

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Human immunodeficiency virus (HIV) infection has historically been an absolute contraindication to kidney transplantation (KT). Since the introduction of potent combined antiretroviral therapies (cARTs), the survival of HIV-infected kidney transplant recipients has dramatically improved. However, despite the improved survival, the mortality from non–HIV-related events, such as malignancies and chronic diseases including end-stage renal disease (ESRD), has increased [1]. HIV is a chronic and manageable disease in many patients with well-controlled viral replication [2]. Consequently, chronic conditions such as ESRD have become an important concern in HIV treatment. Numerous studies have shown favorable outcomes after KT in HIV-infected patients, with similar patient and graft survival between HIV-positive and HIV-negative recipients [34]. We present two cases with an approximate follow-up of 5 years after KT. To our knowledge, this is the first report of successful KT in HIV-infected recipients living in South Korea. This case report discusses some of the challenges encountered to provide insights into transplantation in HIV-positive recipients. In this paper, we present a detailed report of two cases and provide a short review of the existing literature.
CASE REPORTS
Case 1
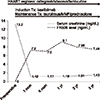
A 37-year-old male patient was identified to have HIV as the underlying disease during a bout of meningitis in 2002. His plasma HIV RNA load was 2,900 copies/mL and his CD4 T-cell count was 387 cells/mm3. No hepatitis B or C coinfection was present. He was started on highly active antiretroviral therapy (HAART) consisting of raltegravir (400 mg, oral, twice a day [BID]), abacavir (600 mg, oral), and lamivudine (150 mg, oral). His renal function rapidly deteriorated to ESRD, which required dialysis to manage the sequelae of meningitis. Subsequently, he underwent living-donor KT with his 60-year-old father as the donor, with whom he shares four histocompatibility leukocyte antigen (HLA) haplotypes. The preoperative panel reactive antibody composition was 0% class I and 0% class II on Luminex (Austin, TX, USA). The pretransplant cross-match test was negative and the recipient was donor-specific antibody negative. The plasma HIV RNA load was always undetectable (<20 copies/mL) and the CD4 T-cell count was ≥200 cells/mm3 during HAART. The patient showed an uneventful early postoperative course without acute rejection, delayed graft function, or surgical complications. Ten days after transplantation, the mean serum creatinine (SCr) level was approximately 1.5 mg/dL, from 11.0 mg/dL before transplantation. Immunosuppression therapy consisting of tacrolimus, mycophenolate mofetil (500 mg, oral, BID), and prednisolone was initiated with an induction therapy with basiliximab. The tacrolimus level was maintained in the range of 5.0–8.0 ng/mL during the follow-up period. The specific HAART regimen remained the same after transplantation, with increased lamivudine dose from 150 to 300 mg after reaching an estimated glomerular filtration rate (eGFR) of >50 mL/min. Except for pneumonia about 2 years after transplantation, no signs of HIV disease progression or opportunistic infections were detected during the follow-up period. Elevated hemoglobin (>19 g/dL) and hematocrit levels were persistently detected after 2 months from transplantation, without thrombocytosis, leukocytosis, or any other potential cause of erythrocytosis. At the same time, the patient complained of malaise, headache and lethargy. An angiotensin II receptor blocker was administered for posttransplant erythrocytosis. At 6.5 years after transplantation, the SCr levels ranged from approximately 1.3 to 1.5 mg/dL (Fig. 1).
Case 2
A 41-year-old man was followed up for chronic glomerulonephritis at our hospital. At that time, laboratory tests revealed a hemoglobin of 10.2 g/dL, blood urea nitrogen level of 49 mg/dL, and SCr level of 7.36 mg/dL. We recommended hemodialysis; however, but the patient refused. Five months later, he visited our emergency department with chest pain. He underwent coronary angiography for unstable angina, which showed 90% stenosis of the proximal left anterior descending artery. Percutaneous transluminal coronary angioplasty was performed using an everolimus-eluting stent. Coronary angiography was followed by temporary hemodialysis with a catheter. HIV infection was detected during the preparation for hemodialysis. The patient's plasma HIV RNA load was 9,400 copies/mL and the CD4 T-cell count was 184 cells/mm3. No hepatitis B or C coinfection was present. HAART with raltegravir (400 mg, oral, BID), abacavir (600 mg, oral), and lamivudine (150 mg, oral) was initiated. About 8 months after hemodialysis, the plasma viral load was <20 copies/mL and CD4 T-cell count was 577 cells/mm3. The patient's 40-year-old sister-in-law, with whom he shares one HLA haplotype offered a kidney for transplantation. The preoperative panel reactive antibody composition was 0% class I and 0% class II on Luminex. The pretransplant cross-match test was negative, and the recipient was donor-specific antibody negative. There was no development of donor-specific antibodies after transplantation. The initial immunosuppressive therapy included tacrolimus, mycophenolate mofetil (500 mg, oral, BID), and prednisolone with basiliximab as the induction therapy. The tacrolimus level was maintained in the range of 5.0–8.0 ng/mL during the follow-up period. The SCr level decreased to 1.1 mg/dL by 2 weeks after transplantation. The specific HAART regimen remained the same posttransplantation, with increased dose of lamivudine from 150 to 300 mg after reaching an eGFR of ≥50 mL/min. At 2 months posttransplantation, the patient visited our hospital with right flank discomfort that had a sudden onset and moderate intensity, with no history of fever, gross hematuria, or trauma. The SCr level increased to 1.85 mg/dL. Physical examination revealed mild tenderness in the right flank. Nonenhanced abdominal computed tomography revealed small-sized hematoma formation around the graft kidney and mild edema. The SCr level continuously increased to 1.97 mg/dL. AS the patient was undergoing antiplatelet therapy, graft biopsy was not performed. Clinical acute rejection was diagnosed, and high-dose steroid pulse therapy was administered for 3 days. One week after pulse therapy, the SCr level decreased to 1.4 mg/dL. At 3.5 years after transplantation, at the last follow-up, the patient was in good condition with excellent renal function (SCr 1.43 mg/dL with minimal proteinuria [0.20 g/L]), plasma HIV viral load <20 copies/mL, and CD4 T-cell count of 421 cells/mm3 (Fig. 2).
