

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Migraine is a common neurological disorder that is preceded by an aura in approximately 20–30% of migraine patients.1 Migraine aura (MA) is a phenomenon whose manifestations coincide with a wave of cortical spreading depolarization/depression (CSD) through the cerebral cortex23 and/or even through associative, commissural, and projective fibers of white matter.4 Numerous imaging studies of migraine patients have described multiple changes in the migraineur brain.5678 A few studies have investigated the role of subcortical structures in the pathophysiology of migraine,91011121314 and they revealed decreased volumes of the left caudate, putamen, right nucleus accumbens, and striatum.101214 Moreover, it was found that the basal ganglia play a significant role in the pathophysiology of pain in episodic migraine.9 However, previous studies have not explored the role of subcortical structures in the pathophysiology of migraine with aura (MwA). Also, they did not pay attention to volume and shape abnormalities in distinct subcortical structures in MwA patients. Thus, alterations of the subcortical structures in MwA patients remain insufficiently explored.
The aim of this study was to compare the volumes of subcortical structures between MwA patients and healthy subjects (HS) using advanced structural neuroimaging techniques. We also aimed to determine the correlations between the characteristics of MwA and the volumes of subcortical structures.
Go to : 
METHODS
Participants
Participants were recruited from a registry of the Headache Center at the Neurology Clinic, Clinical Center of Serbia and diagnosed as MwA using third edition of the International Classification of Headache Disorders (ICHD-3) criteria.1 The inclusion criteria were as follows: 1) 21 to 60 years of age, 2) MwA attacks for 2 years or longer, 3) no clear structural pathology or hyperintense white-matter lesions on previous MRI scans, 4) no comorbid basal ganglia disorder or history of other neurological disorders, and 5) not receiving any prophylactic therapy for 1 year prior to the present MRI examination.
Thirty-two HS who had no neurological or metabolic diseases were voluntarily recruited from clinical staff and matched with the included migraineurs in terms of sex and age. The HS had never experienced any type of a headache other than infrequent tension-type headaches, and had no family members who suffered from migraine. All participants were screened and examined by a neurologist (J.Z.T.) to ensure that they met the inclusion/exclusion criteria, and they were all righthanded. All of the MwA patients were asked about the disease onset, the average aura duration, the annual frequency of MwA attacks, and the occurrence of visual, somatosensory, and language disturbances during MA. A questionnaire specifically designed for MA features was used in the study.15
Participants were referred to the Special Hospital for Prevention and Treatment of Cerebrovascular Diseases (SHPTCD) to undergo three-dimensional (3D) T1-weighted (T1W) and T2-weighted (T2W) MRI scans. All participants gave written informed consent and were scanned on the same MRI scanner. The research protocol of this study was approved by the Review Boards of the SHPTCD and the Neurology Clinic (IRB No. 2773/4).
MRI data acquisition
MRI examinations of patients were performed using a 1.5-Tesla MRI scanner with an eight-channel head coil (Signa, General Electric Healthcare, Milwaukee, WI, USA). The imaging protocol consisted of a T2W spin-echo sequence in an axial plane [echo time (TE)=105.8 ms, repetition time (TR)=5700 ms, flip angle (FA)=90 degrees, 24 slices with 0.47×1×5 mm3 voxels, slice thickness=5 mm, acquisition matrix=512×512] and a 3D T1W fast spoiled gradient-echo (FSPGR) series (TE=3.60 ms, TR=8.12 ms, FA=15 degrees, 248 continuous slices with 0.47×0.47×1.4 mm3 voxels, slice thickness=1.4 mm, acquisition matrix=512×512, and field of view=256×256 mm2). Each MwA patient was migraine free for 72 hours prior to the MRI scan and 48 hours thereafter. T2W images were only used to exclude the presence of hyperintense white-matter lesions.
