

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Neuroendocrine tumors (NETs) are rare neoplasms that mainly occur in the gastrointestinal system. The liver is the most common site of NET metastases, but it is a rare site of primary NETs [12]. Diagnosis of primary hepatic NET (PHNET) is based on 2 prerequisites: the liver mass must be immunohistochemically compatible with NET, and the liver should be the primary site of tumor development with strict exclusion of hepatic metastases from other locations. Differentiating between PHNET and liver metastasis from gastroenteropancreatic NETs is essential for accurate diagnosis of PHNETs. We aim to heighten our understanding of PHNET by retrospectively reviewing our surgical experiences with PHNET patients.
METHODS
During 10 years from January 1997 to December 2015, more than 15,000 patients underwent liver resection for various diseases in our institution. Of them, 35 patients were diagnosed with NET pathologically. To select PHNET study cases, we excluded 18 patients diagnosed with metastatic NET from other sites as well as 4 patients additionally diagnosed with NET from other gastroenteropancreatic sites 3 to 12 months later during postoperative follow-up up to 12 months. Ultimately, 13 patients were diagnosed with PHNET.
We reviewed the clinicopathological characteristics and prognosis in these 13 patients with PHNET. All patients were followed up regularly. We retrospectively obtained the clinical data from their medical records and followed them through December 2018 or patient death.
During the preoperative workup, patients underwent dynamic abdomino-pelvic CT, chest CT, endoscopic screening with gastroduodenoscopy and colonoscopy, somatostatin receptor scintigraphy, and PET-CT scan. Eleven patients underwent preoperative liver biopsy for differential diagnosis. Final pathologic diagnosis of PHNET was made after histopathological assessment and immunohistochemical staining.
This study was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Institutional Review Board of Asan Medical Center (2018-1508).
Numeric data were expressed as, mean ± standard deviation. Continuous numeric parameters were compared with the Student t-test. We used chi-square test and Fisher exact test for comparison of incidences. Survival curves were estimated using the Kaplan-Meier method. A P-value < 0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
Clinical findings
We analyzed the clinical findings of 13 patients (8 males and 5 females) with PHNET who underwent liver resection. The mean patient age was 51.1 ± 12.8 years (range, 26–70 years). The most common clinical manifestation was vague, nonspecific abdominal pain (n = 9). All patients were transferred to our institution after detection of a hepatic mass on imaging studies. The clinical profiles of these 13 patients are summarized in Table 1.
There were no noticeable abnormalities in biochemical liver function profiles or serological tumor markers; α-FP, CEA, and CA 19-9 were all within normal limits, except one patient with serum α-FP concentration of 95.3 ng/mL. HBV infection was diagnosed in 1 patient, but the other 12 patients showed no evidence of viral hepatitis.
Preoperative imaging findings
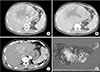
Dynamic liver CT was performed for detection of hepatic mass (Fig. 1). Every available diagnostic method was performed to identify the primary origin of the liver mass, including chest CT, MRI, gastroduodenoscopy, colonoscopy, bone scan, octreotide scintigraphy, and PET-CT scans. Small bowel series was also performed in one patient. These tests revealed no other sites suspected of origin of NET.
Two patients underwent somatostatin receptor scintigraphy, which showed no abnormal findings in one patient and a definite hepatic filling defect in another patient.
Eleven patients underwent percutaneous liver biopsies before surgical resection, which accurately diagnosed NET in 7 patients. The other 4 patients were misdiagnosed as hepatocellular carcinoma in 2, adenocarcinoma in 1, and benign hyperplasia in 1. Two patients underwent transarterial chemoembolization (TACE) before liver resection under the diagnosis of hepatocellular carcinoma.
Surgical treatment
Systematic hepatic resection was preferentially performed when the patient's general condition and functional hepatic reserves permitted. The extents of liver resection were right hepatectomy in 3, left hepatectomy in 3, right posterior sectionectomy in 2, central bisectionectomy in 2, left trisectionectomy in 1, left medial sectionectomy in 1, and left medial sectionectomy with caudate lobe resection in 1. Concurrent bile duct resection and biliary-enteric reconstruction were performed in 2 patients suspected of hilar bile duct invasion. One patient underwent portal vein thrombectomy, in whom the portal vein thrombus was also diagnosed as NET pathologically (Table 1).
There was no perioperative mortality or significant surgical complications. R0 resection was achieved in 10 patients, whereas the other 3 patients were regarded as having undergone R1 resection with tumor cell-positive hepatic resection margins.
