

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Natalizumab is one of the most effective therapies currently available for multiple sclerosis (MS), but it carries the risk of the life-threatening condition of progressive multifocal leukoencephalopathy (PML) caused by the John Cunningham virus (JCV). Substantial efforts have been made over the past decade to identify risk factors for PML development, as well as to establish guidelines for drug surveillance and PML diagnosis and monitoring. Prior use of immunosuppressants, longer treatment duration (especially >2 years), and the presence of anti-JCV antibodies are known to be correlated with an increased risk of developing PML in natalizumab-treated patients.1 The quantitative antibody level (as assessed by the anti-JCV-antibody index) in natalizumab-treated anti-JCV-positive MS patients with no prior immunosuppressant use was recently shown to further indicate the PML risk in individual patients.2 It has been suggested that patients with an anti-JCV-antibody index >1.5 have an increased risk of the subsequent development of PML during natalizumab treatment.2 Data on natalizumab-treated patients pooled from large, open-label studies revealed that about 58% of patients were JCV seropositive3 and that 22–45% of patients in European countries had an index >1.5.45678
There is little information on the seroprevalence of JCV in Asian countries, with especially few reports based on the validated second-generation enzyme-linked immunosorbent assay (ELISA)9 that has been demonstrated to accurately stratify patients according to their risk of PML. In 2014 we reported a rate of 69% for anti-JCV antibodies in 78 patients with neuromyelitis optica spectrum disorder (NMOSD), which was higher than the published rates for MS cohorts in Western countries, suggesting that the rate of JCV seroprevalence is higher in Asian than Western countries.10 Consistent with this hypothesis, a high seroprevalence of anti-JCV antibodies (80%) and a high proportion of patients with an index >1.5 (62% of patients) was reported in Chinese patients with MS.11 It was recently suggested that the JCV-antibody seroprevalence in patients with NMOSD (81% of 52 patients) is higher than that in patients with MS (70% of 105 patients) in Japan, although this difference was not statistically significant.1213
Together the available data indicate that Northeast Asian patients with MS and NMOSD may have higher anti-JCV-antibody-positivity rates and indices than Western cohorts. Considering the increased risk of PML in patients with anti-JCV-antibody positivity, especially those with a high index (>1.5) after 2 years of natalizumab treatment, neurologists in Asia might be concerned about the risk of PML and hence be reluctant to prescribe natalizumab for patients with MS. Therefore, more data on the seroprevalence and longitudinal evolution of the index of anti-JCV antibodies and its association with the risk of PML in Asian patients are required. In the present study we therefore investigated the seroprevalence of the anti-JCV antibodies and the longitudinal evolution of the anti-JCV indices in a large cohort of Korean MS patients.
METHODS
Patients and samples
This study analyzed patients with clinically isolated syndrome (CIS) or MS according to the 2005 McDonald criteria14 or the 2010 McDonald criteria15 who were seen at the MS Center of the National Cancer Center, Goyang, Korea between December 2006 and June 2018. Blood samples were obtained via peripheral venous puncture during routine clinical visits for clinical diagnostics or safety monitoring. Longitudinal blood samples were available from 66 patients over a median of 4 years. Serum was isolated from blood by centrifugation, and all samples were stored at −80℃. All samples were shipped from Korea to Unilabs (Copenhagen, Denmark), where they were analyzed at the same time in 2018. Demographic data (sex and age) and clinical data [disease duration, prior and current immunomodulatory or immunosuppressive treatment, and Expanded Disability Status Scale (EDSS) score] were collected. This study was approved by the ethics committee of the National Cancer Center (approval no. NCC 2019-0043).