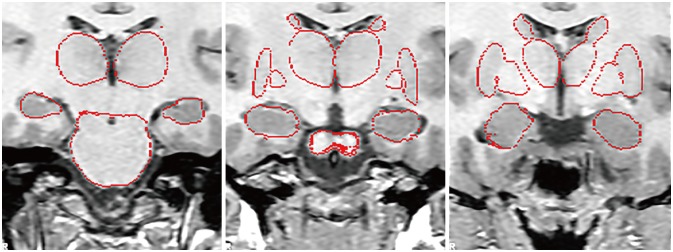
Images were transferred to a PC workstation and converted to Neuroimaging Informatics Technology Initiative (NifTI-1) format using the dcm2nii software (https://people.cas.sc.edu/rorden/mricron/dcm2nii.html). Only T1W FSPGR volumetric images were included in the analysis. In the first step, images were checked for orientation using the fslreorient2std (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/Orientation_Explained) routine in the FSL 5.0 package. The subcortical gray matter was segmented using the model-based FMRIB Image Registration and Segmentation Tool (FIRST) in the FSL 5.0 package. This tool utilizes the principles of active shape and appearance models placed within a Bayesian framework. The models were trained for 15 different subcortical structures using 336 manually segmented and labeled T1W MRI images.16 This method has been successfully implemented in several recent investigations.1718 Voxels were interpolated to 1×1×1 mm3 using the FMRIB Linear Image Registration Tool (FLIRT). The segmentations of subcortical structures were assessed visually. The brainstem was excluded because the shape model used in the FIRST extended beyond the inferior boundary of the images. We also did not investigate the volume of the nucleus accumbens due to its small volume making the measurements unreliable.19 The volume of each of the 12 extracted structures (left and right thalamus, caudate, putamen, GP, hippocampus, and amygdala) was measured in cubic millimeters. The results of subcortical structure segmentation for each subject were carefully reviewed for errors (Fig. 1) by a radiologist (I.P.) and a trained analyst (M.D.). Moreover, the total intracranial volume was computed from the highresolution T1W images of each subject using the fully automated Structural Image Evaluation, using Normalization, of Atrophy (SIENAX) tool in the FSL 5.0 package. Also, shape analysis was performed for subcortical structures that were significantly different while controlling for the effects of age, sex, and total intracranial volume.
Statistical analysis
Subject demographics and MwA characteristics were reported using descriptive statistics and compared amongst the subject groups using the independent-samples t test or chi-squared test as appropriate. The criterion for statistical significance was set at p<0.05.
The data were exported to the R statistics program (https://www.r-project.org/). A general linear model (GLM) analysis was used to investigate differences in the volumes of subcortical structures between the MwA patients and HS while controlling for the effects of age, sex and total brain volume in order to avoid spurious results. Also, the observed power based on the effect size estimated from our data was automatically derived from the GLM analysis. A partial correlation test while controlling for the effects of age, sex and total brain volume was used to assess the correlations between the volumes of subcortical structures and the following characteristics of the MwA patients: aura duration, age at disease onset, disease duration, frequency of MwA attacks, and whether or not language disturbances were present during MA. The results for the GLM and partial correlations were corrected for multiple comparisons using the false-discovery rate with the Bonferroni-Holm correction (p<0.05).
Go to :
RESULTS
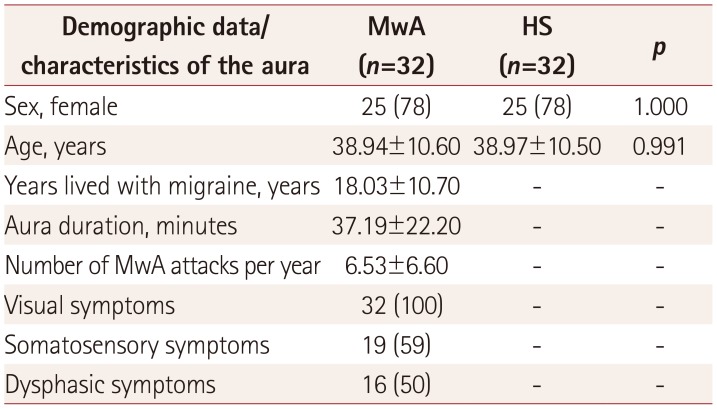
The study included 25 female and 7 male MwA patients who were matched with the same number of HS. The main demographic and clinical characteristics of the included participants are presented in Table 1.