Pathologic and immunohistochemical findings
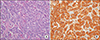
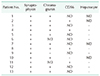
All patients had a single mass of 3.2–18 cm in the greatest diameter; mean and median diameters were estimated to be 9.6 ± 7.6 cm and 4.3 cm, respectively. NETs exhibit microscopic findings of insular, trabecular, or mixed patterns of cell growth (Fig. 2A). Immunohistochemical staining analysis showed positive staining for synaptophysin, chromogranin, and CD56 (Fig. 2B). Tables 2 and 3 summarize these histopathologic and immunohistochemical stain findings.
Treatment for tumor recurrence
Tumor recurrence occurred in 7 patients and 6 of these 7 recurrences developed at the remnant livers.
Since one patient (case number 3) showed multiple intrahepatic metastases with portal vein tumor thrombus after 13 months, systemic chemotherapy with etoposide and cisplatin was performed for 6 cycles, but tumor progressed. Thus, second chemotherapy with capecitabine and cisplatin was performed for 2 cycles, but it was discontinued due to serious adverse side-effects and tumor progression. Three patients (case numbers 7, 9, and 10) showing multiple intrahepatic metastasis underwent TACE with cisplatin repeatedly. One patient (case number 13) showed solitary intrahepatic metastasis at only one month after resection, thus the recurrent mass was treated with radiofrequency ablation. One patient (case number 6) showed retrocaval lymph node metastasis, thus external beam stereotactic radiotherapy was performed. One patient (case number 8) had multiple intrahepatic metastases at 2 months after resection, but any specific tumor treatment was not provided due to poor general condition and very rapid tumor progression.
Patient survival and risk factor analysis
The duration of follow-up periods ranged from 3 to 264 months (mean, 95.1 ± 86.6 months; median, 57 months). Seven of 13 patients suffered from tumor recurrence.
The 1-, 3-, and 5-year cumulative tumor recurrence rates were 30.8%, 47.3%, and 56.0%, respectively. When confined to R0 resections, the 1-, 3-, and 5-year recurrence rates were 20.0%, 31.4%, and 42.9%, respectively.
The 1-, 3-, 5-, and 10-year overall patient survival rates were 84.6%, 61.5%, 61.5%, and 61.5%, respectively. When confined to R0 resections, the 1-, 3-, 5-, and 10-year survival rates were 90.0%, 70.0%, 70.0%, and 70.0%, respectively (Fig. 3).
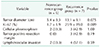
Univariate analysis showed that Ki-67 proliferative index was the only significant risk factor for tumor recurrence (Table 4).
DISCUSSION
Only 1%–2% of all gastrointestinal neoplasms are NETs, and most NETs detected in the liver are metastatic; thus, PHNET is very rare [123]. Diagnosing PHNET is considered challenging due to absence of specific symptoms and because the majority of hepatic NETs are metastatic liver lesions. Hepatic neuroendocrine cells can originate from intrahepatic bile duct epithelial cells, heterotopic pancreatic cells, or adrenal tissue [45]. PHNET can secrete various polypeptides and biogenic amines, including 5-hydroxytryptamine, pancreatic polypeptides, gastrin, prostaglandin, and calcitonin [36]. Clinically, only 5% of patients with carcinoid syndrome have obvious biological consequences such as skin flushing, asthma, and diarrhea [789]. Symptoms of epigastric discomfort, loss of appetite, fatigue, and weight loss are often present as the tumor enlarges. Patients with PHNET do not exhibit obvious carcinoid syndrome-related symptoms, whereas patients with hepatic metastatic NETs are associated with typical carcinoid syndrome-related symptoms. None of our patients in this study manifested carcinoid syndrome-related symptoms.
It is challenging to diagnose PHNET before surgery, in part because common hepatic tumor markers such as α-FP, CEA, CA19-9 are nondiagnostic in PHNET. Preoperative diagnosis of PHNET can be achieved by excluding primary extrahepatic lesions using imaging studies. To date, no PHNET-specific features have been reported using CT/MR imaging studies [1011121314], but a reliable diagnosis can be made using somatostatin receptor scintigraphy and PET-CT scan. Gastroscopy, colonoscopy, endoscopic ultrasound of the pancreas, video capsule endoscopy, and balloon enteroscopy are important examination methods to search for the primary site and exclude the possibility of liver metastasis from other sites [1516].
