

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
South Korea has a rapidly aging population, and according to the 2019 Organization for Economic Co-operation and Development report, it has the world's highest elderly (over 65) poverty rate (45.7%)[1]. The number of the National Basic Livelihood Security Act recipients is 1,743,690 in South Korea. Among those recipients, the number of elderly is estimated to increase to 32.8%, including 7.1% of the total elderly population, which shows a higher rate compared to other age groups [2]. Moreover, the prevalence of metabolic syndrome is 43.6% among elderly Korean adults and is higher in elderly Korean women, relative to elderly Korean men [3]. Compared to the middle-class senior citizens, the socially vulnerable senior citizens tend to be poorly educated, feel more pressured by medical expenses, and feel socially alienated, which causes low medical-seeking behaviors and higher chance of illness exposure [4].
The increasing rate of metabolic syndrome in socially vulnerable senior citizens is not only a result of nutritional problems, but is also linked to unhealthy food choices driven by socioeconomic factors, nutritional imbalance, micronutrient intake deficits (e.g. of vitamins and minerals), inability to participate in health-promoting behavior and mental stress [5]. According to the 2010 National Nutrition Survey, the elderly population with metabolic syndrome showed higher total energy, protein, and fat consumption compared to those without [6]. It also showed that the average total energy consumption among elderly women is 1,321kcal [7], which is lower than the recommended total intake of 1,600kcal for women over 65 (Ministry of Health and Welfare). The diet of socially vulnerable and obese women was comprised of 69.4% carbohydrates, taking a large portion of the total nutritional intake. They also showed a larger consumption of white rice compared to the general female population [8]. Low intake of calcium and high intake of sodium are two of the major problems causing nutritional imbalances in the Korean population [9]. As for the elderly female population, their low calcium intake is more prominent than in the male population [10].
In the past, obesity and metabolic syndrome prevention programs focused on decreasing the individual's total caloric intake. However, continuous studies on obesity and associated chronic diseases have increased their interest by combining total caloric intake balance and nutrient intake adequacy in their approach [10]. Because metabolic syndrome, including hypertension, diabetes, and hyperlipidemia, must be treated chronically, it is extremely important to fully understand the illnesses and to make lifestyle modifications to control each illness [11].
Furthermore, it has been reported that socially vulnerable elderly women with metabolic syndrome are twice as likely to develop depressive symptoms, compared to the normal population, which has a profound effect on their quality of life [12]. Depressive symptoms tend to increase with age and, depending on the severity of depressive symptoms, one's activities of daily living, cognitive skills, and social support can be affected [13]. These depressive symptoms have negative effects on the successful aging process, and thus social relations work as the elderly's protective factors against depression [13]. Engaging in social contacts, such as meeting someone face-to-face, making phone calls, or writing letters, protects the elderly from social isolation and loneliness [14], and has been found to have higher meaning to socially vulnerable older adults than to other older adults [12]. Studies have shown correlations between social relations and physical and psychological health, which carry more significance in old age [15].
A previous study found that as the structural aspects of one's social network such as size, contact frequency, and scope and qualitative aspects such as financial support and social support, increase, depression among elderly females decreases [16]. Therefore, there is a substantial need for community programs reinforcing social networks among socially vulnerable elderly women with metabolic syndrome. Previous studies on social relations among older adults have focused on finding its relationship with depression, chronic illnesses, physical activity, and health status [13], and they emphasized the need for developing a program for socially vulnerable elderly women with metabolic syndrome.
This study has been based on Baltes and Baltes [17]'s Selection Optimization Compensation (SOC) model, a successful aging theory. The SOC maximizes gains of successful aging [18]. The model assumes that the aging process is associated with changes in forms of adaptation and biological vulnerabilities, a decreased state of general potential and a loss of certain functional abilities. Successful development involves the orchestration of selection, optimization, and compensation which, in turn, regulate the maximization of gains and minimization of losses over time. As individuals age, they choose activities or goals that have personal importance, and use SOC-related behaviors to compensate for what they lack. This process enables one to maintain efficient quality of life and to achieve personal dynamics, which can affect other dimensions [18]. Therefore, this study developed and applied a Self-Care Reinforcement Program (SCRP), considering physical damages, decline in income, depressive mood tendency, and loss of social network in socially vulnerable elderly females, based on the SOC model. The program was designed to promote successful aging by improving physical performance through balanced nutritional intake to protect from metabolic disease risks and to improve socio-psychological function by providing a social network in order to aid recovery from depressive mood.
