

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
What started as a single robotic arm aiding in neurosurgical biopsy [1] more than 3 decades ago, technological advancement has produced sophisticated robotic surgery machines that have enabled surgeons to perform more challenging surgical procedures, broadening the indications of laparoscopic surgery. Robotic surgery has even become the preferred approach in selected gynecological and urological procedures [2], with emerging roles in the areas of otolaryngology, cardiothoracic, and gastrointestinal surgeries. In Korea, the robotic surgical system saw its first application in the general surgical field in 2005 after showing technical feasibility in cholecystectomy [3]. In 2008, robotic single-site surgery (RSSS) was introduced, with a single gel port accommodating multiple trocars for a camera, 2 arms, and an assist port [4]. The current robotic single-site surgical system was introduced in Korea in 2013 and was shown to be safe and feasible in robotic single-site cholecystectomy (RSSC) [567]. The da Vinci system has recently released a true single-port platform, the da Vinci SP system, with all the instruments entering into one single port [8].
We now present the first case of RSSC using the da Vinci SP system (RSPC), showing technical feasibility and discussing potential room for expanding indications in hepatobiliary and pancreatic surgery (HBP). This case report was approved by the Institutional Review Board (IRB) of Severance Hospital (4-2019-0185). Informed consent for using intraoperative images was waived by the IRB because it was regarded as anonymous clinical data.
CASE REPORT
Case presentation
A 59-year-old female presented with recurrent symptoms of biliary colic. At the time of consult, the patient was asymptomatic with soft and nontender abdomen. Preoperative abdominal ultrasound revealed gallstones with no signs of inflammation. To estimate severity of inflammatory changes around the gallbladder (GB) and to determine the case-specific appropriate surgical approach, contrast-enhanced CT scan of the abdomen was done and showed chronic calculus cholecystitis. There were no biliary obstructive symptoms based on clinical and laboratory examinations. WBC and CRP were normal.
Operating room set-up
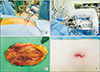
The patient was placed in a supine position, cleansed, and draped. The patient side cart (the robot part bearing the robotic arms) was positioned at the patient's head. A 2.5-cm vertical incision was made at the umbilicus. Due to absence of an access port for assistant surgeon's intervention, gauze, and the endobag were inserted and placed on the right upper abdomen upon entry into the peritoneum. The da Vinci single 2.5-cm trocar was inserted and connected to insufflation (Fig. 1A). The single port was then docked to the da Vinci SP patient side cart arm. The camera was inserted at the lower middle hole, a fenestrated bipolar forceps was placed at the left hole (arm 1), a cadiere forceps was placed at the upper-middle hole (arm 2), while the hook was placed on the right hole (arm 3) (Fig. 1B). Arm 1 was controlled by the left hand, arm 3 was controlled by the dominant right hand, while arm 2 was controlled interchangeably by right and left hand. It took 6 minutes for robotic docking.
Operative procedure
Supero-lateral traction of GB fundus was accomplished by arm 2 (Fig. 2A). Dissection commenced at the cystic plate with the left-hand grasper holding the Hartmann's pouch and the right-hand hook doing the diathermy. Critical view of safety was attained, cystic duct and artery, which were double clipped using hem-o-lock, was then divided (Fig. 2B, C). GB was dissected off its bed (Fig. 2D) then placed inside the endo-bag together with the gauze. Actual dissection time (time taken from starting dissection at Calot triangle to removing GB from liver bed [9]) was 15 minutes. After checking for hemostasis and bile leak, instruments were withdrawn, patient cart arm undocked, and the endo-bag containing the specimen pulled out together with the single-site port. The wound was closed in layers leaving a less than 2.5 cm wound (Fig. 1C). Console time was 15 minutes and the total operation time was 89 minutes. Estimated blood loss was minimal (<10 mL by definition in our institution). No bile leak or iatrogenic injury was encountered. Postoperative diagnosis was chronic cholecystitis with small GB stones based on surgical specimen (Fig. 1D).