Somatostatin receptor scintigraphy is known to be useful in the diagnosis of NET as well as in detection of extrahepatic NET since the majority of these tumors express somatostatin [17]. 68Ga-labeled somatostatin analogs (68Ga-DOTA-SSAs) are becoming a useful primary diagnostic tool in NETs as evidenced by a growing number of reports detailing institutional experience with various DOTA peptides [18].
Of the 35 patients who were diagnosed pathologically with hepatic NET in this study, only 13 patients were ultimately diagnosed with NET of primary liver origin, and metastatic origins were identified in 22. We presume that there were many other patients with metastatic NET in their liver who did not undergo hepatic resection at our institution. Four patients had been initially diagnosed with PHNET at the time of surgery, but other NET lesions of the gastroenteropancreatic system were discovered within 12 months after initial hepatic resection. It is reasonable to consider such extrahepatic NET as the primary mass because there is a very low likelihood of metastasis from PHNET to the gastroenteropancreatic system. Thus, they were ultimately classified as metastatic liver NETs and therefore excluded from this study.
In this study, preoperative liver biopsy was performed in 11 of the 13 patients, and NET was accurately diagnosed in 7. Such a preoperative pathologic diagnosis of hepatic NET usually leads to the performance of additional studies to investigate the possibility of metastasis from other sites. Although preoperative percutaneous liver biopsy is useful for differential diagnosis, it does not appear to be essential to perform liver biopsy routinely in patients suspected of NET, considering that its diagnostic accuracy is not high enough and it can add some oncologic risk of tumor spread. If a liver mass appears to be malignant and its differential diagnosis is difficult, surgical resection often becomes the treatment of choice.
Immunohistochemical staining studies are valuable in the diagnosis of NETs. NET can be diagnosed by histopathologic assessment using hematoxylin-eosin staining, combined with immunohistochemical analysis using antibodies directed against synaptophysin, chromogranin, CD56, and other markers. We initially suspected that cellular pleomorphism might be associated with a worse outcome, but there was no correlation between pleomorphism and Ki67 staining or postoperative prognosis [19].
Ki67 is known as a marker of tumor proliferation, found to be a prognostic factor for various tumors [20]. Patients with malignant NET of the pancreas that have a Ki67 index of <2% have been reported to demonstrate a better prognosis than do patients with a Ki67 index of ≥2% [21]. In this study, Ki67 was a statistically significant prognostic factor for tumor recurrence, with a median value in the non-recurrent group of 1.7%.
Histopathological assessment alone cannot discern PHNET from metastatic NETs. Although a single NET lesion located in the liver has a possibility to be diagnosed with PHNET, a definitive diagnosis requires additional assessments, before, during and even after surgery, to exclude the possibility of metastasis from other sites. Extrahepatic gastroenteropancreatic NET can be inactive for a while; thus, strict follow-up studies are necessary for at least 1 year after resection of PHNET.
The primary treatment modality for PHNET is surgical resection of the tumor. In one study of 48 patients with PHNET, the 10-year survival rate after resection was 68% [22]; another study, with 58 cases of PHNET, reported an 80% 5-year survival rate after resection [23]. In this study, the 5-year and 10-year survival rates were 70.0% and 70.0% respectively in the 10 patients who underwent R0 resection. Liver transplantation can be considered for treatment of metastatic NET as well as for patients with PHNET [242526].
NETs are blood flow-rich tumors and sensitive to ischemia. Therefore, TACE can be used to treat a hypervascular mass in the liver, by which significant tumor size reduction can be achieved [272829]. In this study, a patient who had multiple intrahepatic recurrences after surgical resection were effectively treated by TACE repeatedly.
For intrahepatic tumor recurrence, it is usually recommended to perform repeat resection if indicated. Small solitary intrahepatic metastasis seems to be best indicated for repeat resection. Although 6 patients showed intrahepatic recurrence in this study, we did not perform repeat resection because 5 patients had multiple intrahepatic mass that were not indicated for resection. In addition, one patient had a single liver mass at only one month after resection, which implicated high possibility of further tumor recurrence, thus we decided to perform radiofrequency ablation instead of repeat resection.
In conclusion, PHNET is a very rare tumor with no specific clinical features. The final diagnosis of PHNET depends mainly on pathology and immunohistochemistry as well as exclusion of metastasis from other sites. Aggressive surgical treatment is highly recommended for patients with PHNET because of acceptably favorable postresection outcomes.



 XML Download
XML Download