This study aimed to develop and examine the effects of the SCRP in providing well-balanced nutritional intakes, regular exercise, self-help meetings, and community connection projects for socially vulnerable elderly women with metabolic syndrome.
METHODS
1. Research Design
The current study used a quasi-experimental design, with a pretest/post-test nonequivalent control group, to examine the effects of the SCRP on vulnerable elderly women with metabolic syndrome in Korea.
2. Subjects
This study was conducted on 64 socially vulnerable elderly women aged over 65, receiving the National Basic Livelihood Security Act benefits, falling under 120% of the minimum living cost, and with more than three risk factors for metabolic syndrome. Women with an Korean version of Mini-Mental State Examination (MMSE-K) score of less than 24, diagnosed with stroke or acute myocardial infarction, currently receiving treatment for malignant tumor, and/or involved in any other health-promoting programs were excluded from the study.
The SCRP was conducted three times a week for eight weeks (a total of 24 sessions) with the experimental group. Using G*Power version 3.1.4.[19], we found that 28 participants per group would satisfy an effect size of .80, and that two groups with 85% power were required for onetailed independent t-tests at a significance level of .05. Considering this information, a total sample of 70 participants was deemed appropriate. During the course of the SCRP, six people dropped out, which resulted in a final sample of 33 in the experimental group and 31 in the control group.
3. Measures
1) Body composition analysis
Body composition analysis, including body fat mass, muscle mass, and lean body mass, was measured using InBody 230 (Biospace, Korea), which utilizes bio-electrical impedance.
2) Risk factors of metabolic syndrome
Blood Pressure (BP) was measured using an automatic blood pressure monitor (Baumanometer, USA). Just before their blood pressure was measured, the subjects were asked to stay for at least 10 minutes sitting on a chair. The upper arm was set at the same height as the heart. Blood pressure was measured after placing the lower part of the blood pressure cuff around the upper arm, so as to be positioned 2cm above the brachial artery palpation site. The mean value of blood pressure was obtained by measuring it twice at 5-minute intervals. The waist circumference was measured using a tape measure in the upright posture at the midpoint between the lowest rib and the pelvic iliac crest. In accordance with Asia-Pacific standards, women with waists over 85cm were classified as obese. The subjects, blood test was performed after fasting for more than 12 hours, and was measured with a drop of blood (5µL) using a Cholesterol Meter (Lipid Pro, Korea) in a capillary blood vessel of the finger. This measurement took from 12 seconds to 3 minutes: 5 seconds on fasting blood sugar (FBS), 2 minutes on high-density lipoprotein cholesterol (HDL-C), and 2 minutes on triglyceride. The instrument recognized the condition of the test paper, and was measured by the code test paper method.
3) Nutrient Intake
The participants in this study were asked to keep a daily food diary with a 24-hour recall, and to record the type and amount of food they had consumed over a period of three days using a retrospective method. Furthermore, nutrient intake evaluation was performed by the Computer Aided Nutrition Analysis Program (CAN Pro) 4.0 (Korean Nutrition Society, Seoul, Korea) professional edition, which was provided by the Korean Nutrition Society. CAN Pro has been programmed by Korean Nutrition Society to have reliable database of Korean food and an easy system of estimating food amounts, so it is widely used in nutrition-related papers.
4) Depressive Symptoms
The Geriatric Depressing Scale-Korean Version (GDS-K), developed by Kee in 1995, was used to assess depressive symptoms among participants [20]. GDS-K is a 30-item dichotomous scale (1=Yes, 0=No) with a total score ranging from 0 to 30. The higher the score, the more severe the depression. At the time of its development, the split-half reliability was 0.78. In this research, the split-half reliability was 0.85.