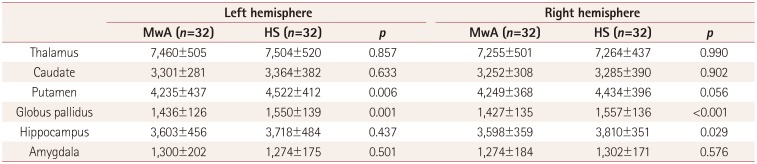
The multivariate GLM had an observed power of 0.965 (p=0.005), indicating that the obtained results were accurate for the sample and generalizable to the population level. After correcting for multiple comparisons, the volumes of the right GP, left GP, and left putamen were significantly smaller in MwA patients than in HS: 1,427±135 mm3 (mean±SD) vs. 1,557±136 mm3 (p<0.001), 1,436±126 mm3 vs. 1,550±139 mm3 (p=0.001), and 4,235±437 mm3 vs. 4,522±412 mm3 (p=0.006), respectively (Table 2). Shape analysis showed statistically significant inward deformations in the right GP, left GP, and left putamen, with maximum differences of −0.53 mm, −0.50 mm, and −0.44 mm, respectively (Fig. 2). We observed no correlations between the volumes of subcortical structures and the occurrence of somatosensory and dysphasic symptoms, MA duration, age at disease onset, disease duration, and frequency of MwA attacks.
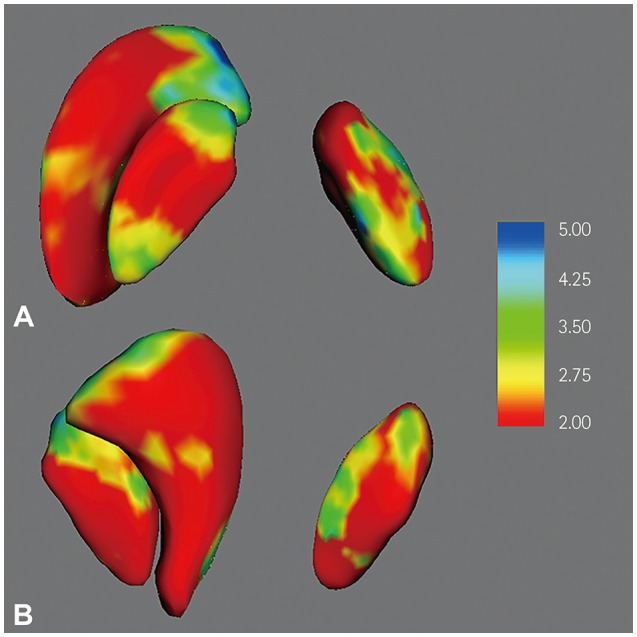 | Fig. 2Three-dimensional visualization of the results of shape analysis of the subcortical structures that were significantly smaller in MwA patients than in healthy subjects. MwA patients showed significant inward deformations of the right globus pallidus, left globus pallidus, and left putamen (A, upper view; B, lower view). Significant inward deformations are quantified on a -log(p) scale, with blue indicating the greatest inward deformations. The results are uncorrected for multiple comparisons, and hence are for illustrative purposes only. MwA: migraine with aura.
|
Go to :
DISCUSSION
This study investigated differences in the volumes of subcortical gray matter structures between MwA patients and HS. Our main finding was that MwA patients exhibit significantly smaller volumes of the globus pallidi and left putamen relative to HS. However, no relationships with clinical parameters were found.