Anti-JCV-antibody assay
The anti-JCV-antibody serostatus and index were determined by two-step ELISA (STRATIFY JCV DxSelect, Focus Diagnostics, Cypress, CA, USA) as detailed previously.29 Index values <0.20, 0.20–0.40, and >0.40 are regarded as JCV seronegativity, indeterminate JCV seronegativity (which requires further testing), and JCV seropositivity, respectively. In the confirmation test, preinhibited and noninhibited aliquots of patient sera are tested. The results of the confirmation assay are reported as the percentage inhibition, calculated as 100×{1−[(optical density of preinhibited)/(optical density of noninhibited sample)]}. Samples are generally scored as positive when the percentage inhibition is >45%. Anti-JCV-antibody indices were categorized into low (>0.9), moderate (>0.9 and ≤1.5), and high (>1.5) in accordance with the criteria used in a previous study of the stratification of PML risk.2
Statistical analysis
This cross-sectional study assessed the association of demographic and clinical variables with the seroprevalence and index of anti-JCV antibodies in the first sample obtained from every patient. Continuous variables are presented as mean±standard-deviation values or median and interquartile-range (IQR) values, while categorical variables are presented as frequencies and percentages. Comparisons between seropositive and seronegative groups were performed using the Mann-Whitney U-test for quantitative variables that did not conform to a normal distribution, and the chi-square test or Fisher's exact test for categorical variables. Differences with a p value <0.05 were considered statistically significant.
RESULTS
There were 355 anti-JCV-antibody results available from 187 patients with CIS or MS. To access longitudinal changes in anti-JCV-antibody indices, a subset of samples from 66 patients were tested annually, resulting in 233 assessments for the entire cohort. The age at the time of obtaining the first sample was 34±10 years, and the median disease duration at that time was 1 year (IQR, 0–5 years). None of the patients developed PML during a median disease duration of 8 years (IQR, 4–12 years).
Demographic and clinical data of the patients are provided in Table 1. The rate of seropositivity in the first sample obtained from each patient in the total cohort was 80% (n=149). The seroprevalence did not differ significantly between the sexes (86% for males and 76% for females, p=0.599). The seropositivity rates stratified by age quintiles were as follows: <21 years, 93%; 21–30 years, 79%; 31–40 years, 82%; 41–50 years, 76%; and >50 years, 83%. In anti-JCV-antibody-positive patients, the median anti-JCV-antibody index was 3.27 (IQR, 1.52–4.18) (Fig. 1A): 4% of them had indices <0.4 (n=6), 11% had indices between 0.4 and 0.9 (n=17), 8% had indices between 0.9 and 1.5 (n=12), and 77% had indices above 1.5 (n=114). It is especially notable that 83 (56%) of the anti-JCV-antibody-positive patients showed extremely high anti-JCV-antibody indices (>3). No significant differences were found in age when the first sample was obtained, sex ratio, disease duration, EDSS score, or use of treatment between patients who were positive and negative for anti-JCV antibodies (Supplementary Table 1 in the online-only Data Supplement). The index did not increase with age in the seropositive patients (Fig. 1B).
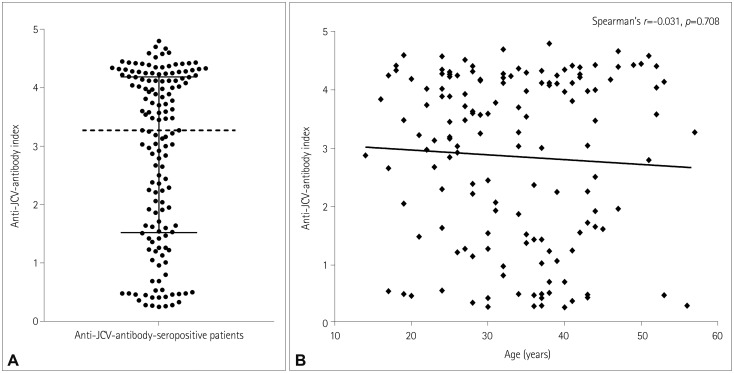
Fig. 1
Anti-JCV antibody index level in patients with multiple sclerosis. A: Anti-JCV-antibody index at baseline in seropositive patients. Dashed line and horizontal bars indicate the median and interquartile-range values, respectively. B: Anti-JCV-antibody index of seropositive patients with multiple sclerosis. The indices of anti-JCV-antibody-positive patients did not increase with age. JCV: John-Cunningham virus.
