

 PDF
PDF ePub
ePub Citation
Citation Print
Print


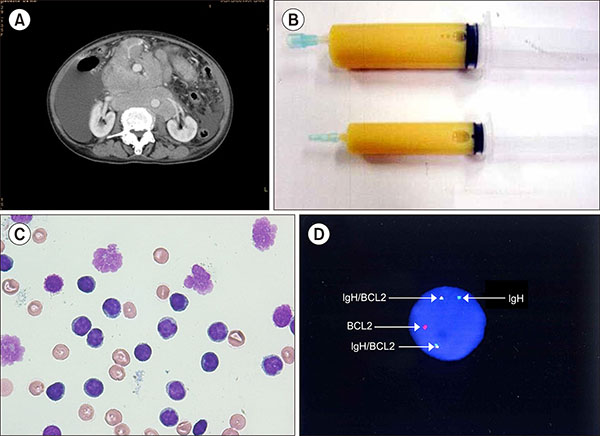
A 71-year-old woman was admitted to our hospital for further examination of massive ascites. The lactate dehydrogenase level was 230 IU/L, and the serum soluble interleukin-2 receptor level was 4,296 U/mL (reference range, 122–496 U/mL). Computed tomography revealed bilateral cervical and abdominal lymphadenopathy accompanied with massive ascites (A). Biopsy specimens obtained from cervical lymph nodes showed well-circumscribed follicles, with a monotonous population of lymphocytes, which was positive for CD10/20 and BCL2. Paracentesis revealed creamy opaque fluid (B), with elevated triglyceride (987 mg/dL), which is referred to as chylous ascites (CA). Cytological examination of CA showed lymphocytes with round nucleus and almost invisible cytoplasm and lymphocytes with lobulated nucleus and slightly visible cytoplasm (C). Flow cytometry showed many T lymphocytes expressing CD3/5 and a few B lymphocytes expressing CD10/20. Fluorescence in situ hybridization of CA confirmed IgH/BCL2 gene fusion (D). Based on these results, the patient was diagnosed with follicular lymphoma (FL) accompanied with CA, including a peritoneal lesion. Although ascites is common in lymphoma, CA is rare, and a few cases of FL accompanied with CA have been reported.
 XML Download
XML Download