5) Social Network
This study used the Korean Social Network Scale (KSNS) by Lee et al. [21], a Korean-modified version of Lubben Social Network Scale (LSNS) [22]. The LSNS was originally developed based on the Berkman-Syme Social Network Index. Then, Lee et al. adapted the LSNS to suit the Korean elderly population in 2009[21]. The scale consists of items rating the subject's sense of closeness by counting number of times the subject meets with family, number of family members the subject feels close to, number of friends, and number of times the subject meets with friends. It also includes items asking about the frequency of psychological and physical help received from people with whom the subject has social relationships. The questionnaire contains 10 items rated on a 6-point Likert scale, with scores ranging from 0 to 50, where a higher score means a larger social network. The reliability for the original measure demonstrated a Cronbach's α was .75; in this study, Cronbach's α was .70.
4. Research Procedures
1) SCRP Development
This study was based on Baltes and Baltes [17]'s SOC model, a successful aging theory. The SCRP was based on interviews conducted with socially vulnerable elderly females. Metabolic disease education, nutritional education, physical activities, and social networks were included in the program as advised by the literature review. The SCRP was reviewed by two nursing professors, two nutritionists, and two social workers to investigate validity. The professionals were asked to validate the program in five questions rated on a 4-point Likert scale, which demonstrated a content validity index of .89.
2) Research Assistant Preparation
The research assistants were two nurses who helped with questionnaires and measurements, a physical therapist with 5 years' experience, a nutritionist with 6 years' experience, a social worker with 10 years' experience, and a community nurse with 5 years' experience. The researcher provided two hours of pre-training on the purpose and procedure of the research at the welfare centers, located in Districts S and B.
3) Data collection
Data collection was conducted from August 2015 to October 2015. The research subjects were selected with the cooperation of health-center staff after obtaining permission from the director of the institution at the S and B Health Centers, in D city. The researcher visited the welfare centers located in Districts S and B, explaining the purpose and necessity of this study, and obtained the agency's approval for the progress of the program, research activities, and location provision. The experimental group selected vulnerable elderly women with metabolic syndrome at S Health Center. The control group selected subjects at B Health Center, which had a similar economic and healthcare environment to that of the experimental group, so as to prevent diffusion effects.
A pre-test took place a week prior to the start of the program to measure general characteristics, body composition, nutritional intake, risk factors of metabolic syndrome, depressive symptoms, and social networks. After the SCRP was conducted, the same measurements were taken using the same instruments as a posttest, and the SCRP was then provided to the control group. The data were collected from a total of 64 subjects, excluding 6 people who refused to undergo some of the measurements.
4) Intervention
The SCRP provides health education including metabolic syndrome education and nutritional education, exercise, and social network reinforcement (Table 1). Metabolic syndrome education was provided in the form of a lecture followed by a discussion for 50 minutes/week for 3 weeks. Metabolic syndrome education included setting personal health goals and the researcher providing information about obesity, hypertension, diabetes, and hyperlipidemia (which are all factors for metabolic syndrome), including the definitions, causes, management plans and complications of each illness. Nutritional education was provided for 50 minutes/week for 2 weeks and included consultations and a practical course by nutritionists. The participants were educated on meal plans and effects of nutrition on obesity, hypertension, diabetes, and hyperlipidemia. In the nutrition education, food materials that could be bought in traditional markets were selected, considering the economic level of the vulnerable elderly women. Exercises included progressive strength exercises, endurance exercises, cardiovascular exercises, stretching, and circular exercises using balls, towels and chairs, walks, etc. Each physical activity session was provided for 50 minutes, twice a week for 8 weeks, and included warm-up, main, and wrap-up exercises conducted by a physical therapist. Each physical activity session's exercise intensity, duration, and progression was designed considering the participants' age and maximum exercise capacity. Each session was structured with 5 minutes of warm-up exercise, 40 minutes of main exercise, and 5 minutes of wrap-up exercise. To determine the participants' exercise goal achievement, the self-reported Rating of Perceived Exertion (RPE) was used. To examine social networking among participants, group discussion sessions were held. To reinforce social networking, participants were taught about self-help groups and community welfare services.
5) Ethical Considerations
This study was conducted after receiving the Daegu Catholic University Medical Center IRB approval (IRB No.: CR-15-103-L). The study purpose, method, and expected study effects were explained to the subjects in written and verbal form. To protect the rights of subjects', they were informed about voluntary participation and the possibility to withdraw from the study at any time, and consent forms were collected from the subjects before the start of data collection.