The function and structure of the GP in migraine have been investigated previously,910 but the exact connection with MwA patients was not explored. The present findings suggest that MwA patients have a smaller GP compared to HS that is not demonstrated in the population of migraineurs without aura.10
It is known that GABAergic neurons from the GP externa (GPe) project throughout the subthalamic nucleus, GP internus (GPi), substantia nigra, and striatum. Thus, GPe neurons are positioned to respond to the main basal ganglia pathways and coordinate activity throughout the brain using synaptic inhibition.20 Considering that the GPi forms the final output pathway from the basal ganglia to the cerebral cortex21 and has the ability to modulate cortical excitability and plasticity,22 the role of the GP in the pathophysiology of MA cannot be excluded. Our shape analysis of the globus pallidi revealed that both the GPe and GPi are significantly smaller in MwA patients than in HS. Since the morphological correlate of the reduced volumes of the GPe and GPi is currently unknown, it is even more difficult to speculate on the possible functional effects of these volume reductions. Moreover, the causal directions of the associations between MwA and GP volumes are unclear because of the cross-sectional design of this study. However, a reduced volume of the GP was not detected in patients with migraine without aura10 or in patients with nonmigraine or tension-type headache.14 The role of the basal ganglia in headaches and other pain conditions has not been explored sufficiently. However, the results of our study indicate that alterations in subcortical volumes could not be related to aura symptoms per se. Thus, future studies with longitudinal experimental designs should focus on the role of subcortical volumes in delineating MwA patients and migraineurs without aura.
The left putamen was also found to be smaller in our study. The putamen together with the GP make up the lenticular nucleus, which is highly interconnected with the cerebral cortex, thalamus, and brainstem. A smaller volume of putamen was demonstrated in patients with nonmigraine and tensiontype headaches,14 as well as in other pain conditions such as knee osteoarthritis and lumbar disc herniation.2324 In contrast, a larger volume putamen has been demonstrated in some chronic neuropathic pain conditions,252627 indicating that the effects of pain on the putamen and vice versa are not straightforward. Previously reported alterations in the cerebral cortex of MwA patients2829 together with the observation of lenticular volume differences in our study suggest the involvement of corticolenticular loops in the pathogenesis of MwA. It can be speculated that a smaller putamen could exert excitatory or inhibitory effects on the hyperexcitability of MwA brains. Moreover, we did not find any correlations between the volumes of subcortical structures and the disease duration or frequency of attacks, and so we are inclined to think that the observed changes are a biomarker for the migraineur brain—rather than a consequence of repetitive stimulation—triggered by CSD, which is not exclusively reserved for the cerebral cortex.4 However, significant regional atrophy of the thalamus, putamen, and GP was previously demonstrated in patients with idiopathic generalized epilepsy.3031 It is therefore possible that cumulative stress on the cerebral parenchyma (e.g., from CSD) could lead to the atrophy of the most vulnerable subcortical structures. A longitudinal study is needed to clarify this issue.
The current study had both strengths and limitations. Clear strengths of this study are 1) the inclusion of a relatively large sample of MwA patients, 2) the methodology used for investigating subcortical structures, and 3) the detailed information about MA in our sample that allowed us to investigate the connections between dysphasic symptoms and subcortical structures that have previously been neglected. Limitations of this study include its cross-sectional design, which meant that we could not determine whether the observed differences were a consequence or precondition of migraine. Also, we did not use any scales to measure depression, anxiety, or the pain intensity during a migraine attack, and hence the influences of these aspects on subcortical structures were not assessed. In addition, we did not include patients who had migraine without aura, and so we cannot suggest that the observed changes are specific to MwA. However, a recent study stressed that MwA and migraine without aura should be investigated separately, since they could be distinct disorders.32 Another limitation of this study was the use of a T1W FSPGR sequence—rather than a magnetization-prepared rapid acquisition gradient-echo sequence—with nonisotropic voxels. However, the unreliability of findings stemming from the use of nonisotropic voxels in morphometric studies had not been established. Moreover, the reliability of subcortical measures is extremely high regardless of whether nonisotropic or isotropic imaging parameters are used.33
In summary, we found that both the globus pallidi and left putamen were significantly smaller in MwA patients than in a well-matched group of HS. The importance of this result remains to be determined in future neuroimaging studies addressing the role of the basal ganglia in MwA patients.
Go to :
 XML Download
XML Download