DISCUSSION
Since potent cARTs became widely available in 1996, HAART has significantly improved the life expectancy of patients with HIV. Although deaths from acquired immunodeficiency syndrome (AIDS)-defining events have steadily decreased, the mortality from non–AIDS-related infections and ESRD has steadily increased [15]. HIV infection was traditionally considered an absolute contraindication to transplantation because of concerns that immunosuppression would accelerate HIV disease progression. Recent results from prospective multicenter trials on KT in HIV-positive recipient candidates have demonstrated the success and challenges of transplantation in this population. Several studies have reported comparable patient and graft outcomes between HIV-infected and HIV-uninfected recipients after KT in the era of potent cARTs [6789].
KT in HIV-infected recipients is associated with several challenges, including defining the criteria for the inclusion of HIV-infected patients in the transplantation waitlist, drug interactions of potent cARTs under immunosuppression, risk of infection, and the need for coordinated care after transplantation and an infectious disease diagnosis.
The effective evaluation of HIV-infected patients after KT requires continuous coordination between the transplant center and the infectious disease care clinic. HIV-infected patients on KT waitlist must meet the general selection criteria for transplantation in addition to the HIV-specific criteria. Several transplantation groups in Europe and North America are assiduously working to harmonize the criteria for solid organ transplantation [101112]. However, many centers follow the candidate selection criteria established by the National Institutes of Health (NIH) multicenter trials [1314]. The NIH criteria specify that candidates must have an undetectable viral load and a CD4 T-cell count of >200 cells/mm3 and must be on a stable ART regimen for at least 6 months. Ideally, no candidate should have had AIDS-defining diseases. However, opportunistic infections, such as esophageal candidiasis, tuberculosis, and Pneumocystis jirovecii pneumonia, have been withdrawn as exclusion criteria because of the existence of effective treatment and prevention.
The main considerations about ART in a kidney transplant recipient candidate include toxicities and drug interactions. The ideal ART regimen has not been established for HIV-infected patients undergoing KT. However, the ideal therapeutic regimen should aim to achieve and maintain continuous viral suppression and an increased CD4 T-cell count. In addition, renal toxicities and pharmacokinetic interactions with immunosuppressive drugs and their adverse effects can be prevented using low-toxicity regimens and by avoiding pharmacokinetic interactions with calcineurin inhibitors that are metabolized by cytochrome P450 [1516]. Taking these considerations together, in our cases, cARTs were initiated with abacavir and lamivudine as nucleoside/nucleotide reverse transcriptase inhibitors, and raltegravir as an integrase inhibitor. Interactions may be prevented by modifying the cART regimen before transplantation to avoid protease inhibitors in posttransplant drug regimens. Dose-limiting immunosuppressive therapy with calcineurin inhibitors in patients undergoing cART before KT is feasible and can minimize immunosuppressive therapy-related complications in the posttransplantation period [17]. The regimens for induction and maintenance immunosuppression therapies in HIV-infected kidney transplant recipients are similar to those used in HIV-uninfected recipients [1819]. In our cases, immunosuppression therapy comprising tacrolimus, mycophenolate mofetil, and prednisolone was administered along with basiliximab induction therapy.
HIV-infected kidney transplant recipients should receive the same routine monitoring as HIV-uninfected recipients. Regular monitoring of the plasma HIV RNA load and CD4 T-cell count is recommended at 1 month after KT and every 3 months thereafter. In addition, similar to other solid organ transplant recipients, HIV-infected kidney transplant recipients require prophylaxis against the most common posttransplant opportunistic infections, such as P. jirovecii, cytomegalovirus, fungus, and toxoplasmosis.
In conclusion, our cases demonstrate favorable outcomes after KT. Several studies have shown that, with careful patient selection, the patient and graft outcomes in KT are comparable between HIV-infected and HIV-uninfected ESRD patients. KT is now accepted as the standard of care for HIV-infected patients with ESRD. Therefore, HIV-infected patients with ESRD should be referred and evaluated for KT. Our experience illustrates the effective clinical management of HIV-infected recipients undergoing KT.

 XML Download
XML Download