5. Data Analysis
SPSS version 22.0 for Windows was used for data analysis (SPSS, INC., IBM Company, Chicago, IL, USA). Analysis of the honogeneity of these characteristics was performed using χ2 test and Fisher's exact test. All data were reported as means (SD). An independent t-test was used to evaluate significant changes in the dependent variables. Statistical significance levels were set at p<.05.
RESULTS
1. Homogeneity of General Participant Characteristics
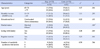
No significant differences were found in general characteristics between the experimental and control groups (Table 2). The homogeneity test showed no differences in age, monthly income, educational level, marital status, living with family, regular exercise, or number of metabolic syndrome risk factors. There were no statistically significant differences in the general characteristics of the participants between the two groups (p>.05).
2. Effect of the SCRP
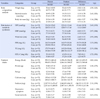
An independent t-test of mean difference (posttest score minus pretest score) showed that the SCRP had significant effects on body composition analysis (skeletal muscle mass (t=2.41, p=.021)), risk factors of metabolic syndrome [SBP
(t=2.40, p=.019), DBP (t=2.97, p=.004), waist circumference (t=2.95, p=.005), FBS (t=3.33, p=.001), TG (t=2.33, p=.024)], nutrient intake [sodium (t=2.11, p=.039)], depressive symptoms (t=4.44, p<.001), and social networks (t=2.63, p=.011) in the experimental group. However, there were no significant differences in body composition analysis [(weight (t=4.58, p=.121), body fat mass (t=1.14, p=.258)], risk factors of metabolic syndrome (HDL-C (t=1.72, p=.091), and nutrient intake [energy (t=0.82, p=.416), protein (t=1.38, p=.173), fat (t=0.93, p=.356), calcium (t=1.02, p=.311)] between the two groups (Table 3).
DISCUSSION
This research aimed to develop and examine the effects of a SCRP, based on Baltes and Baltes [17]'s SOC model, on socially vulnerable elderly women with metabolic syndrome.
Previous nursing intervention programs for patients with metabolic syndrome focused on providing moderate-intensity physical activities, decreasing total caloric intake, and moderating lifestyle patterns [23]. However, the SCRP included a social network reinforcement program to consider socially vulnerable elderly women's underlying reasons for poor well-being, and included strategies to strengthen their understanding of metabolic syndrome to maintain proper self-care. This study aimed to provide a basis for socially vulnerable elderly women to choose appropriate health behaviors to achieve successful aging process. After the SCRP, the experimental group showed improvement in systolic blood pressure, diastolic blood pressure, waist circumference, fasting blood sugar level, and triglyceride level, compared to the control group. Systolic blood pressure and triglyceride level dropped to 122 mmHg and 145 mg/dL, respectively, on average after the SCRP, which can be interpreted as a significant improvement according to NCEP-ATP III's metabolic syndrome diagnosing standards. Waist circumference measurement is directly related to abdominal obesity; therefore, it is used commonly to diagnose risk factors for metabolic syndrome [24]. Abdominal obesity causes a rise in triglycerides, such as leptin and resistin, in visceral fat, the hardening of arteries, and the increase in blood pressure and blood lipid level by secreting substances that decrease insulin sensitivity [25].
Therefore, an improvement in abdominal obesity has positive effects, not only on obesity itself, but also on hypertriglyceridemia, hypertension, high-density lipoprotein cholesterol level, and uncontrolled blood glucose level, which emphasizes the importance of abdominal obesity prevention when providing nursing interventions [25]. The SCRP showed a decrease in waist circumference size as well as in FBS, BP, and TG levels. However, the SCRP did not show any significant changes in high-density lipoprotein cholesterol level. This may be because the NCEPATP III recommends the duration of interventions provided to subjects with metabolic syndrome to be at least 6 months. Therefore, running the SCRP intervention for a longer period of time is suggested in future.