![]()
A median of 3 (range, 2–7) samples longitudinally collected over a median of 4 years (range, 1–10 years) were available for each of the 66 patients, of which 53 (80%) were initially anti-JCV-antibody positive, among which 39 (74%) had an anti-JCV index >1.5. The serostatus of 59 (89%) patients did not change during the longitudinal analysis. Patients were treated during the observational period with interferon-beta (n=32), alemtuzumab (n=8), natalizumab (n=5), teriflunomide and alemtuzumab (n=4), interferon-beta and mitoxantrone (n=4), interferon-beta and alemtuzumab (n=3), mitoxantrone (n=3), fingolimod (n=2), interferon-beta and fingolimod (n=2), interferon-beta and dimethyl fumarate (n=2), or dimethyl fumarate and natalizumab (n=1).
Five patients exhibited seroreversion (from seropositive to seronegative) at least once during the follow-up period. All of these patients had low indices near the cutoff of 0.4, with no patients exhibiting seroreversion from an index of >0.9 to seronegativity (Fig. 2). Two of these five patients had again converted from seronegativity to seropositivity at the last follow-up. Of 39 patients with an index >1.5 at baseline, 36 (92%) had maintained a high index (>1.5) at the last follow-up (Fig. 2A). Seroconversion (from seronegative to seropositive) at least once during follow-up period was observed in four patients (including the two patients who exhibited seroreversion followed by reconversion from seronegativity to seropositivity): one of these patients was being treated with alemtuzumab and had an index >1.5, two patients were receiving interferon-beta treatment and had indices between 0.4 and 0.9, and one patient was receiving interferon treatment and had an index <0.4. In addition, three patients who were seropositive but had indices <0.9 at baseline exhibited increases in their antibody index to extremely high values (>3.0) while being treated with interferon-beta (n=1) or alemtuzumab (n=2). Serial anti-JCV-antibody results were available for six patients receiving natalizumab: five were anti-JCV-antibody positive at baseline, with four patients having indices >1.5 and one patient having an index between 0.4 and 0.9. The serostatus had not changed and no significant increase in the anti-JCV index was observed in any of these patients after about 2 years of natalizumab treatment.
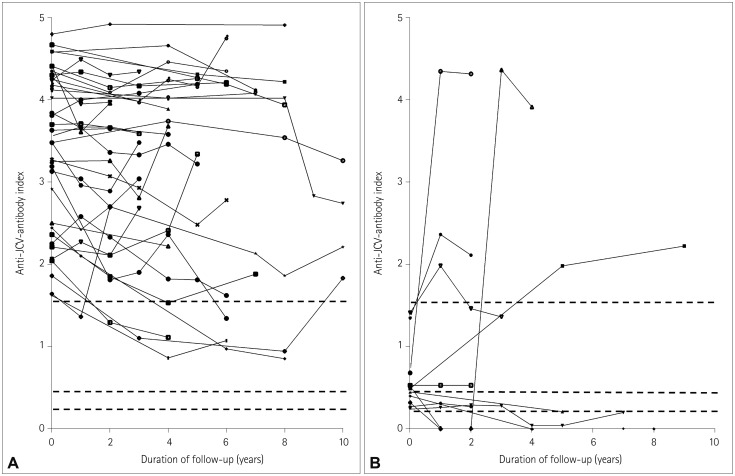
Fig. 2
Serial assessment of anti-JCV-antibody indices of patients who were seropositive at baseline (two to seven JCV serology assessments were performed in each patient). A: Patients with anti-JCV indices >1.5. B: Patients with anti-JCV indices ≤1.5. Horizontal dashed lines indicate indices of 0.2, 0.4, and 1.5. JCV: John-Cunningham virus.