Postoperative outcome
Postoperative course was unremarkable. Full diet was initiated upon full awakening. Numerical pain intensity score was 4/10 at immediate postoperative period (6 hours after surgery) and 2/10 on postoperative day 2, when the patient was discharged with oral pain killers as home medication.
DISCUSSION
To date, RSSS has been performed in different procedures including hysterectomies, prostatectomies, pancreatic surgeries, and cholecystectomies. As far as authors' knowledge, this experience is the first report to apply da Vinci SP robotic surgical system in general surgical field. The indication for robotic cholecystectomy is similar to the usual single-port laparoscopic cholecystectomy, however, we usually try to avoid acute and severe chronic cholecystitis to shorten operation time and enhancing procedural efficacy.
Table 1 summarizes the differences between the da Vinci SP system and its predecessors Si and Xi systems. One limitation of the Si/Xi RSSS of particular importance to cholecystectomy is the unidirectional retraction provided by the assist port. In RSSC, the tract in the gel port provided for the assistant port is oriented supero-medially, hence retraction of the GB fundus follows the same direction, making the triangle of Calot narrower. Although this has been addressed by the reversed-port technique [10], resulting in the ideal supero-lateral retraction of the GB fundus, retraction remains unidirectional. The availability of the third arm in the SP system enables retraction in all directions as required by the different phases of the operation and as per the surgeon's preference. An assistant surgeon is no longer required for retraction. Unlike in its multiport counterpart, Si/Xi single-port systems lack endowrist motion. In da Vinci SP, the endo-wrist motion was not only restored, but further improved via the multijoint (elbow and wrist) movement resulting in efficient distal triangulation. Distal triangulation provides a greater degree of freedom of movement, especially in narrow access areas. The improved degree of freedom is further complemented by better vision provided by the fully-wristed 3-dimensional high definition endoscope that can also easily convert from upside to downside view. In addition, the 3 arms and the endoscope in unison can rotate 360° around the umbilicus to reach difficult to reach areas. A new graphic user interface in the lower middle part of the display in the surgeon console shows real-time position and the relationship of the 4 instruments to each other (Fig. 2C).
The SP system has a much simpler docking process needing only to dock one trocar as compared to 3 trocars in the Si/Xi systems. Having 3 trocars, the Si/Xi single-port systems actually have 3 remote centers that just converge at one common area, the gel port, as compared to single remote center in the SP system's single trocar. Whether this difference can result in improved postoperative pain or not remains to be investigated in future studies. All 3 arms and endoscope in the SP system are oriented parallel to each other and are held by one major arm. This parallel orientation eliminates the potential arm clashing that is sometimes experienced in the Si/Xi systems.
One limitation of the SP system observed by the author is absence of an accessory port for fast and efficient delivery of needed materials (i.e., gauze, sutures, endo-bag). An accessory port is also important for immediate intervention by an assistant surgeon such as suctioning in cases of bile leak or bleeding. More complicated surgical procedures may not be considered without assistant surgeon's intervention. Technical modification such as addition of one laparoscopic trocar for assistant intervention maybe suitable for more complicated procedures.
Innovation always comes at a price. Individual instruments of the SP systems are more expensive as compared to the previous platforms. Hence, currently, RSPC may not be routinely done in clinical practice. The potential benefits over current laparoscopic single-port surgery and current robotic single-site surgery need to be further investigated based on accumulating experiences in well-selected patients.
When contemplating SP surgery in the field of HBP, SP configuration set-up needs to be kept in mind (Fig. 3). A precise distance from the system to the target organ needs to be considered due to the unique characteristics of the SP surgical system. The indication of da Vinci SP in HBP surgical field may still be limited. Potential applications can be in cases of pancreatic tumor enucleation, distal pancreatectomy, and some procedure requiring an intracorporeal suture-procedure. However, these potential applications of the SP system in the area of HBP still needs further study.
In conclusion, a single-site approach is not new to robotic surgical procedures. The SP robotic surgical system is basically a refinement of the predecessor SI and XI RSSS platforms. The present case suggests RSPC is technically feasible and safe with the new da Vinci SP system. Other new features are very promising in aiding in performing more challenging surgeries, especially in narrow access surgery.



 XML Download
XML Download