After the SCRP intervention, there was a significant change in sodium intake level. Increased sodium intake results in increased blood pressure, and cardiovascular illnesses such as myocardial infarction, stroke, and congestive heart failure [26]. Our findings are consistent with those of Jung et al. [26], who provided an 8-week nutritional education for borderline hypertensive subjects; this showed significantly decreased sodium consumption and decreased blood pressure. Among nutrient-intake behaviors, no significant results were found in total caloric, protein, fat, and calcium intakes. However, this may be related to the characteristics of the socially vulnerable elderly women. Most previous studies [23] have focused on body weight loss and decreased total caloric intake but, considering our study's population, the study subjects were more prone to physical health problems arising from nutritional imbalance [5]. The pretest showed that the subjects' average total caloric, protein, fat, and calcium intake levels were all lower than the Korean Nutrition Society's recommended amount [27]. Yang and Bang [28]'s study on low-income older adults also showed severe nutritional imbalance, proposing that low-income older adults residing in cities may be a nutritionally vulnerable social group. According to the pretest, the subjects' meals usually consisted of a simple meal of kimchi and white rice, which matches the average food intake patterns of socially vulnerable female population group in South Korea [8], may be the reason for their excessive intake of sodium. Although it may not have been statistically significant, the subjects showed total caloric, protein, fat, and calcium intakes closer to the recommended intake level after the intervention program. This shows that there had been a positive change in meal planning and health promotion.
According to the National Nutrition Survey in Korea, the elderly population with metabolic syndrome showed higher total energy, protein, and fat consumption compared to a healthy population [6]. It also showed that the average total energy consumption among elderly women was 1,321 Kcal [7], which was lower than the recommended total intake of 1,600 Kcal for women over 65 [27]. Socially vulnerable and obese women's diet was comprised of 69.4% carbohydrates, making up a large portion of their total nutritional intake. They also showed larger consumption of white rice compared to the general female population [8]. Low intake of calcium and high intake of sodium are two of the major problems causing nutritional imbalances in the Korean population [9]. These nutritional imbalances have a high influence on obesity, metabolic illnesses, and cardiovascular diseases, and act as a risk factor for health inequality. Previous studies mostly used nutritional and physical activity interventions for subjects with metabolic syndrome [27]. Nutritional interventions are known to have positive effects by increasing insulin sensitivity for unsaturated fatty acids and complex carbohydrates [25].
Physical activity interventions differ depending on types of exercise (cardiovascular, resistance, or strength exercises). However, it has been shown that daily 30-minute moderate-intensity exercise increases muscular density and fat oxidation, resulting in lowering metabolic syndrome risks by improving blood lipid levels, insulin resistance, and blood pressure [25]. A combined nutrition and exercise intervention has been shown to have much larger positive effects [29], correlating with the current study's results. A previous study by Kim [11] showed possible correlations between depressive symptoms and metabolic syndrome. Although there is no definitive causal explanation between the two factors, interactive correlations have been reported.
Social networking plays a greater role in socially vulnerable elderly women compared to the home-cared elderly [12]. As the size, frequency, and scope of social network increases, depressive moods in female older adults reportedly decreases [13]. Therefore, in order to decrease depressive symptoms and increase health-promoting behaviors in socially vulnerable elderly women, it is extremely important to foster their social contacts within the community and to decrease their social isolation and loneliness [14].
CONCLUSION
The current study provided a 3-week-long self-care program, and reinforced the subjects' social networking system by providing self-help groups and community resources to the elderly women. After the SCRP intervention, the subjects' social network score significantly increased. This may be due to the increased frequency of meeting with neighbors and interacting with them through the social network reinforcement strategy. Therefore, social networking should be taken into consideration as a modification factor when providing care for a socially vulnerable population. The SCRP has resulted in positive effects on physical and psychological factors by decreasing the risk factors for metabolic syndrome, and by helping to maintain nutritional balance and reinforce the social networking system.
This study has verified that the SCRP intervention can have positive effects on socially vulnerable elderly women by lowering the risk factors for metabolic syndrome. It also has a significant meaning to nursing intervention programs based on the SOC model. Based on these findings, further studies are suggested to include various population groups, and further research is needed to validate the long-term effect of the SCRP. This study has some limitations. The intervention collectively provided education, exercise, and social networking, which makes it difficult to clearly analyze the causal relationships between each of these factors. Also, the intervention was provided only for 8 weeks, which may be too short to have an effect on nutritional intake patterns, because the NCEP-ATP III recommends 6-month-long interventions. Subjects using the 24-hour recall method for the food diary may result in differences in individual recipes and missing foods. The researcher repeatedly emphasized how to impreve accuracy, including suggesting that researchers take pictures of meals and provide explanations using models of real food.

 XML Download
XML Download