![]()
DISCUSSION
The seroprevalence of anti-JCV antibodies in our cohort (80%) was higher than the overall seroprevalence worldwide (57%) among patients with MS and NMOSD,16 and higher than that found (58%) in large clinical studies of natalizumab-treated MS patients.3 Furthermore, 61% of our total cohort had anti-JCV-antibody indices >1.5, which is much higher than the rates reported for Western cohorts, such as 22% in Germany,8 33% in the UK,7 40% in Spain,5 40% in Portugal,4 and 45% in Austria.6 Previous studies have found that the seropositivity rates are higher in males than in females and increase with age,817 but we did not observe significant differences in serostatus according to sex or age. Consistent with a previous study that found the baseline anti-JCV-antibody index to be highly accurate in predicting a stable positive serostatus,6 we also confirmed the long-term stability of the anti-JCV index in predicting seroprevalence, particularly in patients with indices >0.9.
The high indices (median, 3.27; IQR, 1.52–4.18) observed in seropositive patients and the high proportion of seropositive patients (77%) with anti-JCV-antibody indices >1.5 are especially notable findings of the present study, particularly in the context of the indices used to define STRATIFY JCV DxSelect cutoffs (seronegative, <0.2; intermediate 0.2–0.4; seropositive, >0.4).9 A previous study from the Netherlands found stable high anti-JCV-antibody indices (median, 3.04; range, 2.04–3.59) in all samples obtained from four patients before developing PML, while the median index in natalizumab-treated MS patients who were seropositive at baseline but did not develop PML was 2.105 (range, 0.260–3.941).18 The median anti-JCV-antibody indices of seropositive patients in studies from Austria6 and Finland17 were 2.3 (IQR, 1.1–3.1) and 1.64 (range, 0.26–3.12), respectively, which are much lower than that observed in our seropositive patients.6 However, our results are consistent with a previous study from China finding a median anti-JCV-antibody index of 3.17 (IQR, 0.4–4.1) and 78% of seropositive patients having indices >1.5 (61% of 123 patients with MS).11 Aoyama et al.1213 recently reported a high anti-JCV-antibody seroprevalence in Japanese patients with MS (70%) and NMOSD (81%). The proportions of Japanese seropositive patients with NMOSD and MS with a high anti-JCV-antibody index (>1.5) were 76% and 75%, respectively,1213 which are comparable to our results. Together these data indicate that patients with MS and NMOSD in Northeast Asia appear to have higher seroprevalence rates with higher indices than do Western cohorts.
A previous study suggested that high levels of anti-JCV antibodies in the blood indicate a high risk of PML in patients with no prior immunosuppressant use.2 The risk of PML after 2 years was >1.0 per 1,000 patients with an index >1.5 and no prior immunosuppressant use, and the largest numerical increase in risk occurred after 3 years.2 Therefore, results showing a high proportion (>60%) of patients with high anti-JCV-antibody indices (>1.5) in Asian patients may raise concern about the risk of PML when this population is being treated with natalizumab. Although an anti-JCV-antibody-positive status with an index >1.5 is not a contraindication for natalizumab treatment, more than 60% of Asian patients would reach the highest risk category for PML after 24 months of natalizumab treatment. Given that the highest ever-reached index category should be used to determine the PML risk in individual patients6 and that the upper limit of the assay may limit the ability to track further increases in high indices (>3.0),18 the monitoring of indices during natalizumab treatment becomes less useful when predicting the development of PML in patients with baseline indices >1.5.
