment. BG might be the simplest type of gait among the three gait tasks. In other words, BG might be more closely linked to the function of the basal ganglia in relation to the locomotor system compared to FG or DG. It is therefore reasonable to infer that BG reflects the primary function of the basal ganglia better than does FG or DG, especially in the early stages of PD. Conversely, the tremor score was positively correlated with the FG speed in patients with de novo PD. This result does not imply that tremor accelerated the walking speed, but that patients with less tremor might belong to the non-tremor-dominant or PIGD type, thereby indicating that non-tremor-dominant PD patients exhibited a slower gait than tremor-dominant PD patients. Similarly, several other studies have found that the reductions in gait speed were more pronounced in non-tremor-dominant PD patients than in tremor-dominant PD patients.112122
The risk factors for falling in patients with PD include a previous history of falls, disease duration, disease severity, dyskinesia, freezing of gait, stride-time variability, fear of falling, and postural instability.23242526 Falls can occasionally occur even in the early stages of PD, which has prompted several researchers to investigate the risk of falling in early-stage PD, including the de novo state.272829 However, those studies have not produced consistent results. Moreover, meaningful comparisons of the fall history between controls and patients with de novo PD could not be performed in the present study since the number of participants with a history of a recent fall was very small in both groups (data not shown). Instead, the fear of falling was correlated with the BG speed, but not the FG or DG speed in patients with de novo PD; however, a similar association was not found for any of the three gaits in healthy normal controls (Fig. 2). Lord et al.27 recently reported that a slower gait was an independent risk factor for falling in de novo PD patients, and Son et al.30 demonstrated that freezing of gait in patients with PD was associated with slower walking in BG than in FG. Together these findings indicate that the BG speed is more strongly associated with the risk of falling than are the FG or DG speed in the early stages of PD. Future studies should investigate the relationship between the BG speed and falls in patients with PD.
This study was subject to several limitations. First, it was conducted in a single hospital and included a relatively small number of participants, and so the findings should be interpreted with caution. Nevertheless, significant results could be obtained since it was a prospectively designed case-control study. Second, the measurements using the GAITRite system for evaluating each gait did not accurately represent real walking conditions. However, several efforts were made not only to reduce the learning effect, but also to minimize the effects of acceleration and deceleration on the gait, as described in the Methods.
In summary, patients with de novo PD exhibited a slower gait and shorter stride in FG, BG, and DG compared with normal controls. However, the stride-to-stride gait variability was more impaired in BG than in FG or DG. Furthermore, the BG speed was more closely related to motor symptoms and fear of falling than were the FG and DG speeds in patients with de novo PD. Our findings suggest that more clinically relevant studies of BG are required in patients with PD.
 XML Download
XML Download