The reasons for the anti-JCV-antibody levels being higher in Asian patients than in patients from other geographic regions remain unclear. JCV strains are acquired asymptomatically early in life, probably from exposure within the family or the immediate community, and then persist in renal tissue.1920 The persistent high indices observed in most of our patients over several years probably reflects the periodic release of latent JCV into the periphery from persistently or latently infected lymphoid cells.21 The second-generation ELISA detects serum anti-JCV antibodies specific for JCV-like particles containing VP1 capsid protein. JCV has been classified into several genotypes according to sequence variations within the major capsid protein (VP1) and regulatory protein (T antigen) genes, and these genotypes are linked to populations in specific geographic regions.22 Among the four main genotypes, JCV type 1 predominates in Europe while JCV type 2 predominates in Asia. Although comparative data on the biological properties of the JCV genotypes are lacking, differences in viral loads and variability in VP1 mutations between BK polyomavirus genotypes have been reported.23 In addition, studies of host genetic factors that determine immune responses to the virus have found that human leukocyte antigen are associated with the anti-JCV-antibody response.524 We therefore hypothesize that the interplay of viral and host genetic factors leads to differences in the anti-JCV-antibody seroprevalence and index between Asian and Western countries.
Nevertheless, it remains unclear whether Asian patients are more susceptible to developing PML. Oshima et al.25 recently reported that rates of drug-associated PML in patients with MS appear higher in Japan (2.5%) than in the United States (0.24%), but that the odds ratios for the risk of PML following natalizumab and fingolimod therapy were similar after adjusting for age and sex. The index thresholds are chosen with the aim of keeping false-negative rates low, and likewise the specificity for predicting PML is low, as 57% and 75% of non-PML patients were found to have indices >1.52 and >0.9,26 respectively. Likewise, none of the patients who maintained high indices over several years or who exhibited significant increases in anti-JCV-antibody indices from <0.9 to >3.0 developed PML in our cohort.
JCV exists in at least two forms in an individual host: a latent nonpathogenic form (wild-type JCV) and a virulent neurotropic form (pathogenic JCV).27 Previous studies have shown that JCV mutants from the cerebrospinal fluid of PML patients carry a defined spectrum of mutations in a region of VP1.28 These mutations in pathogenic JCV strains prevent the engagement of sialylated glycans, which are thought to serve as receptors for the infectious entry of wild-type JCV.28 Nevertheless, PML-mutant JCV strains remain infectious via a nonsialylated glycosaminoglycan-receptor-dependent entry pathway.29 Modulation of this glycan-binding specificity of JCV may result in differences in tissue tropism and allow the virus to escape from neutralizing antibodies.29 It was recently reported that most samples from healthy seropositive individuals robustly cross-neutralized all tested JCV variants, whereas samples from PML patients neutralized wild-type JCV strains but failed to neutralize PML-mutant JCV strains.30 Therefore, rather than high antibody titers alone (mostly for wild-type JCV), an increase in the antibody response due to the newly enhanced replication of pathogenic JCV mutants may determine the risk of developing PML.
This study was limited by its retrospective design and by the collection of data from a single center. The number of enrolled MS patients was not large due to the relative rarity of the disease in the Korean population. However, this is the largest study yet undertaken in an Asian country. In addition, we cannot directly compare the seroprevalence of our cohort with those in other cohorts due to differences in patient characteristics. Older age, male sex, and natalizumab treatment have been known to increase the anti-JCV-antibody seroprevalence.781731 However, our cohort was relatively young (mean age of 34 years), its sex ratio was similar to those of other cohorts,45 and none of the patients had a previous history of natalizumab treatment at baseline. Thus, these factors cannot explain the higher anti-JCV-antibody seroprevalence and indices in our cohort compared to the previously reported values for Western cohorts.
This study contributes to the very small amount of literature on anti-JCV-antibody seroprevalence and longitudinal stability of anti-JCV-antibody index in Asian patients. The utility of monitoring the anti-JCV-antibody index during natalizumab treatment seems to be low in the >60% of our patients who exhibited a high anti-JCV-antibody index from baseline. Considering the low specificity of the antibody test for PML prediction, other biomarkers such as the expression of L-selectin on CD4-positive T cells,32 lipid-specific IgM bands in CSF,33 or multiplex PCR for identifying mutant pathogenic JCV34 should be validated in Asian cohorts. Further research is needed to confirm our findings in other Asian countries and to elucidate the mechanism underlying why anti-JCV-antibody responses are stronger in Asian MS patients than in other patients worldwide.
 XML Download
XML Download